

- Department of Clinical Neurosciences, Cumming School of Medicine, University of Calgary, Calgary, Canada,
- Department of Surgery, Division of Neurosurgery, College of Medicine, King Saud University, Riyadh, Saudi Arabia,
- Department of Clinical Neurosciences, Hotchkiss Brain Institute, Canada.
- Department of Clinical Neurosciences, Arnie Charbonneau Cancer Institute, University of Calgary, Calgary, Canada.
Correspondence Address:
Garnette R. Sutherland
Department of Clinical Neurosciences, Cumming School of Medicine, University of Calgary, Calgary, Canada,
DOI:10.25259/SNI_660_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Abdulrahman Albakr1,2, Nicholas Sader1, Sanju Lama1,3,4, Garnette R Sutherland1,3,4. Interhemispheric arachnoid cyst. 30-Mar-2021;12:125
How to cite this URL: Abdulrahman Albakr1,2, Nicholas Sader1, Sanju Lama1,3,4, Garnette R Sutherland1,3,4. Interhemispheric arachnoid cyst. 30-Mar-2021;12:125. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=10686
Date of Submission
19-Sep-2020
Date of Acceptance
24-Feb-2021
Date of Web Publication
30-Mar-2021
Abstract
Background: Interhemispheric arachnoid cysts are uncommon and typically associated with other midline neurodevelopmental disorders, such as complete or partial agenesis of the corpus callosum.
Case Description: We report a case of a 27-year-old woman with worsening headache, memory deficit, and radiological progression of an interhemispheric arachnoid cyst. The treatment consisted of craniotomy for interhemispheric cyst fenestration into both the interhemispheric cistern and lateral ventricle. The postoperative course was unremarkable, with considerable clinical improvement and significant reduction in cyst size.
Conclusion: We successfully treat a patient with an enlarging arachnoid cyst and associated progressive symptoms with microsurgical fenestration.
Keywords: Arachnoid cyst, Corpus callosum, Interhemispheric fissure, Microsurgery
