

- Department of Neurosurgery The University of Texas at Austin Dell Medical School, Austin, Texas, United States.
- Department of Diagnostic Medicine, The University of Texas at Austin Dell Medical School, Austin, Texas, United States.
Correspondence Address:
Ramsey Ashour
Department of Neurosurgery, The University of Texas at Austin Dell Medical School, Austin, Texas, United States.
DOI:10.25259/SNI_611_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Akhil Surapaneni1, John Kuo1, Min Wang1, Ramsey Ashour2. Epidermoid cyst in a patient with Alagille syndrome: Coincidence or connection?. 11-Dec-2020;11:432
How to cite this URL: Akhil Surapaneni1, John Kuo1, Min Wang1, Ramsey Ashour2. Epidermoid cyst in a patient with Alagille syndrome: Coincidence or connection?. 11-Dec-2020;11:432. Available from: https://surgicalneurologyint.com/surgicalint-articles/10444/
Date of Submission
06-Sep-2020
Date of Acceptance
28-Nov-2020
Date of Web Publication
11-Dec-2020
Abstract
Background: Alagille syndrome is a rare genetic syndrome, which arises due to defects in the Notch signaling pathway, resulting in liver, cardiopulmonary, renal, skeletal, and ophthalmologic problems, among others. Epidermoid cysts are rare congenital benign lesions that develop from ectopic ectodermal cell rests formed during neurulation.
Case Description: A 24-year-old Alagille syndrome patient presented with hearing loss and was found to have a sizable posterior fossa mass. He underwent craniotomy for uneventful resection of the lesion, which was found to be an epidermoid cyst.
Conclusion: While our case may represent a coincidental occurrence of two pathologies presenting together, given that epidermoid cysts arise from aberrant neurulation, and in light of the crucial role of the Notch signaling pathway both in normal neurogenesis and in the pathogenesis of Alagille syndrome, we hypothesize a possible association between these entities.
Keywords: Alagille syndrome, Epidermoid cyst, Notch signaling
INTRODUCTION
Alagille syndrome[
CASE REPORT
History
A 24-year-old male with established Alagille syndrome, complicated by hemodialysis-dependent end-stage renal disease and liver cirrhosis, presented with an 8-month history of headaches and hearing loss (right worse than left). Brain magnetic resonance imaging (MRI) revealed a 3 cm, extra-axial, diffusion restricting, posterior fossa mass involving the right temporal bone posterior to the mastoid air cells, invading and occluding the transverse/sigmoid sinuses, and distorting the cerebellum [
