

- Neurosurgery Department, Centro Médico “Lic. Adolfo López Mateos”, Instituto de Salud del Estado de México, Av. Nicolas San Juan s/n Ex Hacienda La Magdalena, Estado de México, México
Correspondence Address:
A. Ceja-Espinosa
Neurosurgery Department, Centro Médico “Lic. Adolfo López Mateos”, Instituto de Salud del Estado de México, Av. Nicolas San Juan s/n Ex Hacienda La Magdalena, Estado de México, México
DOI:10.4103/sni.sni_251_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: A. Ceja-Espinosa, J. A. Franco-Jiménez, A. Sosa-Nájera, G. A. Gutiérrez-Aceves, M. I. Ruiz-Flores. Fourth ventricle neurocysticercosis: Rigid endoscopic management. Description of direct transcerebellar approach. 26-Sep-2017;8:232
How to cite this URL: A. Ceja-Espinosa, J. A. Franco-Jiménez, A. Sosa-Nájera, G. A. Gutiérrez-Aceves, M. I. Ruiz-Flores. Fourth ventricle neurocysticercosis: Rigid endoscopic management. Description of direct transcerebellar approach. 26-Sep-2017;8:232. Available from: http://surgicalneurologyint.com/surgicalint-articles/fourth-ventricle-neurocysticercosis-rigid-endoscopic-management-description-of-direct-transcerebellar-approach/
Date of Submission
08-Jul-2017
Date of Acceptance
18-Jul-2017
Date of Web Publication
26-Sep-2017
Abstract
Background:Endoscopy has gained a crucial role in high specialty neurosurgery during the last decades. At present, there are well-defined flexible neuroendoscopic procedures to treat ventricular and subarachnoid space pathologies. Neurocysticercosis is recognized as a common cause of neurologic disease in developing countries and the United States. Surgical intervention, especially cerebrospinal fluid diversion, is the key for management of hydrocephalus. In 2002, a consensus suggested that ventricular forms should be treated with endoscopy as the first option.
Case Description:Here, we present the case of a 51-year-old right-handed male, from Estado de México. Two days before admission he experienced holocraneal headache 7/10 on the visual analogue scale which was intermittent, with no response to any medication, sudden worsening of pain to 10/10, nausea, and vomit. On physical examination, he presented with 14 points in the Glasgow coma scale (M6, O4, V4), pupils were 3 mm, there was adequate light-reflex response, and bilateral papilledema. The cranial nerves did not have other pathological responses, extremities had adequate strength of 5/5, and normal reflexes (++/++) were noted. Neuroimaging studies showed dilatation of the four ventricles as well as a cystic lesion in the fourth ventricle. Surgical position was Concorde, and the approach through a suboccipital burr hole was planned preoperatively with craneometric points. A rigid Karl Storz Hopkins II® endoscope was inserted directly through the cerebellum and the cystic lesion was extracted entirely.
Conclusion:This article presents a useful technique with low morbidity and mortality. Further investigation is needed, especially in our Mexico, where neuroendoscopical techniques are still in the development phase.
