

- Department of Histopathology, Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, India
- Department of Radiotherapy, Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, India
- Department of Neurosurgery, Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, India
Correspondence Address:
Bishan Dass Radotra
Department of Neurosurgery, Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, India
DOI:10.4103/sni.sni_284_17
Copyright: © 2018 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Debajyoti Chatterjee, Bishan Dass Radotra, Narendra Kumar, Rakesh Kumar Vasishta, Sunil Kumar Gupta. IDH1, ATRX, and BRAFV600E mutation in astrocytic tumors and their significance in patient outcome in north Indian population. 14-Feb-2018;9:29
How to cite this URL: Debajyoti Chatterjee, Bishan Dass Radotra, Narendra Kumar, Rakesh Kumar Vasishta, Sunil Kumar Gupta. IDH1, ATRX, and BRAFV600E mutation in astrocytic tumors and their significance in patient outcome in north Indian population. 14-Feb-2018;9:29. Available from: http://surgicalneurologyint.com/surgicalint-articles/idh1-atrx-and-brafv600e-mutation-in-astrocytic-tumors-and-their-significance-in-patient-outcome-in-north-indian-population/
Date of Submission
02-Aug-2017
Date of Acceptance
14-Nov-2017
Date of Web Publication
14-Feb-2018
Abstract
Background:According to the current World Health Organization (WHO) classification of central nervous system (CNS) tumors (2016), histological diagnosis of gliomas should be supplemented by molecular information. This study was carried out to determine the frequency of isocitrate dehydrogenase 1 (IDH1), ATRX, and BRAF V600E mutations in different grade astrocytomas and their prognostic value.
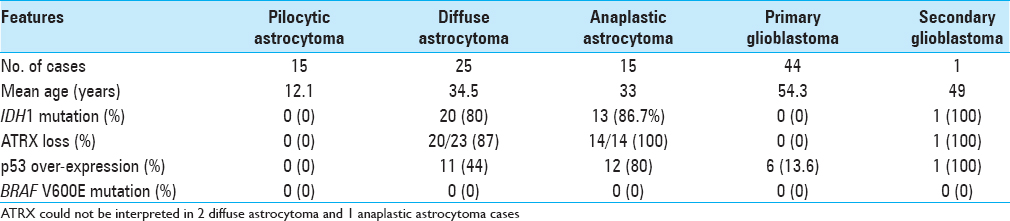
Methods:Eighty cases of astrocytoma (15 pilocytic astrocytoma, 25 diffuse astrocytoma, 15 anaplastic astrocytoma, and 25 glioblastoma) with follow-up information were analyzed using immunohistochemistry for IDH1 mutant protein, ATRX, p53, and BRAF. Sanger sequencing was carried out for IDH1 exon 4 and BRAF exon 15.
Results:All pilocytic astrocytoma and primary glioblastoma cases were negative for IDH1 mutation. IDH1 mutation was detected in 80% (20/25) DA and 87% (13/15) AA cases. IDH1 R132H was the commonest IDH1 mutation (94.1%) and immunohistochemistry showed 100% sensitivity and specificity to detect this mutation. Loss of nuclear ATRX expression was found in 87% (20/23) and 100% (14/14) DA and AA cases, respectively. IDH1 mutant DA patients had longer overall survival than IDH1 wild cases, although this difference was not significant (79.5 months vs. 42.5 months, P value 0.417). BRAF V600E mutation was not detected in any astrocytic tumor.
Conclusions:IDH1 and ATRX mutations are very common in diffuse astrocytoma and anaplastic astrocytoma, while they are rare in pilocytic astrocytoma and glioblastoma. Immunohistochemistry for IDH1 and ATRX can successfully characterize the diffuse gliomas into molecularly defined groups in majority of the cases. BRAF V600E mutation is rare in astrocytic tumors in Indian population.
Keywords: Astrocytoma, ATRX, BRAF, glioblastoma, isocitrate dehydrogenase
INTRODUCTION
Gliomas are the commonest brain tumors, both in adults as well as in children. According to the World Health Organization (WHO) classification of central nervous system (CNS) tumors 2007, gliomas were divided into astrocytomas, oligodendrogliomas, and mixed oligoastrocytomas.[
The most important and well described molecular alteration in the pathogenesis of grade glioma is isocitrate dehydrogenase (IDH) mutation. It is now believed that IDH mutation is responsible for initiation of glioma genesis. IDH1 or IDH2 mutation is seen in >90% of astrocytomas and oligodendrogliomas.[
These molecular markers not only help to classify the glial tumors into different molecular subgroups, but also provide prognostic information. It has been observed that IDH mutant gliomas carry better prognosis than IDH wild-type tumors. Gliomas with 1p/19q co-deletion behave better than cases that do not show this deletion. Glioblastomas with IDH mutation also show longer survival than IDH wild type GBs. According to the recommendation of ISN-Haarlem 2014 consensus, only histological diagnosis with a WHO grade is no longer sufficient.[
Most of the information regarding molecular alterations in gliomas is available from the western literature. There is limited data involving these molecules in glial tumors in the Indian population.[
MATERIALS AND METHODS
A retrospective study was performed. Patients of different grades of astrocytoma (grade I to IV) diagnosed in the year 2011 were evaluated for the molecular alterations. The clinical detail of the patients was obtained from the database of Department of Radiotherapy. Those patients who underwent near total or gross total excision with available follow-up information were included in this study. Cases diagnosed on stereotactic biopsy, cases for which the blocks were not available or patients who were lost to follow up were excluded. Other astrocytic tumors like pleomorphic xanthoastrocytoma (PXA) and other glioneuronal tumors were excluded from the study. Archival material from the Department of Histopathology was used for histopathological, immunohistochemical, and molecular analyses.
