

- Department of Neurosurgery, University of Foggia, Foggia, Italy,
- Department of Neurosurgery, University of Bari, Bari, Italy.
Correspondence Address:
Francesco Carbone, Department of Neurosurgery, University of Foggia, Foggia, Italy.
DOI:10.25259/SNI_344_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Antonio Colamaria1, Maria Blagia2, Matteo Sacco1, Savino Iodice1, Francesco Carbone1. Infratentorial abscess secondary to dermal sinus associated with dermoid cyst in children: Review of the literature and report of a rare case. 14-Jun-2021;12:282
How to cite this URL: Antonio Colamaria1, Maria Blagia2, Matteo Sacco1, Savino Iodice1, Francesco Carbone1. Infratentorial abscess secondary to dermal sinus associated with dermoid cyst in children: Review of the literature and report of a rare case. 14-Jun-2021;12:282. Available from: https://surgicalneurologyint.com/surgicalint-articles/10885/
Date of Submission
08-Apr-2021
Date of Acceptance
23-May-2021
Date of Web Publication
14-Jun-2021
Abstract
Background: Dermal sinus is usually located at either end of neural tube but most commonly lumbosacral. When occipital, it extends caudally and is mostly localized in the midline position or in the cavity of the fourth ventricle. It could communicate with the skin through a fistula with potential risk of deeper abscesses. Posterior fossa abscess secondary to dermal sinus associated with intracranial dermal cyst is an uncommon pathology.
Case Description: A 24-month-old girl was admitted to our institution with a cutaneous fistula in the midline of the occipital region. Brain imaging showed an infratentorial intradiploic cyst with peripheral enhancement to contrast medium. The mass showed hyperintensity on T1-weighted sequences, with the lower signal on T2-weighted images. A suboccipital craniotomy was performed with evacuation of the abscess and excision of the capsule. Contextually a 3 cm whitish and encapsulated cystic mass with hair component was extracted. Histology confirmed the diagnosis of abscess associated with dermal cyst and dermal sinus. The patient condition improved and 15 days after excision, was discharged. The postoperative MRI showed total removal of the lesion. A 36-month follow-up highlighted no evidence of recurrence.
Conclusion: Posterior fossa dermoid cyst should be considered in all children with a cutaneous fistula. Early neurosurgical treatment of these benign tumors should be performed to prevent the development of severe intracranial infection. Best results are associated with early diagnosis and complete removal of the abscess. The present work further reviews the few similar cases that have been reported in the literature confirming the need for future research.