Keywords: 4th ventricle neurocysticercosis, neuroendoscopy, transcerebellar approach
BACKGROUND
Endoscopy has gained a crucial role in high specialty neurosurgery during the last decades. It started being used in neurosurgery 30 years ago and is the approach of choice for multiple pathologies such as spontaneous intracranial hemorrhage, hydrocephalus, pituitary adenoma, and intraventricular tumors.[
The fourth ventricle was originally studied by Galen[
The fourth ventricle exploration has been reported by Torres-Corzo et al. in tri or tetraventricular hydrocephalus;[
Neurocysticercosis is recognized as a common cause of neurologic disease in developing countries as well as the United States. The pathogenesis and clinical manifestations vary with the site of infestation and the accompanying host response. Ventricular neurocysticercosis often causes obstructive hydrocephalus. Surgical intervention, especially cerebrospinal fluid diversion, is the key to the management of hydrocephalus. Shunt failure may be less frequent when patients are treated with prednisone and/or antiparasitic drugs. Subarachonid cysticercosis is associated with arachnoiditis. Arachnoiditis may result in meningitis, vasculitis with stroke, or hydrocephalus. Patients should be treated with corticosteroids, antiparasitic drugs, and shunting if hydrocephalus is present.[
In 2002, a consensus suggested that ventricular forms should be treated with endoscopy as the first option.[
CASE DESCRIPTION
A 51-year-old right-handed male, from Estado de México, presented with deficient hygiene and dietary habits. He was hypertense since 5 months prior to presentation which was controlled with losartan (40 mg once daily). Two days before admission, he experienced holocraneal headache 7/10 in the visual analogue scale, intermittent, with no response to any medication, sudden worsening of pain to 10/10, nausea, and vomit. On physical examination, he presented with 14 points in the Glasgow coma scale (M6, O4, V4), pupils were 3 mm, adequate light-reflex response, and bilateral papilledema. The cranial nerves did not have other pathological responses, extremities had adequate strength 5/5, and normal reflexes (++/++) were noted. He presented with gait disturbance with lateralization to the right side [
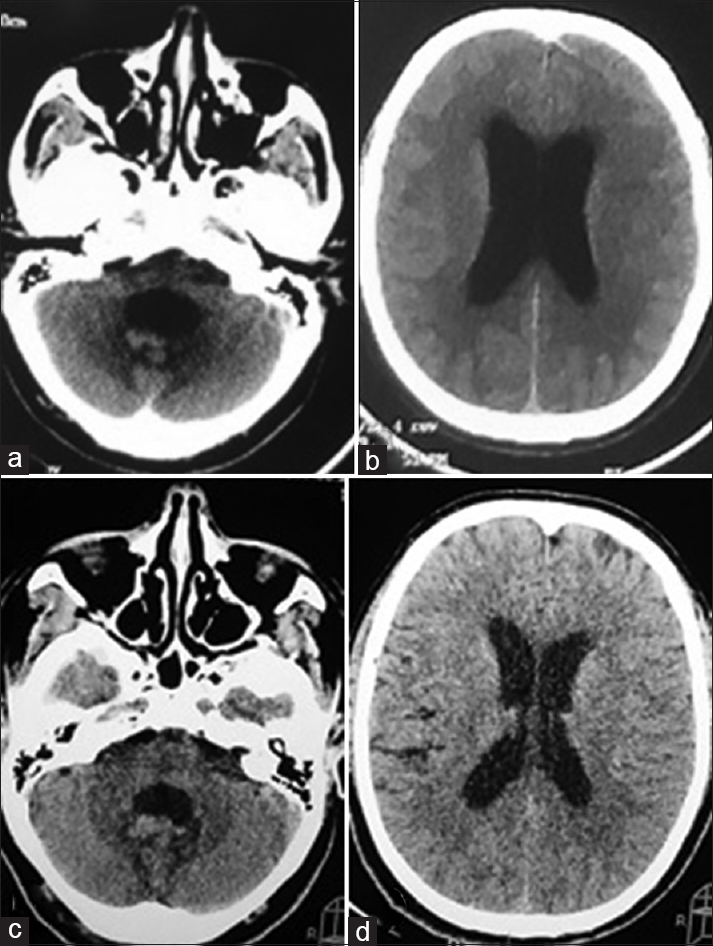
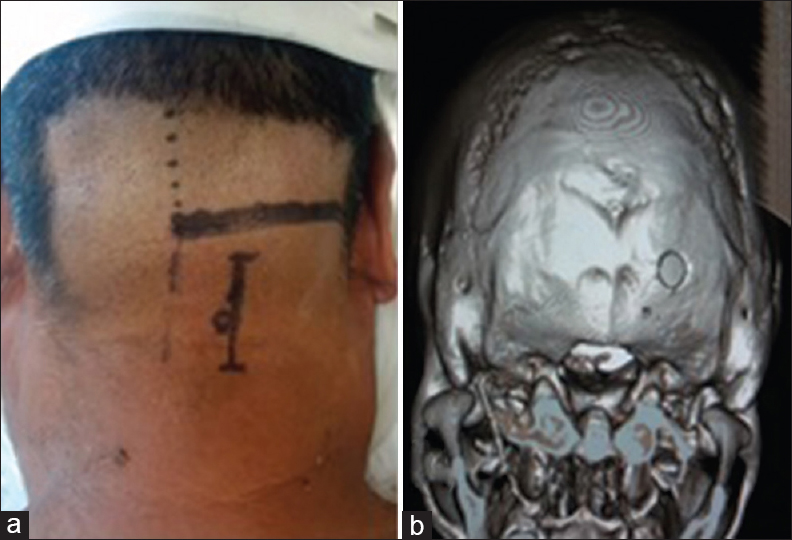
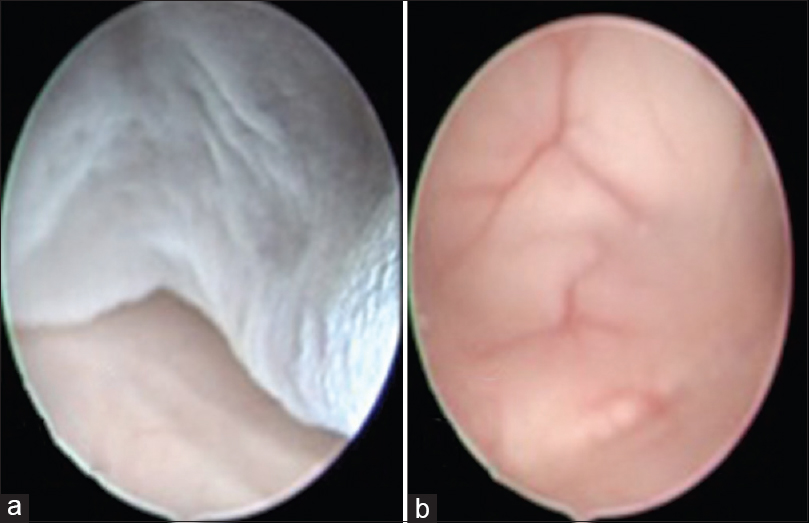
