

- Institute of Neurology and Neurosurgery, Hospital Zambrano Hellion, San Pedro Garza García, N.L., México.
DOI:10.25259/SNI-217-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Jose A. Figueroa-Sanchez, Ana S. Ferrigno, Mario Benvenutti-Regato, Enrique Caro-Osorio, Hector R. Martinez. Internal jugular phlebectasia: A systematic review. 19-Jun-2019;10:106
How to cite this URL: Jose A. Figueroa-Sanchez, Ana S. Ferrigno, Mario Benvenutti-Regato, Enrique Caro-Osorio, Hector R. Martinez. Internal jugular phlebectasia: A systematic review. 19-Jun-2019;10:106. Available from: http://surgicalneurologyint.com/surgicalint-articles/9378/
Date of Submission
04-Apr-2019
Date of Acceptance
01-May-2019
Date of Web Publication
19-Jun-2019
Abstract
Background: Internal jugular phlebectasia (IJP), the abnormal dilatation of internal jugular vein, is generally considered a benign anomaly. However, because IJP is uncommon, little is known about its natural history, and currently, no consensus on the best treatment modality is available.
Methods: The purpose of this article is to conduct a systematic review of available literature on recently reported IJP cases to understand the main characteristics of IJP and its most frequent therapeutic approaches. Following the preferred reporting items for systematic reviews and meta-analyses guidelines, literature search for IJP cases was conducted in the COCHRANE, PUBMED, EBSCOHOST, SCOPUS, OVID, and SCIELO databases.
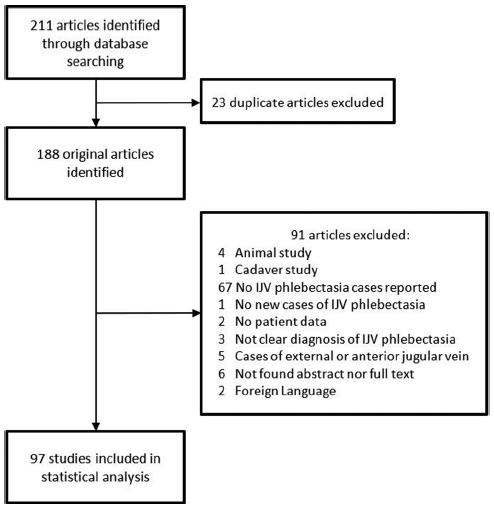
Results: A total of 97 original articles were found, with a total of 247 IJP cases reported including both pediatric and adult patients.
Conclusions: To the best of our knowledge, this study is the largest systematic review analyzing all the reported cases of IJP. IJP is considered by most authors as a benign abnormality that predominantly affects the right jugular vein. It is most commonly diagnosed in children. At present, conservative treatment is preferred for pediatric but not for adult patients. Multicenter randomized prospective studies are required to further understand this rare anomaly.
Keywords: Internal jugular vein, Neck mass, Phlebectasia, Venous dilatation
INTRODUCTION
Internal jugular phlebectasia (IJP), a nontortuous dilatation of the internal jugular vein (IJV), is typically considered a benign anatomical variant of unknown etiology.[
In literature, multiple terms have been applied to describe IJP such as venoma, venous cyst, venous aneurysm, and venous ectasia.[
METHODS
Following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines,[
RESULTS
Following PRISMA guidelines, a total of 97 articles were included in the analysis [
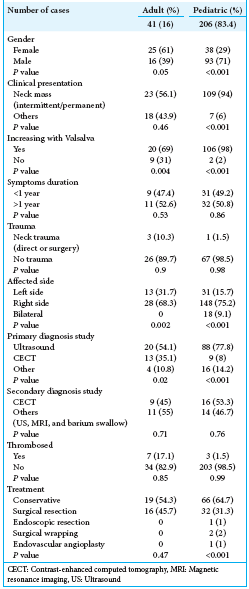
We found that IJP predominantly affected the pediatric population, with 206 patients (83.4%) younger than 18 years and only 41 adult cases (P < 0.001) reported in literature. The mean age of presentation was 47.8 years in adults (range: 17–74 years) and 6.4 years in pediatric patients (range: 6 weeks–15 years). The sex most affected was female in the adult group (61%) and male in the pediatric group (71%).
The duration of symptoms before diagnosis was not significantly different between adult and pediatric patients. Adult IJP symptoms manifested predominantly as the presence of a permanent neck mass in 12 cases (29.4%), an intermittent neck mass in 11 (26.8%), an incidental neck mass in 9 (22%), voice changes and neck pressure in 2 cases each (9.8%), neck tenderness, neck pain, and hemoptysis, chest discomfort, and right shoulder weakness in one case each. Pediatric patients predominantly presented intermittent neck masses in 67 patients (57.8%), permanent neck masses in 42 cases (36.2%), voice changes in 2 (1.5%), and neck tenderness, acute venous hypertension symptoms dysphagia, Horner’s syndrome, and otorrhea-otalgia in one case each. The Valsalva maneuver in both groups showed augmentation of the mass in 126 patients (92%) and no change in 11 patients (8%).
A history of head or neck trauma in both groups was reported in 97 patients. Only 4.1% of cases were related to direct trauma or surgery, and the proportion of this association in adults was higher than in pediatric patients but was not statistically significant.