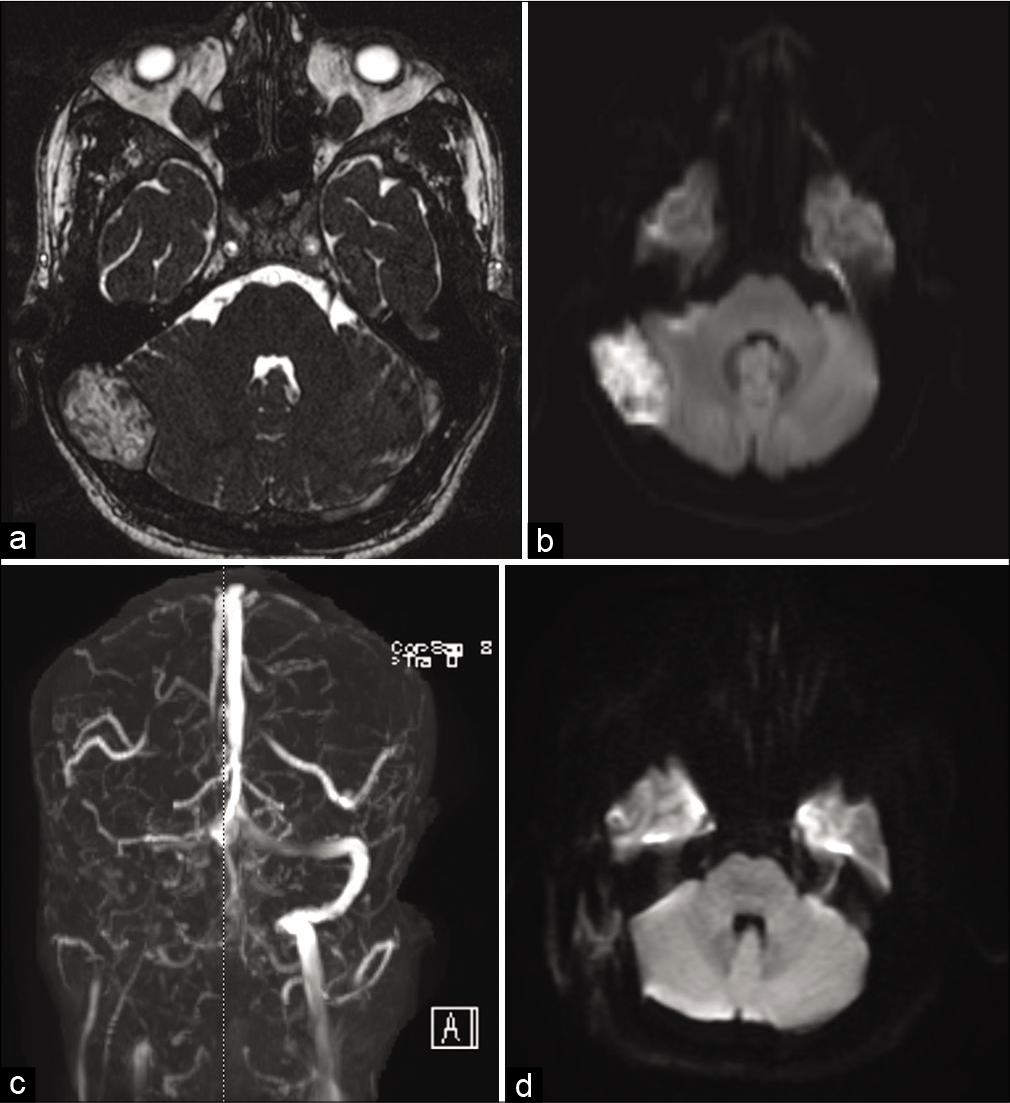
Figure 1:
Preoperative (a) T2 magnetic resonance imaging (MRI), (b) diffusion-weighted imaging (DWI) MRI, and (c) magnetic resonance venography demonstrating right posterior fossa mass causing transverse sigmoid sinus occlusion with cerebellar distortion. (d) Postoperative DWI MRI showing resection of the mass.
Procedure
A C-shaped retroauricular incision was made, and the underlying muscle and fascia were reflected to expose the retromastoid region. Drilling was performed to create a quarter-sized retrosigmoid craniotomy; then, dissection under the operating microscope showed an epidural white keratinizing pearly lesion displacing the cerebellum inferomedially. Samples of the lesion were removed and sent for pathological analysis. The lesion was hypovascular and removed completely with suction and microdissection to carefully elevate the capsule of the lesion from the dura. The exposed mastoid air cells were covered with muscle grafts and oxidized cellulose along the superior and anterior aspects. The lesion was further resected to the occluded transverse and sigmoid sinuses, which were filled with thrombus. The surrounding bone was thoroughly curetted, and the surgical cavity was copiously irrigated, then carefully inspected to confirm the absence of gross residual disease. A small myofascial free tissue graft was placed over the resection cavity. There were multiple small rents in the dura, which were covered with a synthetic dural graft. A titanium mesh was used to cover the entire craniectomy defect. The fascia and skin were closed in standard fashion.
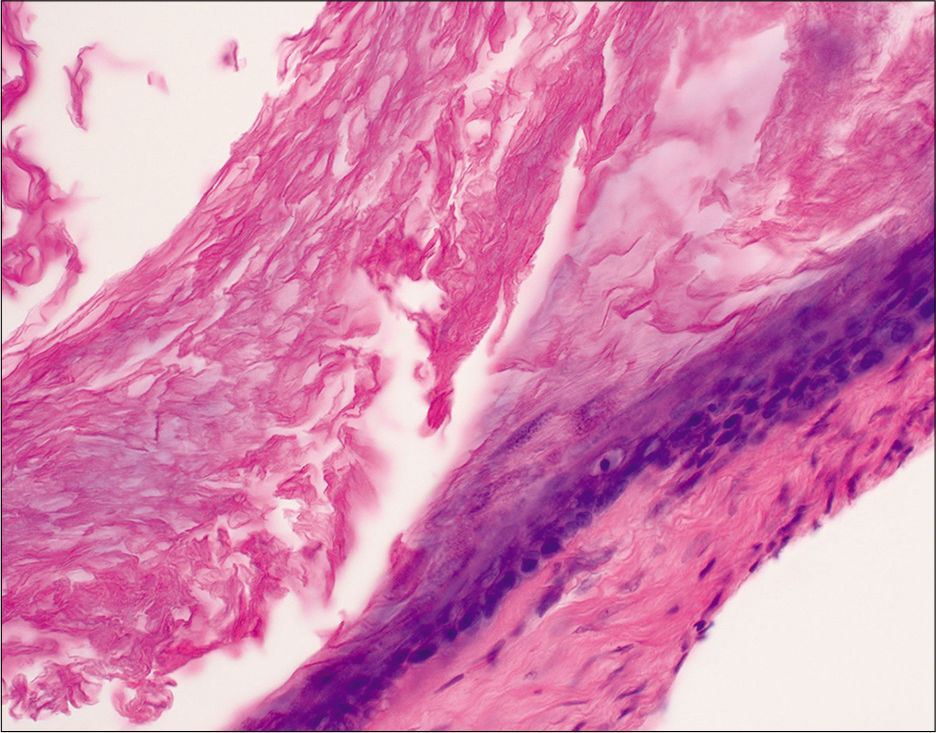
Pathology
On microscopic examination, permanent sections showed multiple portions of tumor wall containing acellular keratin debris. The tumor was lined by keratinizing stratified squamous epithelium with a granular layer. This was most consistent with an epidermal inclusion cyst with dystrophic calcification [
Postoperative course
Postoperative brain MRI demonstrated gross total resection of the lesion. Postoperatively, he received hemodialysis while hospitalized and was quickly weaned off of steroids and restarted on his home antihypertensive medications. He made an uneventful recovery and was discharged on postoperative day 3, and was doing well when evaluated at 3 months postoperatively.