We describe our surgical decision and rationale for this management. The patient had classical clinical symptoms of intracranial hypertension such as headache, nausea and vomiting. The computed tomography (CT) scans showed tetraventricular hydrocephalus and important dilatation of the fourth ventricle, due to this finding and because of the high prevalence of neurocysticercosis in our country, we decided to perform a fourth ventricle exploration with the Hopkins II rigid endoscope (Karl Storz, Germany)®. In this case, we considered that the described approach for the exploration of the fourth ventricle through a prefrontal burr-hole with flexible endoscopy could be riskier than approaching just the fourth ventricle with one suboccipital burr hole because the third ventricle and cerebral aqueduct were not dilated enough to allow our endoscope to go through. The patient was placed in a Concorde position, with a soft head paddle, taking care of the pressure points to avoid any complication, and then adequate antisepsis of the region was performed with iodine solution. A single burr hole approach was made, which was planned 3 cm from the midline to the right side and 2 cm down from the inion. The burr hole was planned with craneometric points in the preoperative images, as shown, we did not use any image-guided system. The skin was approached in the standard manner until the suboccipital bone was reached. Then we performed the burr hole with a midas rex system and adequate hemostasis was made. The dura was opened in a cruciate form and then we performed a 1 cm cortisectomy with bipolar forceps. The rigid endoscope was inserted directly through the cerebellar cortical surface in the right hemisphere with a freehand approach. Just as soon as the endoscope passed through to the fourth ventricle, a cystic lesion was found, which was compatible with a neurocysti; as shown in the image it was not adherent to any of the fourth ventricle structures. We were able to remove the entire cystic lesion, and then we performed a fourth ventricle exploration, showing that the aqueduct and both Luschka foramina were permeable, as well as the obex. Surgical time was 40 minutes with no complications. The fourth ventricle ependymal showed no macroscopycal findings of ependymitis, and due to the surgical procedure the cerebrospinal fluid flow was restored. Postoperatively, the patient did well and was discharged home 48 hours later, with oral standard neurocysticercosis treatment with albendazole 15 mg/kg and corticosteroids [Figures
CONCLUSION
As described by Bergsneider et al.,[
In selected patients such as this one, that presents with a single neurocysti in the fourth ventricle and tetraventricular hydrocephalus, we consider that cerebrospinal fluid diversion with a shunt device has risks such as malfunction or infection, and also the CSF diversion would not remove the neurocysti that would keep the inflammatory response of the host going on, and this could lead to complications such as neurological deterioration and death.
