

- Departments of Spine, Kokilaben Dhirubhai Ambani Hospital, Mumbai, Maharashtra, India.
- Departments of Pathology, Kokilaben Dhirubhai Ambani Hospital, Mumbai, Maharashtra, India.
- Departments of Ear, Nose and Throat, Kokilaben Dhirubhai Ambani Hospital, Mumbai, Maharashtra, India.
- Radiodiagnosis, Kokilaben Dhirubhai Ambani Hospital, Mumbai, Maharashtra, India.
Correspondence Address:
Rajendra Sakhrekar
Departments of Spine, Kokilaben Dhirubhai Ambani Hospital, Mumbai, Maharashtra, India.
DOI:10.25259/SNI_317_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Rajendra Sakhrekar, Vishal Peshattiwar, Ravikant Jadhav, Bijal Kulkarni, Sanjiv Badhwar, Hrishikesh Kale, Rammohan Yedave. Extremely rare case of retropharyngeal space benign plexiform schwannoma - Excised through Smith- Robinson Approach. 11-Jul-2020;11:182
How to cite this URL: Rajendra Sakhrekar, Vishal Peshattiwar, Ravikant Jadhav, Bijal Kulkarni, Sanjiv Badhwar, Hrishikesh Kale, Rammohan Yedave. Extremely rare case of retropharyngeal space benign plexiform schwannoma - Excised through Smith- Robinson Approach. 11-Jul-2020;11:182. Available from: https://surgicalneurologyint.com/surgicalint-articles/10124/
Date of Submission
27-May-2020
Date of Acceptance
16-Jun-2020
Date of Web Publication
11-Jul-2020
Abstract
Background: Approximately 25–45% of schwannomas are typically slow-growing, encapsulated, and noninvasive tumors that occur in the head-and-neck region where they rarely involve the retropharyngeal space. Here, we report deep-seated benign plexiform schwannoma located in the retropharyngeal C2-C5 region excised utilizing the Smith-Robinson approach.
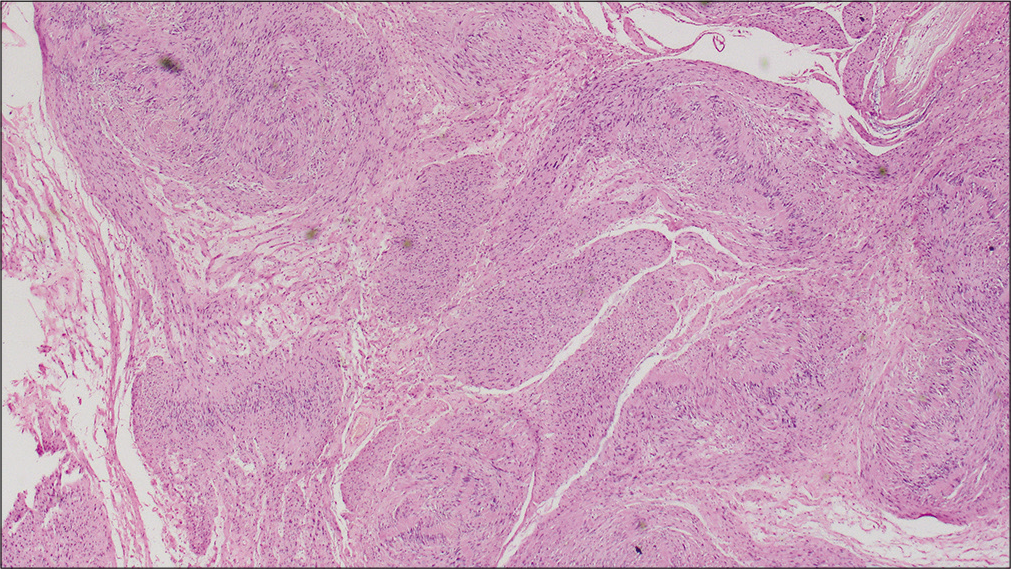
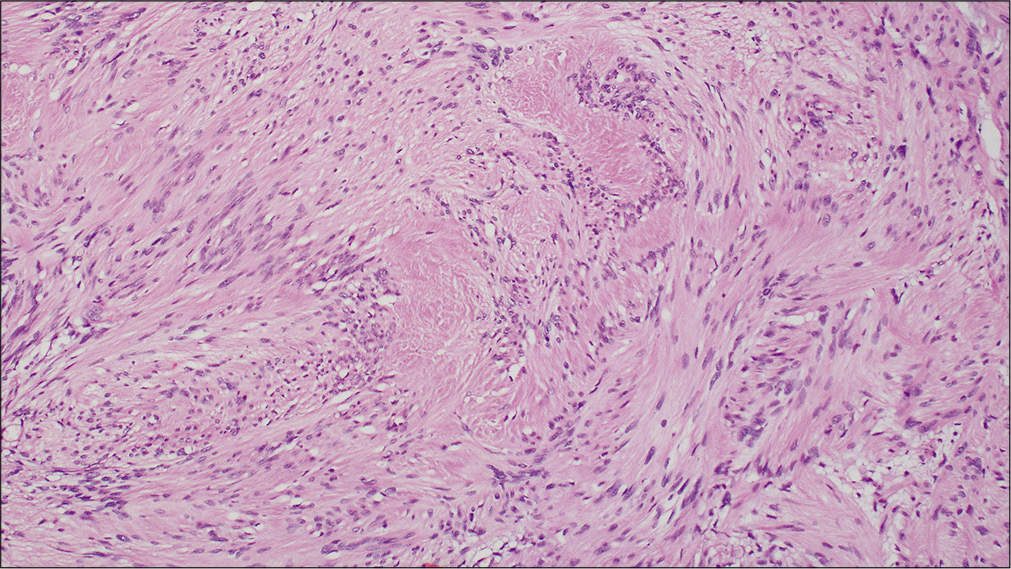
Case Description: A 30-year-old male presented with dysphagia and impaired phonation attributed to an MR documented C2-C5 retropharyngeal schwannomas. On examination, the lesion was soft, deep seated, and extended more toward the right side of the neck. Utilizing a right-sided Smith-Robinson’s approach, it was successfully removed. The histopathology confirmed the diagnosis of a plexiform schwannoma.