Keywords: Dermoid cyst, Infratentorial abscess, Pediatric cerebellar abscess, Posterior fossa dermoid tumor
INTRODUCTION
We report an unusual case of posterior fossa abscess secondary to a dermal sinus associated with intracranial dermal cyst. Intracranial dermoid tumors are usually developmental, rare, and benign, with a linear growth rate. They represent between 0.1% and 0.7% of all intracranial tumors.[
CASE REPORT
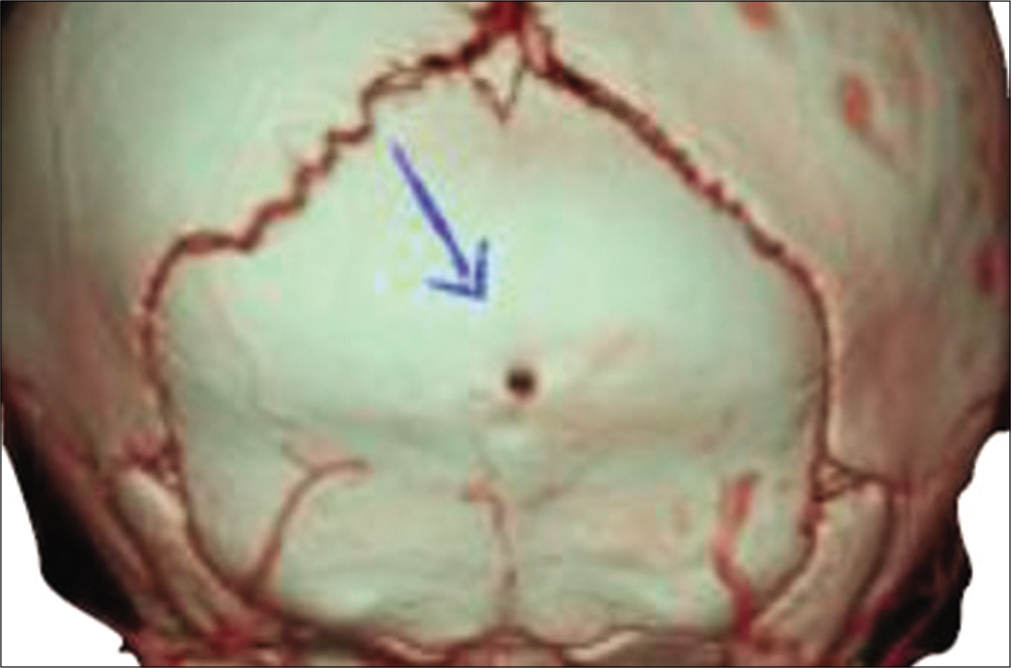
A 24-month-old female with a 2-month history of psychomotor retardation, weight loss, and unremarkable medical history was admitted to our institution. She presented horizontal nystagmus without sensory nor motor deficits. Physical examination revealed mild confusion and a cutaneous fistula in the mid-occipital region. The fistula appeared to communicate with intracranial space. Emergency CT scan [

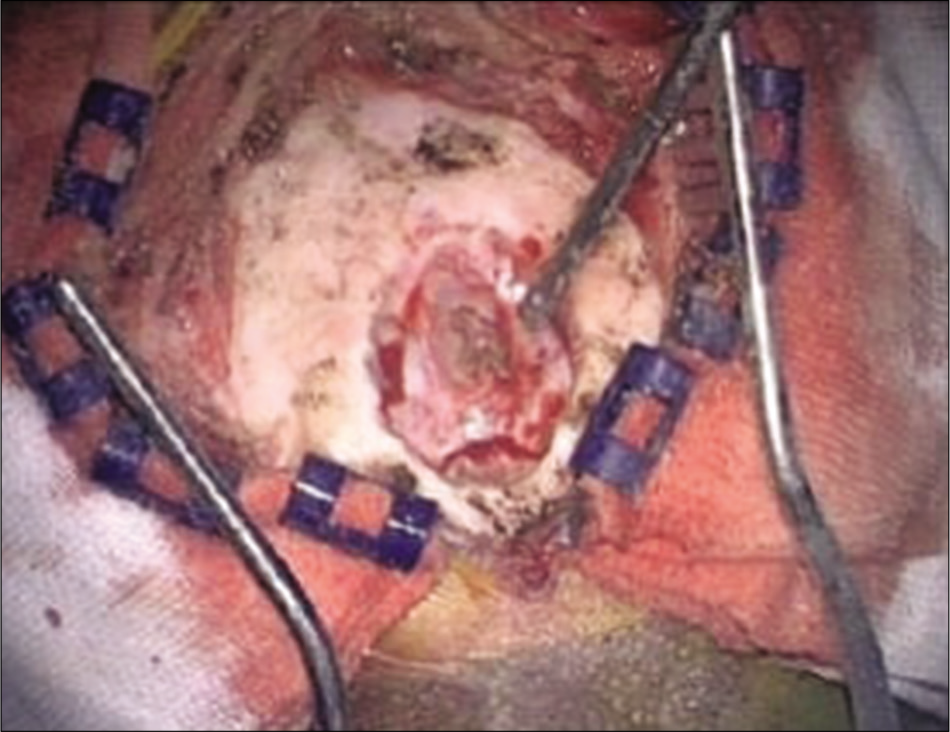
During preparation for surgery, a 5 mm non-purulent subcutaneous nodule with skin fistula was seen [


Bacterial investigation revealed methicillin-sensitive Staphylococcus aureus. Histological examination confirmed the diagnosis of dermoid tumor [

The patient’s physical condition and neurological symptoms improved rapidly. After 15 days, she was discharged without any deficit. At a 36-month follow-up, there was no evidence of recurrence [

DISCUSSION
Classification
Intracranial dermoid cyst represent a rare condition mostly recognized in the pediatric population with few cases described in the literature.[
Instrumental diagnosis
Dermoid cysts usually present as an oval or round defect on plain skull X-ray films. While they could be both small or moderate in diameter, rarely exceed 20 mm. Commonly reported are the sclerotic margins and the preferred midline location.[
Smith et al.[
Surgical treatment
Treatment of dermoid cysts consists in microsurgical excision and antibiotic therapy.[
CONCLUSION
Posterior fossa dermoid cyst should be suspected in children with an occipital skin lesion with concomitant dermal sinus. Neuroradiological investigation is necessary to define dermoid cyst site and any associated disorders. An early neurosurgical treatment should be performed to prevent the development of severe infections, such as bacterial meningitis and cerebellar abscess.[
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Akhaddar A, Boukhrissi N, Chakir N, El Hassani R, Hommadi A, Jiddane M. Dermoid cyst of the conus medullaris revealed by chronic urinary retention. Contribution of imaging. J Neuroradiol. 1999. 26: 132-6
