

- Department of Neurosurgery, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
DOI:10.25259/SNI_562_2019
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Sunil Kumar Gupta, Ashish Aggarwal, Lomesh Wankhede. Elective inferior temporal lobe resection as an adjunct to subtemporal approach for a case of tentorial meningioma arising from the middle part of the free edge of the tentorium: A case report. 01-Aug-2020;11:215
How to cite this URL: Sunil Kumar Gupta, Ashish Aggarwal, Lomesh Wankhede. Elective inferior temporal lobe resection as an adjunct to subtemporal approach for a case of tentorial meningioma arising from the middle part of the free edge of the tentorium: A case report. 01-Aug-2020;11:215. Available from: https://surgicalneurologyint.com/surgicalint-articles/10167/
Date of Submission
17-Nov-2019
Date of Acceptance
17-Jul-2020
Date of Web Publication
01-Aug-2020
Abstract
Background: Tentorial meningiomas attached to the inner edge of the tentorium are difficult to excise due to their deep location. Sufficient space may not be always available through a subtemporal approach. Thus, the aim of not retracting the brain is not fulfilled.
Methods: To gain surgical corridor, we electively resected the inferior temporal lobe. This helped in greater working space, better visualization, and less chances of venous damage.
Results: Employing this technique of elective temporal lobe resection helped us in complete tumor removal without compromising on vision or surgical corridor.