Conclusion: Retropharyngeal benign plexiform schwannomas are rare causes of dysphagia/impaired phonation in the cervical spine. MR studies best document the size and extent of these tumors which may be readily resected utilizing a Smith-Robinson approach.
Keywords: Benign plexiform schwannoma, Dysphagia, Dysphonia, Retropharyngeal space, Smith-Robinson’s approach
INTRODUCTION
Approximately 25–45% of schwannomas are found in the head-and-neck region, but rarely involve the retropharyngeal space.[
CASE PRESENTATION
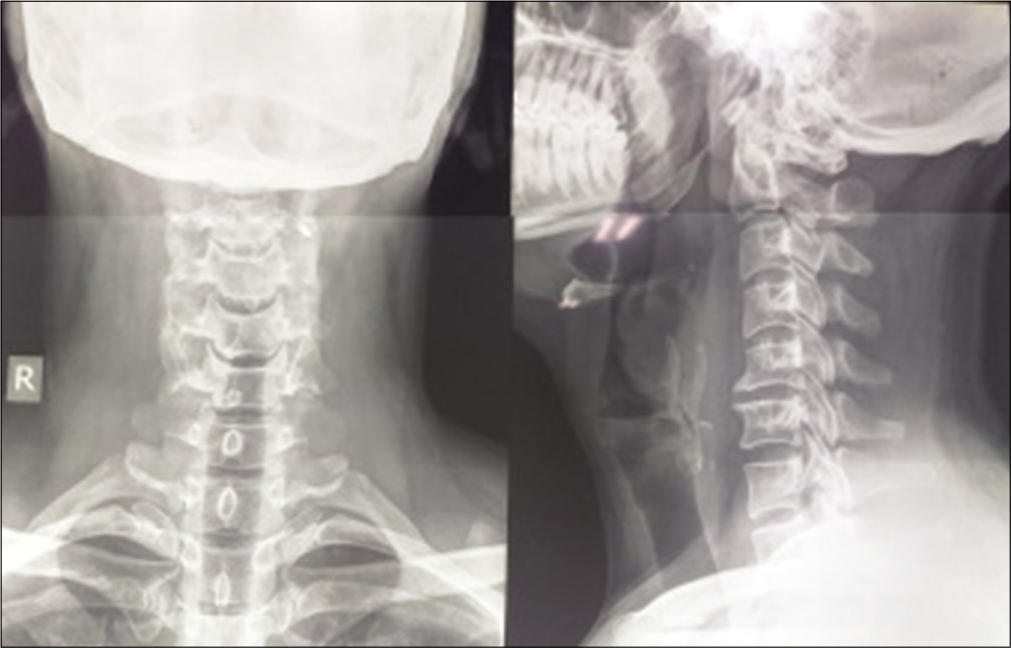
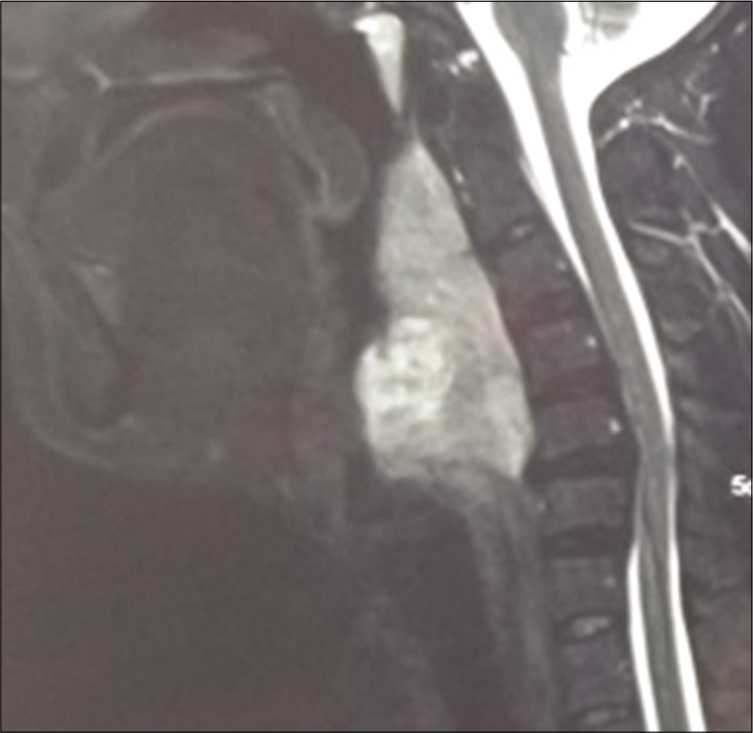
A 30-year-old male was admitted with a 1-year history of feeling a “lump in the throat,” accompanied by impaired phonation, snoring, and increasing difficulty swallowing. On examination, a deep soft-tissue swelling right-sided swelling could be palpated. While plain X-rays showed scalloping of the C5 vertebral body, magnetic resonance imaging (MRI) demonstrated a large lobulated retropharyngeal mass (7.5 cm craniocaudal × 4.8 cm transverse 4.8 cm × 3.1 cm AP) compressing the upper airway (i.e., oropharynx and hypopharynx) [




DISCUSSION
Retropharyngeal schwannomas are exceptionally rare. Raimondo et al. in 2015 reported a posterior pharyngeal wall plexiform schwannomas.[
Diagnostic studies
The contrast-enhanced CT scans and MRI scans readily established the diagnosis of the retropharyngeal schwannoma. On enhanced MRI, these lesions are best demonstrated as well capsulated tumors.[
Surgery
Gross total surgical excision is the treatment of choice for schwannomas. Observation or incomplete tumor excision can lead to malignant transformation.[
Outcomes
Bozza et al. and Gallo et al. noted good prognoses associated with the gross total resection of encapsulated schwannomas. Only rarely do these lesions recur or undergo malignant transformation.[
CONCLUSION