The follow-up information for patients with grade II–IV tumor was obtained from the department of Radiotherapy. For the patients with grade I tumor, follow up information was obtained by personal communication.
Slides of all these cases were reviewed. All the cases were classified and graded according to the existing 2016 WHO criteria.[
Immunohistochemistry
IHC was carried out at least on one representative block in all the cases. IHC was performed using primary antibody against the following antigens- IDH1 R132H (Dianova, dilution 1:40), ATRX (Sigma, dilution 1:300), p53 (Dako, dilution 1:50), Ki-67 (OSB, dilution 1:300), and BRAF (VE1 clone, Ventana).
Cases showing cytoplasmic positivity for IDH1 in >10% tumor cells were considered positive.[
Molecular analysis
DNA was extracted from the formalin-fixed, paraffin-embedded (FFPE) tissue by commercially available (Qiagen) kit as per manufacturer's instruction.
For IDH1 mutation analysis, exon 4 of the IDH1 gene was amplified using following sets of primers -
Forward primer: 5′-TCACCAAATGGCACCATACGA-3′
Reverse primer: 5′-TCATACCTTGCTTAATGGGTGT-3′
Using this pair of primers, a product of 255bp was amplified. In brief, the initial reaction was at 95°C, followed by denaturation at 95°C, annealing at 54°C, and amplification at 72°C. This cycle was repeated for 36 times.
For BRAF V600E mutation, exon 15 of the BRAF gene was amplified using following set of primers -
Forward primer: 5′-TCTTCATAATGCTTGCTCTGATA GG-3′
Reverse primer: 5′-CTAGTAACTCAGCAGCATCTCAGG-3′.
Using this set of primers, a product of 250 bp was amplified. In brief, the initial reaction was at 95°C, followed by denaturation at 95°C, annealing at 58°C, and amplification at 72°C. This cycle was repeated for 38 times.
The amplification products were purified using commercially available DNA purification kit (Quigen) and subjected to Sanger sequencing.
Fluorescent in-situ hybridization
FISH for 1p/19q was carried out in 10 selective astrocytoma cases (as discussed subsequently). It was carried out on formalin-fixed, paraffin-embedded tissue using commercially available probes (Vysis 1p36/LSI 1q 25 and LSI 19q13/19p 13 dual color probe). For analysis, 200 nonoverlapping interphase nuclei were counted. Ratio of red to green signal was calculated and ratio <0.8 was taken as deleted.
Control
Twenty cases of oligodendroglioma (ODG), 10 each for WHO grade II and grade III were included for comparison of the molecular findings. We performed immunohistochemistry for IDH1, ATRX, p53, Ki-67 and BRAF as well as sequencing for IDH1 exon 4 and BRAF exon 15 in all these cases. FISH for 1p/19q was also performed in 8 selective cases (as described subsequently). DNA extracted from peripheral blood of a normal donor was subjected to sequencing to obtain the normal sequence (IDH1 exon 4 and BRAF exon 15) for purpose of comparison. DNA of one case of hairy cell leukemia was used as a positive control for BRAF V600E mutation.
Follow-up of patients
Clinical details including treatment history were noted from the patient's file. The patients were followed up till December, 2015. Outcome in terms of death, recurrence or disease-free survival wwas recorded.
Statistical analysis
All statistical analyses were carried out using SPSS software, version 21 (SPSS Inc; Chicago, IL, USA). For normally distributed parametric data, student's t test and analysis of variant (ANOVA) were used. For non-parametric data, Kruskal Wallis test followed by Mann–Whitney tests were applied. Statistical significance was considered if P value is <0.05. Kaplan–Meier estimator and Cox proportional hazards regression were performed to assess survival data.
This study was approved by the institute ethics committee.