Conclusion: A limited inferior temporal lobectomy greatly enhances the working space and vision in cases of difficult tentorial meningiomas. This translates into ease of tumor excision without compromising the patient safety.
Keywords: Free edge of tentorium, Inferior temporal lobe resection, Meningioma
INTRODUCTION
Large tentorial meningiomas arising from the free inner edge of the tentorium and compressing the brain stem are difficult to excise completely. The ideal surgical approach should allow early control of vascular supply of the tumor, avoid brain retraction and venous injury, and allow excision without any cranial nerve manipulation and injury.
We discuss here a case of tentorial meningioma arising from the free edge of the tentorium in its middle part which was excised completely through a subtemporal approach with addition of inferior temporal lobectomy.
CASE REPORT
A 50-year-old female presented with history of mild frontal headache, weakness of the left half of body, and numbness of the right side of face for 1 year. On examination, the patient had grade 4 power in the left upper and lower limb and 50% sensory loss in the distribution of the right 5th nerve. The rest of the neurological examination was unremarkable. Noncontrast computed tomography head [
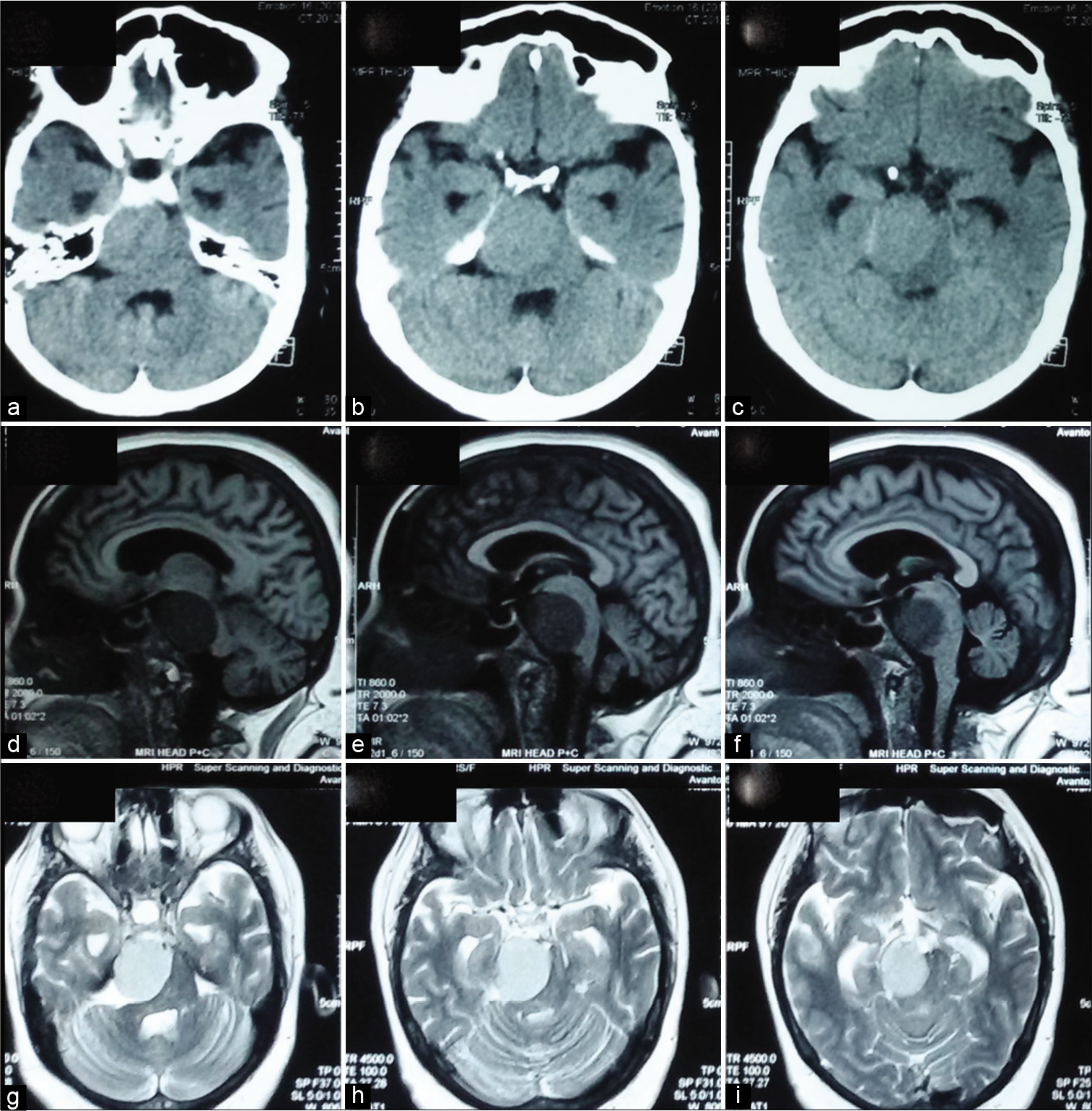
Figure 1:
(a-c) Axial noncontrast computed tomography head showing isointense tumor in the right incisural space causing distortion of the brain stem and producing mass effect. (d-f) Magnetic resonance imaging (MRI) T1WI sagittal section showing hypodense tumor anterolateral to the brain stem and posterior to clivus. (g-i) MRI T2WI axial section showing hyperintense tumor in the right incisural space causing distortion of the brain stem and producing mass effect.
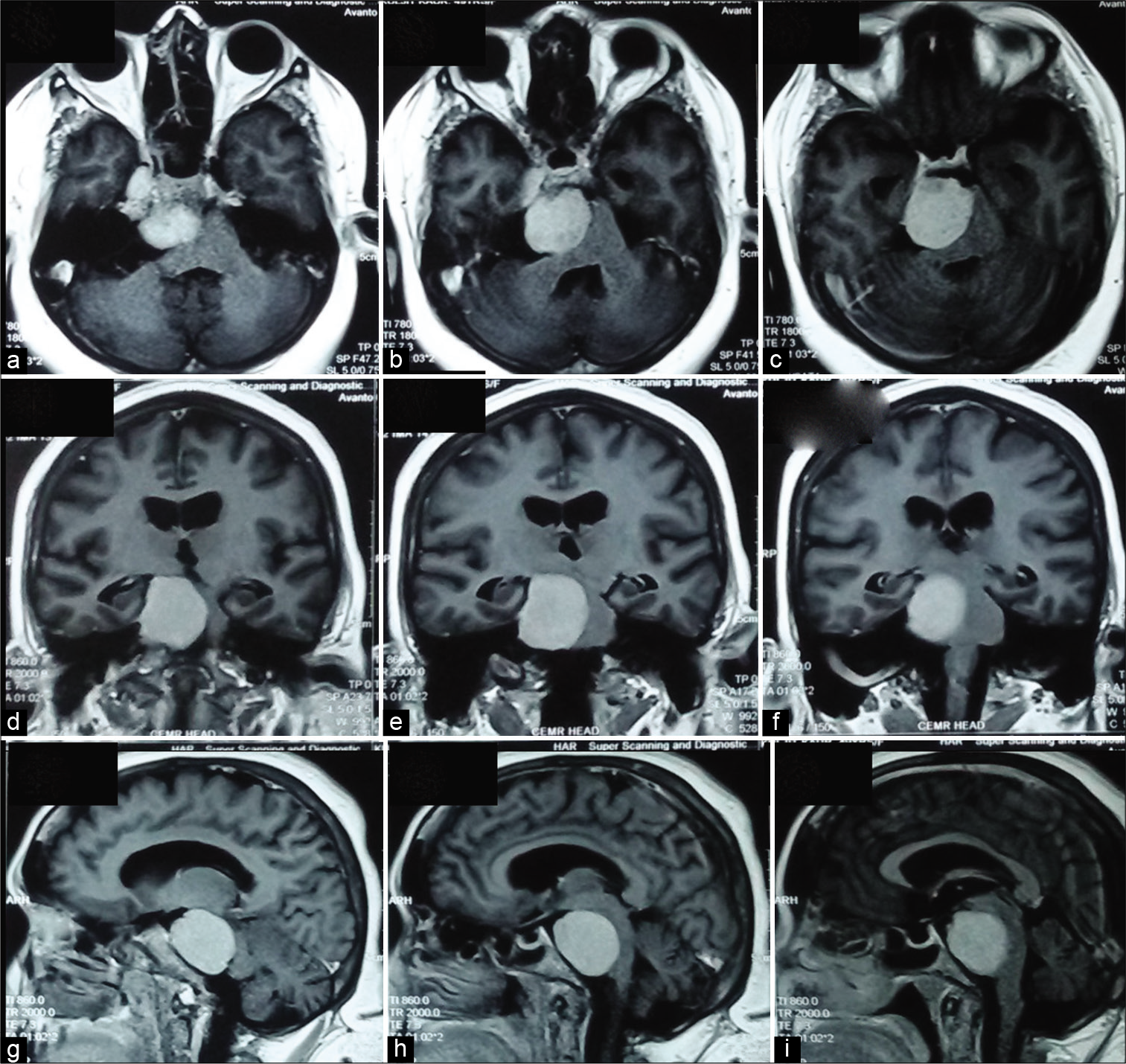
Figure 2:
(a-c) Contrast-enhanced magnetic resonance imaging (CEMRI) axial section showing contrast-enhancing lesion in the right incusral space causing mass effect on adjacent structures. (d-f) CEMRI coronal section showing tumor extending in the supra and infratentorial compartment and compressing medial part of temporal lobe and brain stem. (g-i) CEMRI sagittal section showing tumor anterolateral to the brain stem and posterior to clivus.
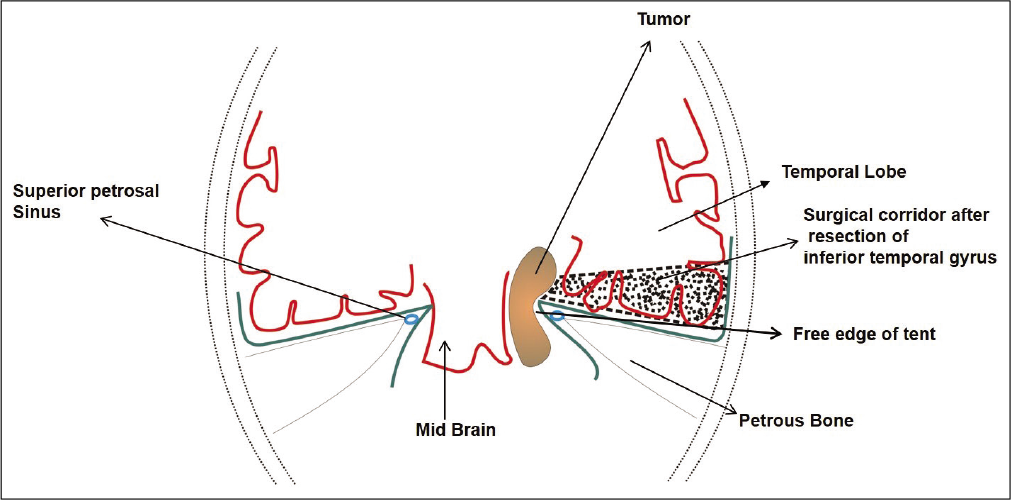
The tumor was approached initially by extradural subtemporal approach. The bone in the region of Kawase’s triangle was drilled, the dura was opened on the inferior medial temporal side and extended into the posterior fossa after ligating the superior petrosal sinus. The tentorium was sectioned. The tumor was firm, not easily suckable, and not even amenable to excision by cavitron ultrasonic surgical aspirator. In the limited corridor thus available, the excision of tumor became difficult as it involved the retraction of temporal lobe.