Retropharyngeal benign plexiform schwannomas are rare, but can be readily diagnosed utilizing contrasted enhanced MR scans. The optimal surgical choice for these lesions is gross total excision that was readily accomplished in this case for the C2-C5 tumor utilizing an anterior cervical Smith- Robinson approach.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bozza F, Vigili M, Ruscito P, Marzetti A, Marzetti F. Surgical management of parapharyngeal space tumours: Results of 10-year follow-up. Acta Otorhinolaryngol Ital. 2009. 29: 10-5
2. Colreavy M, Lacy P, Hughes J, Bouchier-Hayes D, Brennan P, O’Dwyer A. Head and neck schwannomas-a 10 year review. J Laryngol Otol. 2000. 114: 119-24
3. Gallo S, Bandi F, Maffioli MP, Giudice M, Castelnuovo P, Fazio E. Retropharyngeal space schwannoma: A rare entity. Iran J Otorhinolaryngol. 2017. 29: 353-7
4. Giraddi G, Vanaki SS, Puranik R. Schwannoma of parapharyngeal space. J Maxillofac Oral Surg. 2010. 9: 182-5
5. Huang CM, Leu YS. Schwannoma of the posterior pharyngeal wall. J Laryngol Otol. 2002. 116: 740-1
6. Ijichi K, Muto M, Masaki A, Murakami S. Recurrent plexiform schwannoma involving the carotid canal. Auris Nasus Larynx. 2018. 45: 358-61
7. Khafif A, Segev Y, Kaplan DM, Gil Z, Fliss DM. Surgical management of parapharyngeal space tumors: A 10-year review. Otolaryngol Head Neck Surg. 2005. 132: 401-6
8. Kim SH, Kim NH, Kim KR, Lee JH, Choi HS. Schwannoma in head and neck: Preoperative imaging study and intracapsular enucleation for functional nerve preservation. Yonsei Med J. 2010. 51: 938-42
9. Moukarbel RV, Sabri AN. Current management of head and neck schwannomas. Curr Opin Otolaryngol Head Neck Surg. 2005. 13: 117-22
10. Raimondo L, Garzaro M, Mazibrada J, Pecorari G, Giordano C. Plexiform schwannoma of the posterior pharyngeal wall in a patient with neurofibromatosis 2. Ear Nose Throat J. 2015. 94: E17-9