RESULTS
Within this study period, a total of 28 pilocytic astrocytoma, grade I (PA), 35 diffuse astrocytoma, grade II (DA), 18 anaplastic astrocytoma, grade III (AA), and 87 glioblastoma, grade IV (GB) cases were diagnosed on histopathology examination [
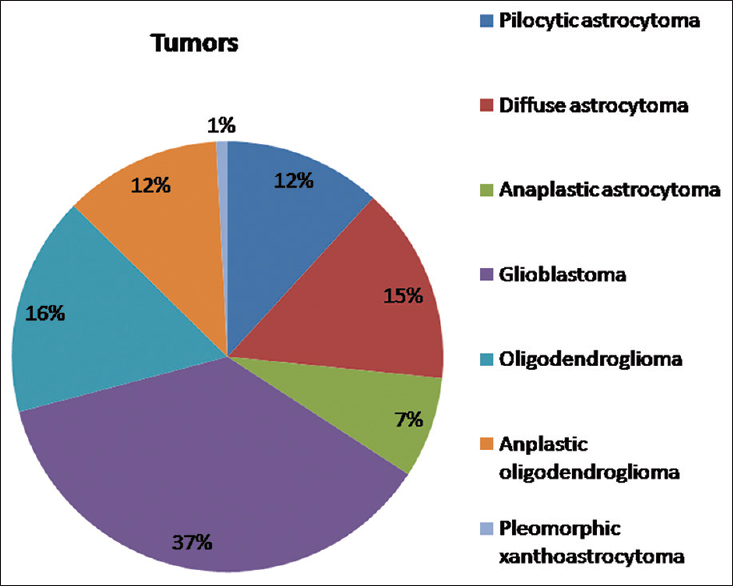
We finally included 15 PA, 25 DA, 15 AA, and 45 cases of GB in this study. There were 44 primary GB cases and one secondary GB case, which developed in the background of AA diagnosed 22 months earlier. The age of the patients ranged from 11–68 years (mean 46.4 years), and there was male predominance (65% males). All cases of DA, AA, and GB were located supratentorially with frontal lobe being the commonest site (67.7%), while 60% of the PA (n = 9) were infratentorial in location. All cases underwent near total or gross total excision. Twenty cases of ODG (10 grade II and 10 grade III) were randomly selected for molecular analysis (as control group).
Post-operative therapy
None of the PA cases received any post operative therapy. All DA cases received 54Gy radiotherapy (RT) and none received chemotherapy (CT). All AA patients received 60 Gy, while one patient was given 54Gy radiation. One case of AA received six cycles of temozolomide chemotherapy. All cases of GB received RT. Majority (43 cases) received 60Gy radiation. One young boy of 16 years and one 62-year-old male with poor general health received lower dose (40Gy and 54Gy, respectively). Thirteen cases received temozolomide chemotherapy ranging from 2 to 23 cycles.
Molecular analysis [ Table 1 ]
A. Pilocytic astrocytoma [Figure
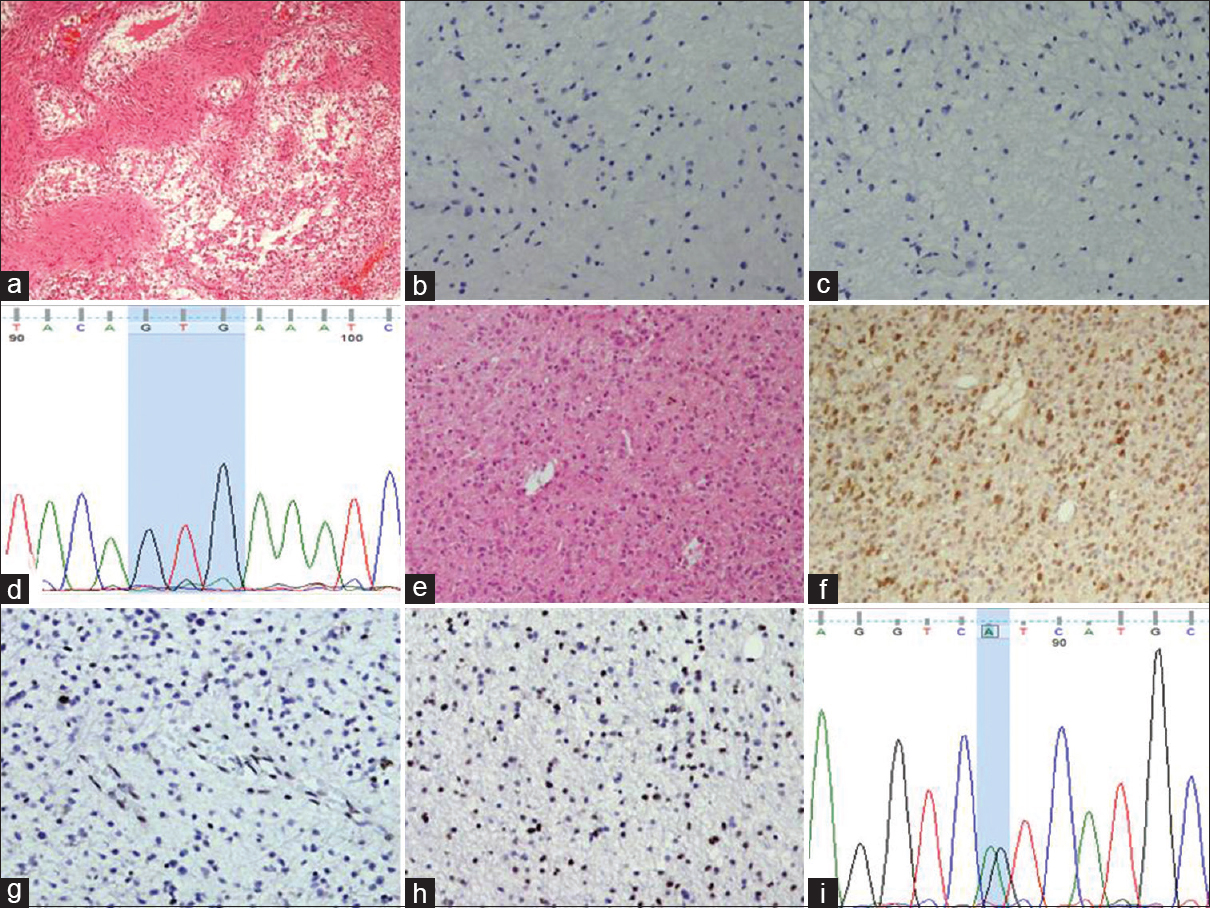
Figure 2