To gain space further, the inferior temporal lobe was electively resected. This maneuver remarkably improved the operative corridor and the tumor now could be resected completely without any temporal lobe retraction and without compromise of the vein of Labbe. The tumor was attached to the inner edge of the tentorium and had vascular supply from the tentorial branch of the meningohypophyseal trunk which was encountered and coagulated early in the course of excision. The V3 division of the 5th nerve and the Gasserian ganglion was severely compressed and partly encased by the tumor.
The patient had an uneventful postoperative course. Postoperative MRI brain [
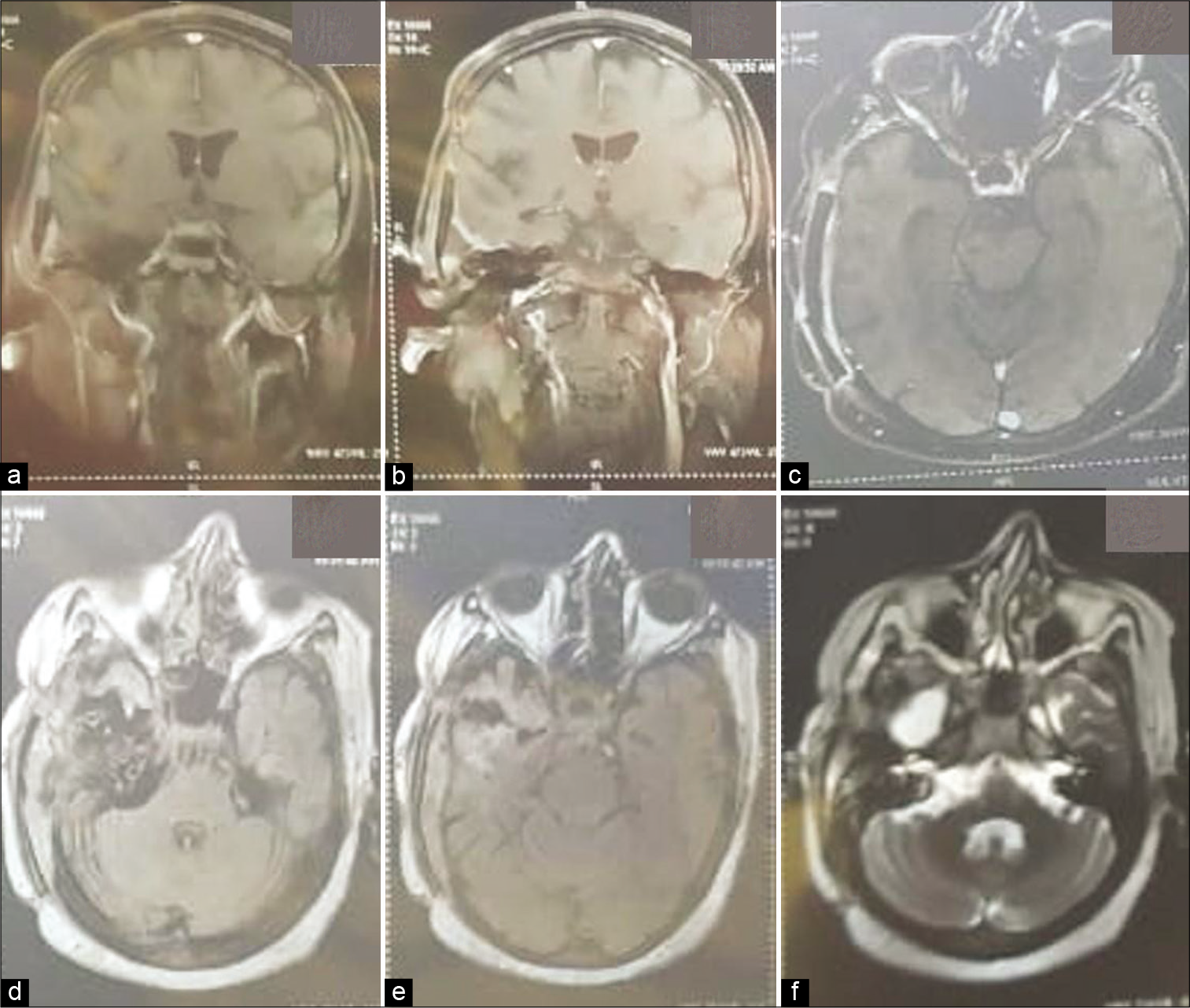
Figure 3:
(a and b) Contrast-enhanced magnetic resonance (CEMR) coronal T1WI showing area of encephalomalacia from where temporal lobe was partially excised. No tumor is visible. (c) CEMR axial T1WI showing complete tumor excision. (d and e) MR axial fluid-attenuated inversion recovery image showing area of temporal lobe excision. The surgical corridor is visible. (f) MR axial T2WI showing area of encephalomalacia in temporal lobe and complete tumor excision.