INTRODUCTION
Intracranial arachnoid cysts classically involve the middle cranial fossa.[
Here, we report a case of a large interhemispheric arachnoid cyst successfully treated with microsurgical fenestration.
CASE PRESENTATION
A 27-year-old woman was referred to our neurosurgical clinic in early 2019 with worsening headache and short-term memory deficit. Neurological examination revealed no mental status or cranial nerve abnormalities. She was previously diagnosed with a primary interhemispheric arachnoid cyst in 2012 following syncope. At that time, the cyst was small and presumed incidental. The most recent brain magnetic resonance imaging (MRI) scan showed a large interhemispheric arachnoid cyst with partial agenesis of the corpus callosum. The lesion had grown significantly compared to her initial MRI study, with associated ventriculomegaly [
Video 1
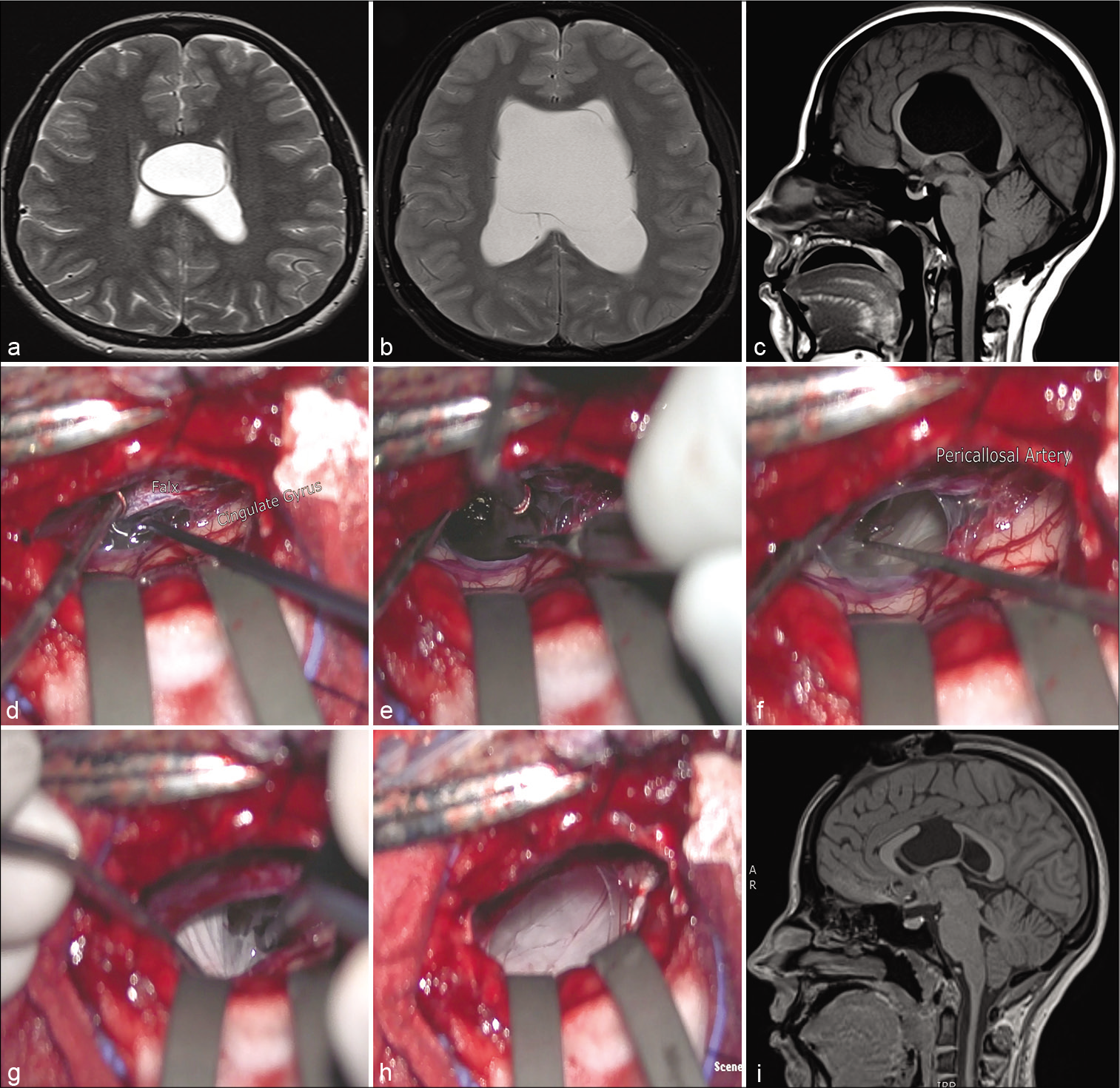
Figure 1:
(a) Initial T2-weighted axial magnetic resonance imaging (MRI) scan showing an interhemispheric arachnoid cyst with partial agenesis of the corpus callosum. (b and c) Preoperative T1 sagittal and T2 axial MRI scan showing the enlarging cyst with partial agenesis of the corpus callosum and ventriculomegaly. (d-h) Intraoperative microscopic views. (d) View from a right interhemispheric approach showing the falx cerebri, cingulate gyrus, and upper surface of the cyst. (e and f) Fenestration of the upper surface of the cyst with a view of the pericallosal arteries. (g) After incising and draining the cyst, fenestration was performed in the ventricular system. (h) View of the lateral ventricle following fenestration into both the interhemispheric cistern and lateral ventricle with dilation of the cyst wall. (i) Follow-up T1 sagittal MRI scan 5 months after the microscopic fenestration showing a successful surgical decompression with a decrease in the cyst and ventricle size.