(a) Photomicrograph showing pilocytic astrocytoma (HE, ×100). This case is negative for IDH1 (b, immunohistochemistry, ×200) and BRAF (c, immunohistochemistry, ×200). (d) Chromatogram featuring BRAF exon 15 sequencing from pilocytic astrocytoma showing normal sequence. (e) Photomicrograph showing diffuse astrocytoma with infiltrative pattern of growth (HE, ×100). The tumor cells of the same case show IDH1 positivity (f, immunohistochemistry, ×100), loss of nuclear ARTX expression (g, immunohistochemistry, ×100) and p53 expression (h, immunohistochemistry, ×100). (i) Chromatogram of IDH1 exon 4 from the same tumor shows heterozygous mutation at nucleotide position 395 (G to A) producing IDH1 R132H mutation
B. Diffuse astrocytoma: Out of 25 cases of DA, 18 showed positivity for IDH1 IHC [Figure
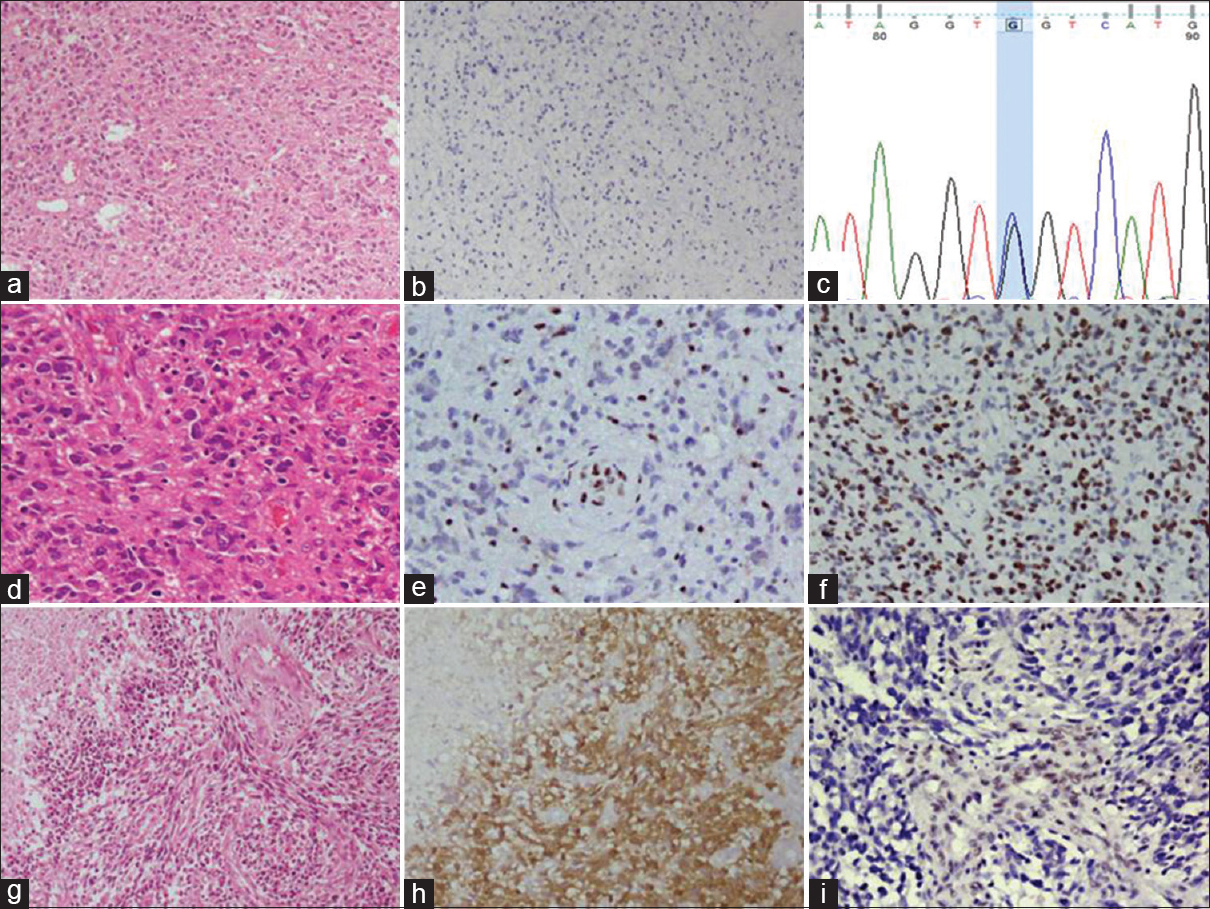
Figure 3
(a) Photomicrograph of a diffuse astrocytoma (HE, ×100) which is negative for IDH1 immunohistochemistry (b, ×100). (c) Chromatogram of IDH1 exon 4 from the same tumor shows heterozygous mutation at nucleotide position 394 (c-g) producing IDH1 R132G mutation. (d) Photomicrograph of anaplastic astrocytoma (HE, ×200). The tumor cells show loss of nuclear ATRX expression, whereas the endothelial cells are positive (e, immunohistochemistry, ×200) and they show strong p53 expression (f, immunohistochemistry, ×200). (g) Photomicrograph showing secondary glioblastoma with area of necrosis (HE, ×100). The same case showing diffuse IDH1 positivity (h, immunohistochemistry, ×100) and loss of ATRX expression (i, immunohistochemistry, ×200)
Fluorescent in-situ hybridization (FISH): five DA cases (IDH1-mutant and ATRX lost), three IDH1-mutant DA cases with retained nuclear ATRX expression, and two IDH1-mutant DA cases where ATRX staining could not be interpreted were subjected to fluorescent in-situ hybridization (FISH) analysis for 1p/19q co-deletion. All ten cases were 1p/19q non-deleted, thus confirming astrocytic nature of these tumors.
C. Anaplastic astrocytoma [Figure