DISCUSSION
In this report, we highlight the case of a young man with two uncommon conditions: Alagille syndrome and a posterior fossa epidermoid cyst. Based on a review of the literature, we hypothesize that the importance of Notch signaling in neural tube development and in the pathogenesis of Alagille syndrome may implicate a role for this signaling pathway in the pathogenesis of epidermoid cysts as well.
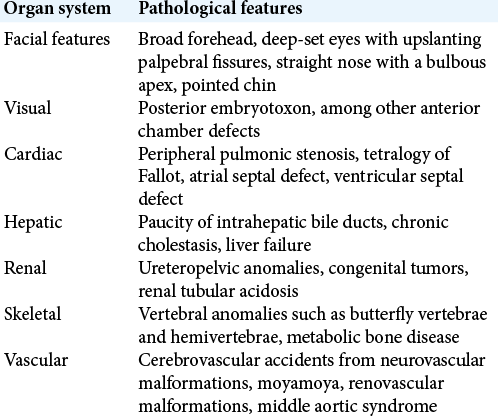
Alagille syndrome
Alagille syndrome is a genetic disorder, transmitted in an autosomal dominant fashion, characterized by liver, heart, lung, kidney, skeletal, and eye problems, among others.[
Epidermoid cysts
Epidermoid cysts develop from displaced ectodermal cell rests that become trapped in the neural tube during closure. These lesions grow over time by accumulating keratin and cholesterol, which are breakdown products from desquamating epithelial cells and give it a characteristic pearly appearance. Within the cranium, they have a predisposition for the cerebellopontine angle and the parasellar region.[
Notch signaling
The Notch signaling system is a highly conserved developmental signaling pathway in many tissues, organisms, and diseases. It plays important roles in cell fate determination and differentiation.[
CONCLUSION
While our case may represent a coincidental occurrence of two pathologies presenting together, given that epidermoid cysts arise from aberrant neurulation, and in light of the crucial role of the Notch signaling pathway both in normal neurogenesis and in the pathogenesis of Alagille syndrome, we hypothesize a possible association between these entities. This report may prove useful for heightened clinical awareness for epidermoid cysts in Alagille syndrome patients.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alagille D, Odièvre M, Gautier M, Dommergues JP. Hepatic ductular hypoplasia associated with characteristic facies, vertebral malformations, retarded physical, mental, and sexual development, and cardiac murmur. J Pediatr. 1975. 86: 63-71
2. Andersson ER, Sandberg R, Lendahl U. Notch signaling: Simplicity in design, versatility in function. Development. 2011. 138: 3593-612
3. Berger MS, Wilson CB. Epidermoid cysts of the posterior fossa. J Neurosurg. 1985. 62: 214-9
4. Conlon RA, Reaume AG, Rossant J. Notch1 is required for the coordinate segmentation of somites. Development. 1995. 121: 1533-45
5. Dunwoodie SL, Clements M, Sparrow DB, Sa X, Conlon RA, Beddington RS. Axial skeletal defects caused by mutation in the spondylocostal dysplasia/pudgy gene Dll3 are associated with disruption of the segmentation clock within the presomitic mesoderm. Development. 2002. 129: 1795-806
6. Eekhof JL, Thomeer RT, Bots GT. Epidermoid tumor in the lateral ventricle. Surg Neurol. 1985. 23: 189-92
7. Emerick KM, Rand EB, Goldmuntz E, Krantz ID, Spinner NB, Piccoli DA. Features of Alagille syndrome in 92 patients: Frequency and relation to prognosis. Hepatology. 1999. 29: 822-9
8. Goldman SA, Gandy SE. Squamous cell carcinoma as a late complication of intracerebroventricular epidermoid cyst. Case report. J Neurosurg. 1987. 66: 618-20
9. Henrique D, Adam J, Myat A, Chitnis A, Lewis J, IshHorowicz D. Expression of a Delta homologue in prospective neurons in the chick. Nature. 1995. 375: 787-90