At the follow-up visit 3 months later, she reported substantial improvement in her headache and memory issues. A follow-up MRI scan 5 months after the surgery demonstrated successful surgical decompression with a decrease in cyst and ventricle size [
DISCUSSION
Interhemispheric fissure arachnoid cysts are uncommon congenital abnormalities, and only a few cases have been reported.[
Controversy exists regarding surgical options. Yamasaki et al. reported an interhemispheric arachnoid cyst in an elderly patient, along with a literature review of similar cases.[
CONCLUSION
Interhemispheric arachnoid cysts are rare in adults, with few reports in the literature. We successfully treated an adult patient with an enlarging interhemispheric arachnoid cyst and progressive symptoms with microsurgical fenestration.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos available on:
www.surgicalneurologyint.com
References
1. Al-Holou WN, Terman S, Kilburg C, Garton HJ, Muraszko KM, Maher CO. Prevalence and natural history of arachnoid cysts in adults. J Neurosurg. 2013. 118: 222-31
2. Cinalli G, Peretta P, Spennato P, Savarese L, Varone A, Vedova P. Neuroendoscopic management of interhemispheric cysts in children. J Neurosurg. 2006. 105: 194-202
3. Deopujari CE, Shaikh ST, Karmarkar VS, Sudke AY, Mohanty CB, Biyani NK. Experience with management of intracranial arachnoid cysts. J Neurol Surg A Cent Eur Neurosurg. 2021. 82: 43-52
4. Gangemi M, Seneca V, Colella G, Cioffi V, Imperato A, Maiuri F. Endoscopy versus microsurgical cyst excision and shunting for treating intracranial arachnoid cysts. J Neurosurg Pediatr. 2011. 8: 158-64
5. Helland CA, Lund-Johansen M, Wester K. Location, sidedness, and sex distribution of intracranial arachnoid cysts in a population-based sample. J Neurosurg. 2010. 113: 934-9
6. Hirohata M, Matsuo H, Miyagi J, Kajihara K, Shigemori M, Kuramoto S. Interhemispheric arachnoid cyst; report of three cases. No Shinkei Geka. 1992. 20: 701-5
7. Hishikawa T, Chikama M, Tsuboi M, Yabuno N. Two cases of symptomatic arachnoid cysts in elderly patients-a comparison and analysis with child cases. No Shinkei Geka. 2002. 30: 959-65
8. Jakubiak P, Dunsmore RH, Beckett RS. Supratentorial brain cysts. J Neurosurg. 1968. 28: 129-36
9. Karabatsou K, Hayhurst C, Buxton N, O’Brien DF, Mallucci CL. Endoscopic management of arachnoid cysts: An advancing technique. J Neurosurg. 2007. 106: 455-62
10. Kotil K, Balci N, Bilge T. Intracranial symptomatic giant arachnoid cyst of the interhemispheric fissure presenting with frontal lobe syndrome. Turk Neurosurg. 2007. 17: 147-51
11. Matsuda M, Hirai O, Munemitsu H, Kawamura J, Matsubayashi K. Arachnoid cysts-report of two adult cases in the interhemispheric fissure and over the cerebral convexity. Neurol Med Chir (Tokyo). 1982. 22: 71-6
12. Novak Z, Chrastina J, Nadvornik P. Is interhemispheric arachnoid cyst with corpus callosum agenesis related to cavum vergae cyst?. Bratisl Lek Listy. 2006. 107: 435-8
13. Spennato P, Ruggiero C, Aliberti F, Buonocore MC, Trischitta V, Cinalli G. Interhemispheric and quadrigeminal cysts. World Neurosurg. 2013. 79: S20.e1-7
14. Tomabechi M, Takano K, Suzuki N, Daita G. A case of symptomatic interhemispheric arachnoid cyst in the elderly. No Shinkei Geka. 1999. 27: 377-81
15. Watanabe M, Kameyama S, Takeda N, Tanaka R. Two cases of symptomatic interhemispheric arachnoid cyst in the elderly. Surg Neurol. 1994. 42: 346-51
16. Yamasaki F, Kodama Y, Hotta T, Taniguchi E, Eguchi K, Yoshioka H. Interhemispheric arachnoid cyst in the elderly: Case report and review of the literature. Surg Neurol. 2003. 59: 68-74