D. Primary glioblastoma: All cases of primary GB were negative for IDH1 mutation by both IHC and sequencing. All primary GB cases showed retained nuclear ATRX expression. p53 over-expression was found in 13.6% (6/44) primary GBs. BRAF V600E mutation was consistently negative in GB cases, both by IHC and sequencing.
E. Secondary glioblastoma [Figure
Correlation of IHC and sequencing
There were total 34 IDH1-mutant cases in this series, out of which 32 (94.1%) showed IDH1 immunopositivity (18 DA, 13 AA and 1 secondary GB). All these immunopositive cases showed heterozygous IDH1 R132H mutation by sequencing. None of the IDH immunonegative cases showed this mutation by sequencing. Thus, IHC showed 100% sensitivity and specificity for detecting IDH1 R132H mutation. However, two DA cases showed different IDH1 exon 4 mutations, which were not detected by this mutation specific antibody.
Molecular analysis in the control group
IDH1 immunopositivity was observed in 90% (9/10) grade II and 80% (8/10) grade III ODG. Sequencing confirmed heterozygous IDH1 R132H mutation in these cases. No additional IDH1 mutation was detected on sequencing. Nuclear ATRX staining was retained in 90% (9/10) grade II and 100% (10/10) grade III ODGs. All cases were negative for p53, except one grade II ODG, which had shown loss of ATRX nuclear staining. All cases were negative for BRAF V600E mutation. FISH for 1p/19q was performed on 4 grade II and 4 grade III ODGs. Three grade II and all 4 grade III ODG showed 1p/19q co-deletion, thus confirming their oligodendroglial nature. However, one IDH1 immunopositive grade II ODG, which revealed over-expression of p53 and loss of nuclear ATRX staining, was 1p/19q non co-deleted. Thus, based on molecular findings, this case was re-categorized as diffuse astrocytoma, IDH1-mutant.