2. Altman RS. Dermoid tumor of the posterior fossa associated with congenital dermal sinus: Report of a case and revies of the literature. J Pediatr. 1963. 62: 565-70
3. Davidson HD, Ouchi T, Steiner RE. NMR imaging of congenital intracranial germinal layer neoplasms. Neuroradiology. 1985. 27: 301-3
4. Erdem G, Topçu M, Topaloğlu H, Bertan V, Arikan U. Dermoid tumor with persistently low CSF glucose and unusual CT and MRI findings. Pediatr Neurol. 1994. 10: 75-7
5. French BN, Youmans JR.editors. Midline fusion defects and defects of formation. Neurological Surgery. Philadelphia, PA: Saunders; 1990. p. 1164-69
6. Goffin J, Plets C, Van Calenbergh F, Weyns F, Van Havenbergh T, Eeckels R. Posterior fossa dermoid cyst associated with dermal fistula: Report of 2 cases and review of the literature. Childs Nerv Syst. 1993. 9: 179-81
7. Groen RJ, van Ouwerkerk WJ. Cerebellar dermoid tumor and occipital meningocele in a monozygotic twin: Clues to the embryogenesis of craniospinal dysraphism. Childs Nerv Syst. 1995. 11: 414-7
8. Guidetti V, Gagliardi FM. Epidermoid and dermoid cysts. Clinical evaluation and late surgical results. J Neurosurg. 1977. 47: 12-8
9. Hashmi S, Jones RA. Delayed recurrence of cerebellar abscess 20 years after excision of dermoid cyst and sinus. Br J Neurosurg. 1998. 12: 358-60
10. Hayek G, Mercier P, Fournier HD, Menei P, Pouplard F, Guy G. Dermal sinus and dermoid cyst revealed by abscess formation in posterior fossa. Report of 2 pediatric cases and review of the litterature. Neurochirurgie. 2001. 47: 123-7
11. Higashi S, Takinami K, Yamashita J. Occipital dermal sinus associated with dermoid cyst in the fourth ventricle. AJNR Am J Neuroradiol. 1995. 16: 945-8
12. Hsu ST, Lee JY, Chao SC, Hsieh MY, Huang CC. Congenital occipital dermal sinus with intracranial dermoid cyst complicated by recurrent Escherichia coli meningitis. Br J Dermatol. 1998. 139: 922-4
13. Karagöz Güzey F, Bas NS, Sencer A, Emel E, Hamamcioglu MK, Ozkan N. Posterior fossa dermoid cysts causing cerebellar abscesses. Pediatr Neurosurg. 2007. 43: 323-6
14. Lepintre J, Labrune M. Congenital dermal fistulae communicating with the central nervous system. 21 operated cases in children. Neurochirurgie. 1970. 16: 335-48
15. Logue V, Till K. Posterior fossa dermoid cysts with special reference to intracranial infection. J Neurol Neurosurg Psychiatry. 1952. 15: 1-12
16. Lunardi P, Missori P, Gagliardi FM, Fortuna A. Dermoid cysts of the posterior cranial fossa in children. Report of nine cases and review of the literature. Surg Neurol. 1990. 34: 39-42