Relevant surgical anatomy
The free inner edge of the tentorium extends from the anterior clinoid process anteriorly to falcotentorial junction on each side. It is attached to the posterior clinoid process, petrous apex, and the anterior clinoid process forming the interclinoid, anterior petroclinoid, and posterior petroclinoid folds.[
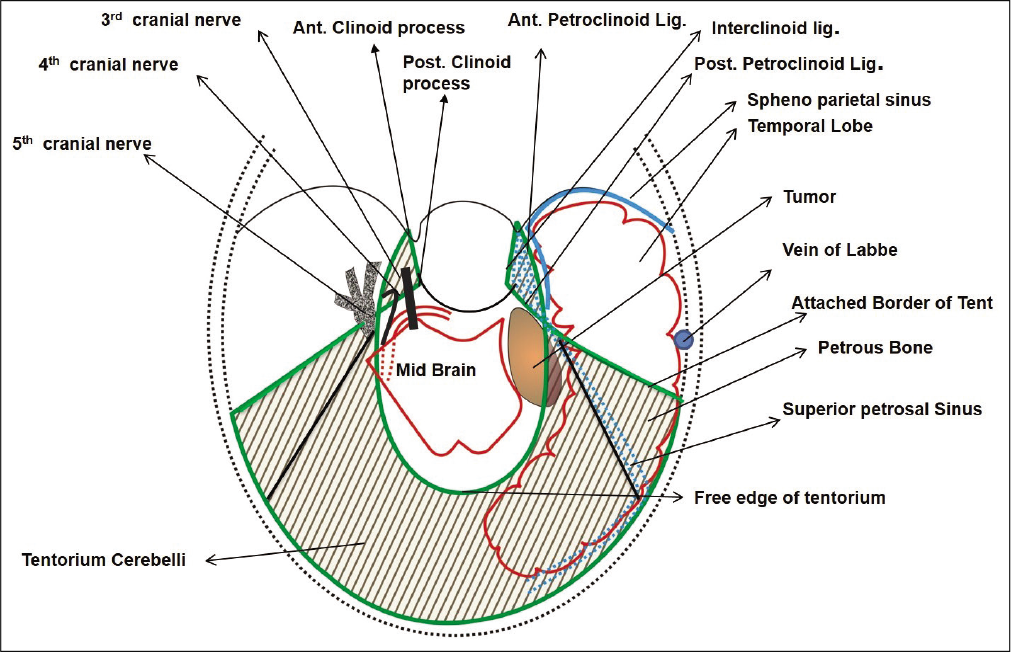
This knowledge of anatomy is helpful while sectioning the tentorium to gain access to the infratentorial tumor. The tentorium is cut from lateral to medial with the aim to section the tentorial edge posterior to the point where the fourth nerve comes in contact with it. Lateral to medial sectioning, with a continuous vision of the undersurface of the tentorium, is necessary to avoid inadvertent 4th nerve injury. The major vascular supply of the tentorial meningioma is from the tentorial artery. Sectioning and coagulating the tentorium helps to de vascularize the tumor.