10. Herreman A, Hartmann D, Annaert W, Saftig P, Craessaerts K, Serneels L. Presenilin 2 deficiency causes a mild pulmonary phenotype and no changes in amyloid precursor protein processing but enhances the embryonic lethal phenotype of presenilin 1 deficiency. Proc Natl Acad Sci U S A. 1999. 96: 11872-7
11. Huppert SS, Le A, Schroeter EH, Mumm JS, Saxena MT, Milner LA. Embryonic lethality in mice homozygous for a processing-deficient allele of Notch1. Nature. 2000. 405: 966-70
12. Kamath BM, Baker A, Houwen R, Todorova L, Kerkar N. Systematic review: The epidemiology, natural history, and burden of Alagille syndrome. J Pediatr Gastroenterol Nutr. 2018. 67: 148-56
13. Kiernan AE, Ahituv N, Fuchs H, Balling R, Avraham KB, Steel KP. The Notch ligand Jagged1 is required for inner ear sensory development. Proc Natl Acad Sci U S A. 2001. 98: 3873-8
14. Li T, Ma G, Cai H, Price DL, Wong PC. Nicastrin is required for assembly of Presenilin/gamma-secretase complexes to mediate notch signaling and for processing and trafficking of beta-amyloid precursor protein in mammals. J Neurosci. 2003. 23: 3272-7
15. Main H, Radenkovic J, Jin S, Lendahl U, Andersson ER. Notch signaling maintains neural rosette polarity. PLoS One. 2013. 8: e62959
16. Massarwa R, Ray HJ, Niswander L. Morphogenetic movements in the neural plate and neural tube: Mouse. Wiley Interdiscip Rev Dev Biol. 2014. 3: 59-68
17. McDaniell R, Warthen DM, Sanchez-Lara PA, Pai A, Krantz ID, Piccoli DA. NOTCH2 mutations cause Alagille syndrome, a heterogeneous disorder of the notch signaling pathway. Am J Hum Genet. 2006. 79: 169-73
18. Netsky MG. Epidermoid tumors, Review of the literature. Surg Neurol. 1988. 29: 477-83
19. Oda T, Elkahloun AG, Pike BL, Okajima K, Krantz ID, Genin A. Mutations in the human Jagged1 gene are responsible for Alagille syndrome. Nat Genet. 1997. 16: 235-42
20. Patibandla MR, Yerramneni VK, Mudumba VS, Manisha N, Addagada GC. Brainstem epidermoid cyst: An update. Asian J Neurosurg. 2016. 11: 194-200
21. Roebroek AJ, Umans L, Pauli IG, Robertson EJ, van Leuven F, van de Ven WJ. Failure of ventral closure and axial rotation in embryos lacking the proprotein convertase Furin. Development. 1998. 125: 4863-76
22. Schwartz JF, Balentine JD. Recurrent meningitis due to an intracranial epidermoid. Neurology. 1978. 28: 124-9
23. Shi S, Stanley P. Protein O-fucosyltransferase 1 is an essential component of Notch signaling pathways. Proc Natl Acad Sci U S A. 2003. 100: 5234-9
24. Tanabe Y, Jessell TM. Diversity and pattern in the developing spinal cord. Science. 1996. 274: 1115-23
25. Tancredi A, Fiume D, Gazzeri G. Epidermoid cysts of the fourth ventricle: Very long follow up in 9 cases and review of the literature. Acta Neurochir (Wien). 2003. 145: 905-10
26. Turnpenny PD, Ellard S. Alagille syndrome: Pathogenesis, diagnosis and management. Eur J Hum Genet. 2012. 20: 251-7
27. Yamakawa K, Shitara N, Genka S, Manaka S, Takakura K. Clinical course and surgical prognosis of 33 cases of intracranial epidermoid tumors. Neurosurgery. 1989. 24: 568-73
28. Yaşargil MG, Abernathey CD, Sarioglu AC. Microneurosurgical treatment of intracranial dermoid and epidermoid tumors. Neurosurgery. 1989. 24: 561-7