In addition, medical treatment has shown partial results in the intraventricular forms of neurocysticercosis.[
Because there is no consensus regarding the management of the fourth ventricular cysticercosis, we consider that this paper shows a useful technique that can be introduced to the neuroendoscopical field to treat this pathology. Further investigation is needed, especially in Mexico where neuroendoscopical techniques are still in the developmental phase.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Baig MN, Chishty F, Immesoete P, Karas CS. The Eastern Heart and Galen's ventricle: A historical review of the purpose of the brain. Neurosurg Focus. 2007. 23: E3-
2. Bergsneider M. Endoscopic removal of cysticercal cysts within the fourth ventricle: Technical note. J Neurosurg. 1999. 91: 340-5
3. Blount JP, Campbell JA, Haines SJ. Complications in ventricular cerebrospinal fluid shunting. Neurosurg Clin N Am. 1993. 4: 633-
4. Carpio A, Santillán F, León P, Flores C, Hauser WA. Is the course of neurocysticercosis modified by treatment with antihelmintic agents?. Arch Intern Med. 1995. 155: 1982-8
5. García HH, Evans CA, Nash TE, Takayanagui OM, White AC, Botero D. Current consensus guidelines for treatment of neurocysticercosis. Clin Microbiol Rev. 2002. 15: 747-56
6. Husain M, Rastogi M, Jha DK, Husain N, Gupta RK. Endoscopic transaqueductal removal of fourth ventricular neurocysticercosis with an angiographic catheter. Neurosurgery. 2007. 60: 249-54
7. Matula C, Reinprecht A, Roessler K, Tschabitscher M, Koos WT. Endoscopic exploration of the IVth ventricle. Minim Invasive Neurosurg. 1996. 39: 86-92
8. Méndez PJA, Bargés CJ, Méndez RD. Neurocirugía endoscópica, la nueva era. Residente. 2009. 4:
9. Ranjan M, Konar SK, Somanna S, Bhagavatula ID, Ashwathnarayana CB. Endoscopic intervention for the fourth ventricular neurocysticercal cyst: What should be the optimum therapeutic approach?. Br J Neurosurg. 2014. 28: 626-30
10. Rodríguez-Della Vecchia R, Torres-Corzo J, Chalita Williams JC, Rangel-Castilla L, Ramos Zuniga R.editors. “Historia de la endoscopia”. Tractos Historicos de la Neurocirugia en Mexico. Guadalajara, Mexico: Ediciones de la Noche; 2012. p.
11. Torres-Corzo J, Rangel-Castilla L. Flexible Neuroendoscopy: Part II—Clinical and diagnostic indications. Contempor Neurosurg. 2013. 35: 1-5
12. Torres-Corzo J, Rangel-Castilla L. Flexible Neuroendoscopy: Part III-Basic endoscopic procedures and advantages of flexible neuroendoscopy. Contempor Neurosurg. 2013. 35: 1-6
13. Torres-Corzo J, Rangel-Castilla L. Flexible Neuroendoscopy: Part IV – Advanced endoscopic procedures and complications of flexible neuroendoscopy. Contempor Neurosurg. 2013. 35: 6-
14. Torres-Corzo J, Rangel Castilla L, Nakaji P.editorsNeuroendoscopic Surgery. Thieme; 2016. p.
15. Tubbs RS, Loukas M, Shoja MM, Shokouhi G, Oakes WJ. Francois Magendie and his contributions to the foundations of neuroscience and neurosurgery. J Neurosurg. 2008. 108: 1038-42
16. Tubbs RS, Vahedi P, Loukas M, Shoja MM, Cohen-Gadol AA. Hubert von Luschka: His life, discoveries, and contributions to our understanding of the nervous system. J Neurosurg. 2011. 114: 268-72
17. White AC. Neurocysticercosis: Updates on epidemiology, pathogenesis, diagnosis and management. Ann Rev Med. 2000. 51: 187-206


efren herrera
Posted August 21, 2020, 8:46 am
No mention of Scolex that are usually present at this place. An MRI is sugested for follow up.