17. Martens F, Ectors P, Noel P, Hanquinet S, Faverly D. Unusual cause of cerebellar abscess: Occipital dermal sinus and dermoid cyst. Neuropediatrics. 1987. 18: 107-9
18. Martin J, Davis L. Intracranial dermoid and epidermoid tumors. Arch Neurol Psychiatry (Chicago). 1943. 49: 56-70
19. Martínez-Lage JF, Capel A, Costa TR, Perez-Espejo MA, Poza M. The child with a mass on its head: Diagnostic and surgical strategies. Childs Nerv Syst. 1992. 8: 247-52
20. Martínez-Lage JF, Ramos J, Puche A, Poza M. Extradural dermoid tumours of the posterior fossa. Arch Dis Child. 1997. 77: 427-30
21. Matson DD, Ingraham FD. Intracranial complications of congenital dermal sinuses. Pediatrics. 1951. 8: 463-74
22. Mount LA. Congenital dermal sinuses as a cause of meningitis, intraspinal abscess and intracranial abscess. J Am Med Assoc. 1949. 139: 1263-8
23. Pennybacker J, Tytus JS. Pearly tumours in relation to the central nervous system. J Neurol Neurosurg Psychiatry. 1956. 19: 241-59
24. Roberts AP. A case of intracranial dermoid cyst associated with the Klippel-Feil deformity and recurrent meningitis. Arch Dis Child. 1958. 33: 222-5
25. Rubin G, Scienza R, Pasqualin A, Rosta L, Da Pian R. Craniocerebral epidermoids and dermoids. A review of 44 cases. Acta Neurochir (Wien). 1989. 97: 1-16
26. Schijman E, Monges J, Cragnaz R. Congenital dermal sinuses, dermoid and epidermoid cysts of the posterior fossa. Childs Nerv Syst. 1986. 2: 83-9
27. Smith AS, Benson JE, Blaser SI, Mizushima A, Tarr RW, Bellon EM. Diagnosis of ruptured intracranial dermoid cyst: Value MR over CT. AJNR Am J Neuroradiol. 1991. 12: 175-80
28. Smith GF, Altman DH. Occipital dermal sinus; clinical and radiological findings when a complete occipital dermal sinus is associated with a dermoid cyst. AMA J Dis Child. 1959. 9: 713-9
29. Starinsky R, Wald U, Michowitz SD, Lahat E, Schiffer J. Dermoids of the posterior fossa. Case reports and review. Clin Pediatr (Phila). 1988. 27: 579-82
30. Tekkök IH, Baeesa SS, Higgins MJ, Ventureyra EC. Abscedation of posterior fossa dermoid cysts. Childs Nerv Syst. 1996. 12: 318-22
31. Vinchon M, Lejeune JP, Krivosic I, Assaker R, Pruvo JP, Christiaens JL. Cranio-cerebral dermoid and epidermoid cysts. Classification and pathogenesis. Neurochirurgie. 1995. 41: 29-37
32. Wiemer DR. An occipital dermoid tumor and sinus. Ann Plast Surg. 1988. 21: 465-7
33. Wright RL. Congenital dermal sinuses. Prog Neurol Surg. 1971. 4: 175-91
34. Yaşargil MG, Abernathey CD, Sarioglu AC. Microneurosurgical treatment of intracranial dermoid and epidermoid tumors. Neurosurgery. 1989. 24: 561-7