Survival analysis [ Table 2 ]

All cases of PA were alive and there was no recurrence expect in one case, which recurred 23 months after the surgery. Among the DA patients, 6 passed away (24%). The median survival period was 70.27 months. In the AA group, 7 patients expired (46.7%). Among the living patients, 2 experienced recurrence. The mean survival time was 46.17 months. For the primary GB patients, 39 (88.6%) expired with median survival 19.7 months. One case of secondary GBM was alive at 44 months follow up. The difference of mean survival among different grades was statistically significant (P value 0.003) [
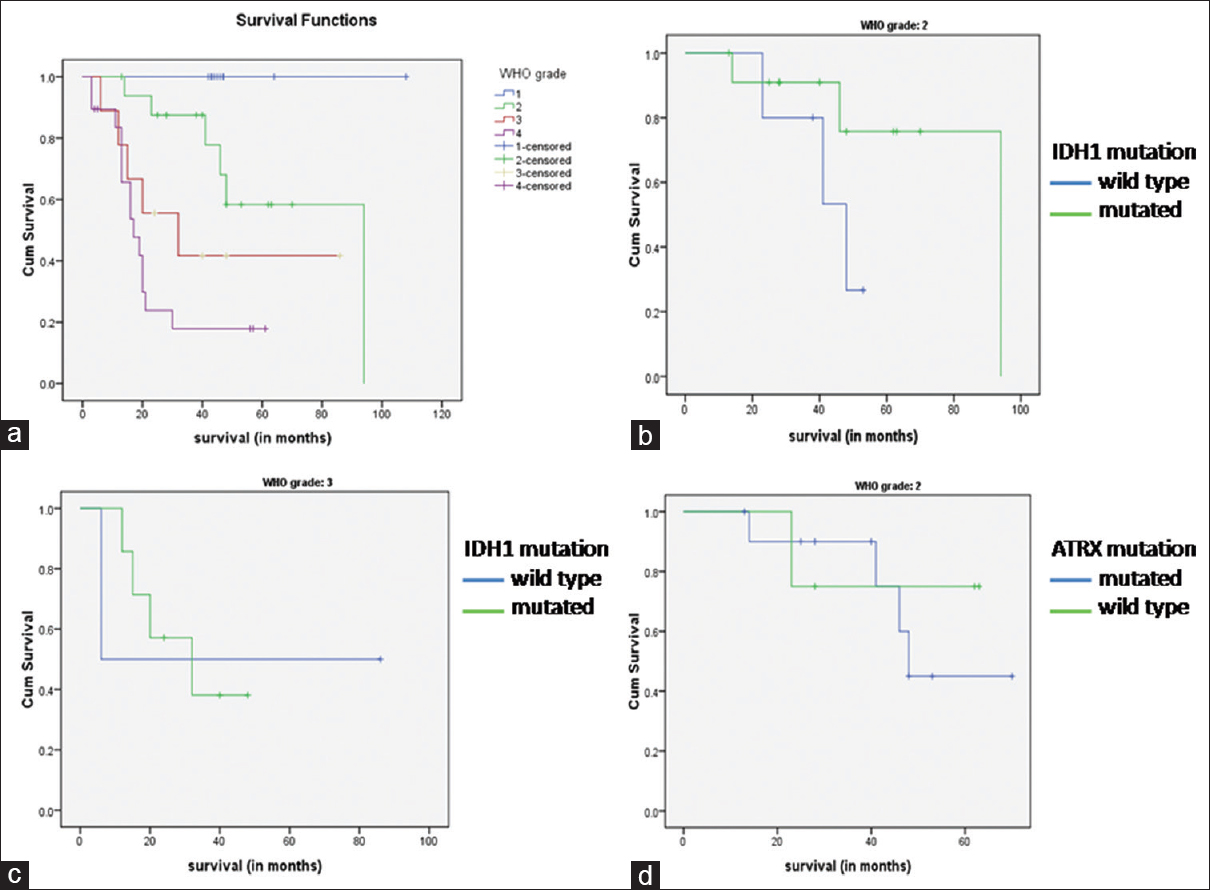
Figure 4
(a) Kaplan–Meier curves showing overall survival in different grades of astrocytoma. (b) Kaplan–Meier curves showing overall survival in diffuse astrocytoma with and without IDH1 mutation. (c) Kaplan–Meier curves showing overall survival in IDH1 mutant and IDH1 wild type anaplastic astrocytoma. (d) Kaplan–Meier curves showing overall survival in diffuse astrocytoma with and without ATRX mutation
The mean survival time of IDH1-mutant and IDH1-wild DA were 79.5 and 42.5 months respectively [
DISCUSSION
The understanding about the pathogenesis and biology of gliomas has undergone revolutionary changes in the recent years. The incorporation of molecular information has helped categorization of glial tumors into different prognostic groups, which assists the individualization and optimization of the treatment. It is now considered that diffuse astrocytoma and anaplastic astrocytoma share similar genetic profile and they are characterized by IDH and ATRX mutation. Isocitrate dehydrogenase (IDH) is one of the most well recognized and widely described molecular markers in glial tumors, both with astrocytic and oligodendroglial differentiation. The frequency of IDH mutation in diffuse glioma is variable, ranging from 54% to 90%.[
IDH1 mutation is also associated with favorable outcome in high grade gliomas.[
ATRX mutation is a feature of astrocytic differentiation, which can be determined by loss of nuclear ATRX expression on immunohistochemistry. It occurs more frequently in DA (60–70%) and AA (70–80%) and is very rare in primary GB (4–6%).[
CONCLUSION
Diffuse astrocytoma and anaplastic astrocytoma are characterized by frequent IDH1 mutation, which can be efficiently detected by IDH1 immunohistochemistry. Combined IDH1 and ATRX IHC can accurately confirm the molecular nature of most of the DA and AA cases, thus avoiding the need of expensive investigations like FISH. p53 can act as a surrogate marker for astrocytic differentiation. IDH1 mutation was not found in any pilocytic astrocytoma and primary glioblastoma cases. Although IDH1 mutant and p53 negative DA cases had a longer survival than IDH1 wild and p53 positive DA cases, respectively, these differences were not statistically significant. BRAF V600E mutation is extremely rare in astrocytic tumors in our population.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Abudumijiti A, Chan AK, Shi Z, Li Y, Zhang R, Yang R. Adult IDH Wild-type Lower-grade Gliomas Should Be Further Stratified. Neuro Oncol. 2017. 19: 1327-37