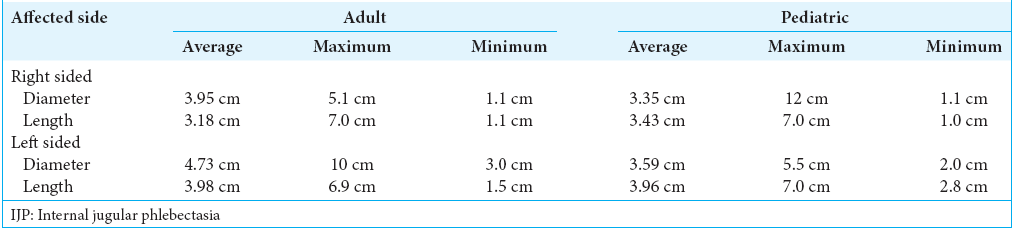
IJP affected the right side in 176 patients (73.9%) and the left side in 44 patients (18.5%), and in 18 patients (7.6%), IJP showed bilateral involvement. Right-sided predominance was similar in adult and pediatric patients. IJP measurements were described in 84 of the 247 patients, of which 29 corresponded to the adult population and 55 were pediatric cases. The average dimensions are summarized in
In just 150 of 247 cases, the primary diagnostic study was reported. Ultrasound (US) was employed for 108 patients (72%) as the primary study, a percentage that was higher in the pediatric population compared with that in adult patients. A contrast-enhanced computed tomography (CECT) was performed on 22 patients (14.6%), venography on 8 patients (5.3%), angiography on 4 patients (2.7%), magnetic resonance imaging (MRI) on 3 patients (2%), xenography on 2 patients (1.3%), and cinefluorographic studies, plain X-ray, and scintigraphy 99mTc-fibrinogen on 1 patient each (0.7%). The most common secondary study was CECT in 25 cases, MRI in 13 cases, US in 7 cases, barium swallow in 4, and unenhanced CT in 1 (2%). Secondary invasive studies were venography in 22 cases and angiography in 10 cases.
The treatment most frequently reported was a conservative approach in 85 patients (62%); however, the proportion of patients treated conservatively in the pediatric population was greater than that in the adult population. In the adult group for whom the treatment was described, no complications were found during conservative treatment, and complications from surgical resection were reported in 4 (11.4%) patients (P < 0.001): massive hemorrhage in 2 cases and paralysis of the left vocal cord and incomplete surgical resection in one case each. In the pediatric population, 102 patients had their treatment described. No complications were found during conservative treatment, and two (2%) patients had surgical complications (P < 0.001). The complications were subjective congestion of the left side of the head for 24 h after surgery and a postoperative transient increase in blood pressure. One patient treated conservatively died 14 months later due to Menkes disease complications.
DISCUSSION
IJP remains an infrequently diagnosed vascular anomaly. Although it is becoming increasingly recognized, partly due to improved diagnostic techniques,[
IJP is classically found unilaterally, although a few bilateral cases have been reported. In this review, bilateral IJP was only found in a few pediatric cases. IJP is most commonly found incidentally during a physical examination as a mass in the neck that increases with common efforts such as talking, coughing, or swallowing. Other symptoms include voice alterations, paralysis of the vocal cords, and/or dysphagia, all of which are caused by the proximity of the vagus nerve and other lower cranial nerves to the IJP.[
Multiple pathologies affecting the neck are considered to be differential diagnoses, especially laryngocele, branchial cyst, cystic hygroma, hemangioma, and paraganglioma.[
Although the etiology of IJP is not completely understood, some authors have suggested previous direct neck injuries or medical procedures such as central venous catheterization, positive-pressure ventilation, neck surgeries, or tumors.[
Histopathological changes in those cases treated with surgical resection include a thinning of the muscular and elastic layers; however, the great majority of cases showed no significant changes compared with the normal venous wall.[
IJP most commonly presents as a unilateral right-sided anomaly.[
The image study most frequently used for the diagnosis of IJP is US, with color Doppler as the study of choice to confirm the flow. This study continues to be useful because it is safe, feasible, sensitive, and of low cost. Other studies, such as MRI or CT, are usually helpful in complementing the diagnosis. Invasive studies such as angiography and venography are less commonly used, with only 10 (4%) and 22 (9%) cases, respectively, diagnosed by such methods.
Classically, IJP has been considered a benign entity; however, a serious possible complication resulting from abnormal vascular flow is thrombosis. In this review, the presentation of this complication was more frequent in adults, with 7 (17.1%) cases reported in literature, than in pediatric patients, with only 3 (1.5%) cases. Some authors describe Horner syndrome[
Conservative treatment was most frequently reported for IJP in the pediatric population, given it is classically considered a benign vascular abnormality. In adults, surgical resection was selected in almost the same proportion as conservative treatment. Alternative treatments consisted of endovascular angioplasty, surgical wrapping, and endoscopic resection, but these were only performed on the pediatric population. In general, the clinical outcome in both groups was described as good, although the follow-up was not described in a standardized manner. Descriptions of surgical treatment revealed a complication rate of 6.9% in the pediatric population and 11.4% in the adult population. In the cases treated conservatively, no complications were reported in either group. In general, conservative treatment was a safer option than surgical treatment in both groups.
CONCLUSIONS
Following PRISMA guidelines, we analyzed a total of 247 patients with IJP, including pediatric and adult patients. Due to the low incidence of this abnormality, there are not enough original prospective studies to perform a meta-analysis. In the analyzed papers, not all the studied variables were described, and the heterogeneity of the reports prevented the homologation of the variables. However, we conducted a systematic review, in which we compiled all the available literature at the present time including all reported cases in the English and Spanish literature. IJP is considered by most authors to be a benign abnormality, is most frequently found in children, and it affects predominantly the right IJV. The clinical outcome in most cases was benign regardless of the treatment, which was either conservative or surgical. Conservative treatment is preferred for children but not for adults. To the best of our knowledge, this is the largest review of IJP to date. Future prospective multicenter studies that study diagnostic and treatment options are necessary to be able to develop guidelines on approaching this vascular abnormality.


Beth Kenavan
Posted November 5, 2019, 9:40 pm
I have this phenomenon. Are there any further studies that I could volunteer to participate in?