The supraclinoid internal carotid artery may come into contact with tumors situated in the anterior incisural space and extending supratentorially. The arteries which are at risk during surgery for meningiomas of the middle tentorial edge are branches from the posterior communicating artery, anterior choroidal artery, and the posterior cerebral artery. The best way to avoid injury to these is not to breach the arachnoid and remain extra-arachnoidal, especially on the medial aspect of the tumor. The most important venous structure is the vein of Labbe which is likely to be damaged if there is significant subtemporal retraction. The surgeon should also be aware of the venous anatomy of the floor of the middle fossa. Apart from veins from the undersurface of the temporal lobe, there may be large venous sinuses in the dural leaves of the middle fossa. The cavernous sinus can also be accidentally injured during tentorial sectioning if the incision is too close to petrous apex. Identification of the Gasserian ganglion and the V3 division of the 5th nerve and the superior petrosal sinus is necessary before the tentorial section. The basal vein of Rosenthal lies on the medial aspect of the tumor and is best preserved if the surgeon takes care not to breach the arachnoid.
DISCUSSION
Meningiomas arising from the medial or inner edge of the tentorium and occupying the tentorial incisural space are a surgical challenge. The intended approach is decided taking into consideration the location of meningioma (in relation to anterior, middle, or posterior incisural space), the size of the tumor, and the degree of supra and infratentorial extension.
Yasargil’s classification of tentorial meningiomas is the most comprehensive and practical one for deciding the surgical approach. As per that classification, the present case was type 2 tentorial meningioma, that is, anterolateral.[
In our opinion, tumors such as the present case should be approached by a subtemporal route. However, in few situations, the exposure is limited in spite of adequate middle cranial fossa base drilling. In addition, tumor may be hard and unsuckable. In these desperate situations, an intradural route with elective partial inferior temporal lobectomy may be employed. The addition of inferior temporal lobectomy avoids temporal lobe retraction and inadvertent injury to the vein of Labbe. Lee et al. have described a “trans zygomatic approach with anteriorly limited inferior temporal gyrectomy” for large medial tentorial meningiomas.[
We feel that a limited inferior temporal lobectomy greatly enhances the surgeons view and working space and obviates the need for any additional bony work. This may also have an additional benefit of avoidance of postoperative CSF leak.
CONCLUSION
Large tumors of the middle incisural space in few select cases may be exposed by a subtemporal transtentorial approach with elective partial resection of the inferior temporal lobe, in situations when the operative corridor is found to be restrictive. This may be better than excessive temporal lobe retraction with the consequent risk of venous injury.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Publication of this article was made possible by the James I. and Carolyn R. Ausman Educational Foundation.
Conflicts of interest
There are no conflicts of interest.
References
1. Ansari SF, Young RL, Bohnstedt BN, Cohen-Gadol AA. The extended supracerebellar transtentorial approach for resection of medial tentorial meningiomas. Surg Neurol Int. 2014. 5: 35
2. Gupta SK. Trans-sylvian transtentorial approach for skull base lesions extending from the middle fossa to the upper petro-clival region. Br J Neurosurg. 2009. 23: 287-92
3. Gupta T, Gupta SK, Sahni D. Anatomy of the tentorial segment of the trochlear nerve in reference to its preservation during surgery for skull base lesions. Surg Radiol Anat. 2014. 36: 967-71
4. Hashemi M, Schick U, Hassler W, Hefti M. Tentorial meningiomas with special aspect to the tentorial fold: Management, surgical technique, and outcome. Acta Neurochir (Wien). 2010. 152: 827-34
5. Hayashi N, Kurimoto M, Nagai S, Sato H, Hori S, Endo S. Tentorial incision in a lateral-medial direction with minimal retraction of the temporal lobe in the subtemporal transtentorial approach to the middle tentorial incisural space. Minim Invasive Neurosurg. 2008. 51: 340-4
6. Lee EJ, Park ES, Cho YH, Hong SH, Kim JH, Kim CJ. Transzygomatic approach with anteriorly limited inferior temporal gyrectomy for large medial tentorial meningiomas. Acta Neurochir (Wien). 2015. 157: 1747-55
7. Shukla D, Behari S, Jaiswal AK, Banerji D, Tyagi I, Jain VK. Tentorial meningiomas: Operative nuances and perioperative management dilemmas. Acta Neurochir (Wien). 2009. 151: 1037-51