2. Ahmadi R, Stockhammer F, Becker N, Hohlen K, Misch M, Christians A. No prognostic value of IDH1 mutations in a series of 100 WHO grade II astrocytomas. J Neurooncol. 2012. 109: 15-22
3. Aldape K, Burger PC, Perry A. Clinicopathologic aspects of 1p/19q loss and the diagnosis of oligodendroglioma. Arch Pathol Lab Med. 2007. 131: 242-51
4. Cahill DP, Sloan AE, Nahed BV, Aldape KD, Louis DN, Ryken TC. The role of neuropathology in the management of patients with diffuse low grade glioma: A systematic review and evidence-based clinical practice guideline. J Neurooncol. 2015. 125: 531-49
5. Capper D, Sahm F, Hartmann C, Meyermann R, von Deimling A, Schittenhelm J. Application of mutant IDH1 antibody to differentiate diffuse glioma from nonneoplastic central nervous system lesions and therapy-induced changes. Am J Surg Pathol. 2010. 34: 1199-204
6. Capper D, Weissert S, Balss J, Habel A, Meyer J, Jäger D. Characterization of R132H mutation-specific IDH1 antibody binding in brain tumors. Brain Pathol. 2010. 20: 245-54
7. Capper D, Zentgraf H, Balss J, Hartmann C, von Deimling A. Monoclonal antibody specific for IDH1 R132H mutation. Acta Neuropathol. 2009. 118: 599-601
8. Cohen AL, Holmen SL, Colman H. IDH1 and IDH2 mutations in gliomas. Curr Neurol Neurosci Rep. 2013. 13: 345-
9. Haberler C, Wohrer A. Clinical Neuropathology practice news 2-2014: ATRX, a new candidate biomarker in gliomas. Clin Neuropathol. 2014. 33: 108-11
10. Hartmann C, Meyer J, Balss J, Capper D, Mueller W, Christians A. Type and frequency of IDH1 and IDH2 mutations are related to astrocytic and oligodendroglial differentiation and age: A study of 1,010 diffuse gliomas. Acta Neuropathol. 2009. 118: 469-74
11. Houillier C, Wang X, Kaloshi G, Mokhtari K, Guillevin R, Laffaire J. IDH1 or IDH2 mutations predict longer survival and response to temozolomide in low-grade gliomas. Neurology. 2010. 75: 1560-6
12. Ichimura K, Pearson DM, Kocialkowski S, Bäcklund LM, Chan R, Jones DT. IDH1 mutations are present in the majority of common adult gliomas but rare in primary glioblastomas. Neuro Oncol. 2009. 11: 341-7
13. Ikemura M, Shibahara J, Mukasa A, Takayanagi S, Aihara K, Saito N. Utility of ATRX immunohistochemistry in diagnosis of adult diffuse gliomas. Histopathology. 2016. 69: 260-7
14. Jha P, Suri V, Sharma V, Singh G, Sharma MC, Pathak P. IDH1 mutations in gliomas: First series from a tertiary care centre in India with comprehensive review of literature. Exp Mol Pathol. 2011. 91: 385-93
15. Jiao Y, Killela PJ, Reitman ZJ, Rasheed AB, Heaphy CM, de Wilde RF. Frequent ATRX, CIC, FUBP1 and IDH1 mutations refine the classification of malignant gliomas. Oncotarget. 2012. 3: 709-22
16. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK.editorsWHO Classification of Tumours of the Central Nervous System. Lyon: International Agency for Research on Cancer (IARC); 2007. p.
17. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK.editorsWHO Classification of Tumours of the Central Nervous System. Lyon: International Agency for Research on Cancer (IARC); 2016. p.
18. Louis DN, Perry A, Burger P, Ellison DW, Reifenberger G, von Deimling A. International Society Of Neuropathology--Haarlem consensus guidelines for nervous system tumor classification and grading. Brain Pathol. 2014. 24: 429-35
19. Myung JK, Cho H, Park CK, Kim SK, Lee SH, Park SH. Analysis of the BRAF (V600E) Mutation in Central Nervous System Tumors. Transl Oncol. 2012. 5: 430-6
20. Rajeswarie RT, Rao S, Nandeesh BN, Yasha TC, Santosh V. A simple algorithmic approach using histology and immunohistochemistry for the current classification of adult diffuse glioma in a resource-limited set-up. J Clin Pathol. 2017. p.
21. Reuss DE, Kratz A, Sahm F, Capper D, Schrimpf D, Koelsche C. Adult IDH wild type astrocytomas biologically and clinically resolve into other tumor entities. Acta Neuropathol. 2015. 130: 407-17
22. Reuss DE, Mamatjan Y, Schrimpf D, Capper D, Hovestadt V, Kratz A. IDH mutant diffuse and anaplastic astrocytomas have similar age at presentation and little difference in survival: A grading problem for WHO. Acta Neuropathol. 2015. 129: 867-73
23. Reuss DE, Sahm F, Schrimpf D, Wiestler B, Capper D, Koelsche C. ATRX and IDH1-R132H immunohistochemistry with subsequent copy number analysis and IDH sequencing as a basis for an “integrated” diagnostic approach for adult astrocytoma, oligodendroglioma and glioblastoma. Acta Neuropathol. 2015. 129: 133-46
24. Sanson M, Marie Y, Paris S, Idbaih A, Laffaire J, Ducray F. Isocitrate dehydrogenase 1 codon 132 mutation is an important prognostic biomarker in gliomas. J Clin Oncol. 2009. 27: 4150-4
25. Takano S, Ishikawa E, Sakamoto N, Matsuda M, Akutsu H, Noguchi M. Immunohistochemistry on IDH1/2, ATRX, p53 and Ki-67 substitute molecular genetic testing and predict patient prognosis in grade III adult diffuse gliomas. Brain Tumor Pathol. 2016. 33: 107-16
26. Takano S, Tian W, Matsuda M, Yamamoto T, Ishikawa E, Kaneko MK. Detection of IDH1 mutation in human gliomas: Comparison of immunohistochemistry and sequencing. Brain Tumor Pathol. 2011. 28: 115-23
27. Thon N, Eigenbrod S, Kreth S, Lutz J, Tonn JC, Kretzschmar H. IDH1 mutations in grade II astrocytomas are associated with unfavorable progression-free survival and prolonged postrecurrence survival. Cancer. 2012. 118: 452-60
28. Thota B, Shukla SK, Srividya MR, Shwetha SD, Arivazhagan A, Thennarasu K. IDH1 mutations in diffusely infiltrating astrocytomas: Grade specificity, association with protein expression, and clinical relevance. Am J Clin Pathol. 2012. 138: 177-84
29. Watanabe T, Nobusawa S, Kleihues P, Ohgaki H. IDH1 mutations are early events in the development of astrocytomas and oligodendrogliomas. Am J Pathol. 2009. 174: 1149-53
30. Weller M, Felsberg J, Hartmann C, Berger H, Steinbach JP, Schramm J. Molecular predictors of progression-free and overall survival in patients with newly diagnosed glioblastoma: A prospective translational study of the German Glioma Network. J Clin Oncol. 2009. 27: 5743-50
31. Wiestler B, Capper D, Holland-Letz T, Korshunov A, von Deimling A, Pfister SM. ATRX loss refines the classification of anaplastic gliomas and identifies a subgroup of IDH mutant astrocytic tumors with better prognosis. Acta Neuropathol. 2013. 126: 443-51
32. Yan H, Parsons DW, Jin G, McLendon R, Rasheed BA, Yuan W. IDH1 and IDH2 mutations in gliomas. N Engl J Med. 2009. 360: 765-73
33. Zhang CB, Bao ZS, Wang HJ, Yan W, Liu YW, Li MY. Correlation of IDH1/2 mutation with clinicopathologic factors and prognosis in anaplastic gliomas: A report of 203 patients from China. J Cancer Res Clin Oncol. 2014. 140: 45-51
34. Zou P, Xu H, Chen P, Yan Q, Zhao L, Zhao P. IDH1/IDH2 mutations define the prognosis and molecular profiles of patients with gliomas: A meta-analysis. PLoS One. 2013. 8: e68782-

