

- Department of Neurosurgery, Instituto Clavel, San Francisco De Asis University Hospital, Madrid, Spain
- Department of Microbiology, Principe de Asturias University Hospital, Madrid, Spain
- Department of Neurosurgery, Fundacion Jimenez Diaz University Hospital, Madrid, Spain
- Department of Pathology, Infanta Elena University Hospital, Valdemoro, Spain
- Department of Pathology, Fundacion Jimenez Diaz University Hospital, Madrid, Spain.
- Internal Medicine, Fundacion Jimenez Diaz University Hospital, Madrid, Spain.
- Radiology, Fundacion Jimenez Diaz University Hospital, Madrid, Spain.
Correspondence Address:
Pablo Barbero-Aznarez, Department of Neurosurgery, Instituto Clavel, San Francisco De Asis University Hospital, Madrid, Spain.
DOI:10.25259/SNI_591_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Pablo Barbero-Aznarez1, Ramon Perez-Tanoira2, Daniel Aguirre-Mollehuanca3, Alvaro Trascasa-Caño4, Jose Fortes-Alen5, Felix Manzarbeitia-Arrambari5, Jorge Castillo-Alvarez6, Julia Montoya-Bordon7, Elizabet Petkova-Saiz6, Laura Prieto-Perez6. Isolated central nervous system Whipple disease. Surg Neurol Int 21-Oct-2022;13:477
How to cite this URL: Pablo Barbero-Aznarez1, Ramon Perez-Tanoira2, Daniel Aguirre-Mollehuanca3, Alvaro Trascasa-Caño4, Jose Fortes-Alen5, Felix Manzarbeitia-Arrambari5, Jorge Castillo-Alvarez6, Julia Montoya-Bordon7, Elizabet Petkova-Saiz6, Laura Prieto-Perez6. Isolated central nervous system Whipple disease. Surg Neurol Int 21-Oct-2022;13:477. Available from: https://surgicalneurologyint.com/surgicalint-articles/11948/
Date of Submission
30-Jun-2022
Date of Acceptance
19-Sep-2022
Date of Web Publication
21-Oct-2022
Abstract
Background: Whipple disease (WD) is an infection caused by Tropheryma whipplei, which might present in three different forms: classical, localized, and isolated in the central nervous system (CNS).
Methods: We report the result of a systematic review of the literature on WD unusually presenting with exclusively neurological symptoms, including two previously unpublished cases. A description of two cases with isolated CNS WD was performed, as well as a literature search in Cochrane, Scielo, and PubMed.
Results: Two male adult patients presented with exclusively neurological symptomatology. Both magnetic resonance imaging (MRI) showed an intracranial mass suggestive of brain tumor. The histopathological examination was consistent with WD, with no systemic involvement. In the review of the literature, 35 cases of isolated CNS WD were retrieved. The median age at diagnosis was 43.5 (IQR 31.5–51.5). In 13 patients, the MRI showed a brain mass consistent with a brain tumor. The most common finding in the biopsy was the periodic-acid Schiff-stained foamy macrophages. Only five cases presented the pathognomonic sign of oculomasticatory myorhythmia. Thirteen cases had an adverse outcome that resulted in death during follow-up, whereas another 13 improved. The other nine patients remained stable or presented moderate improvement.
Conclusion: Isolated CNS WD is a rare disease that should be considered among the differential diagnosis of CNS mass lesions. Brain biopsy is necessary to establish the diagnosis. It is stressed in the literature that an extended antibiotic course is required to prevent relapses and to control the disease.
Keywords: Brain tumor, Cerebral mass, Infection, Tropheryma whipplei, Whipple disease
INTRODUCTION
The central nervous system (CNS) in Whipple disease (WD) might be involved in three different situations: CNS involvement in classic WD, CNS relapse in previously treated WD, and isolated CNS infection.[
T. whipplei-infected macrophages contain particles that stain positive with periodic acid-Schiff (PAS).[
MATERIALS AND METHODS
Besides describing two previously unpublished cases of WD presenting with focal brain lesions, a systematic review of the literature was conducted to identify all reported cases of WD presenting with exclusively CNS lesions, which were identified in PubMed (
The following search strategy was used “(WD or T. whipplei) AND (Central Nervous System OR CNS) AND (brain OR mass).” In Scielo search tool, the research was limited to abstract, keywords, and title, while no restriction was included in PubMed search tool.
Selection: The authors screened articles found by electronic search and evaluated their appropriateness based on title and abstract according to the established criteria. Articles were selected if they reported original data on laboratory confirmed WD cases presenting with brain focal lesions detected by any diagnostic tool (computed tomography [CT] scan, magnetic resonance imaging [MRI], CT Positron emission tomography, and lumbar puncture). Exclusion criteria were: (1) studies concerning WD with gastrointestinal or systemic disease; (2) in vitro studies; (3) basic research; (4) articles with full text written in languages other than that of at least one of the members of the team could read and understand (namely English, French, and Spanish); (5) only radiological findings or descriptions; and (6) spinal affection. If the eligibility of the documents could not be ascertained according to the abstract and title only, the full text was analyzed to exclude or include the document. The reference lists of all included articles were systematically reviewed for additional relevant documents to add.
Two cases
Case 1
A 51-year-old man was admitted because of dysnomia, blurred vision, and gait instability for the previous 3 days. Two months before admission, he noticed semantic paraphasias, a right visual field defect and difficulty in concentration. His previous medical history was remarkable for type I diabetes mellitus since he was 22 years old and hypercholesterolemia. He had been diagnosed with idiopathic hypersomnia and suffered from Achilles tendonitis in 2015. He received follow-up for an isolated pulmonary nodule. He was otherwise healthy and fulfilled a Mediterranean diet. The patient is a musician, so reading sheet music and composing new pieces posed a hard task. He never had fever nor bowel problems, but he had suffered from an irritative cough for the past year. He had travelled to the United States of America 10 years ago and to Portugal the previous year. He was receiving the following treatment: insulin, simvastatin, and salbutamol.
An MRI was then performed [
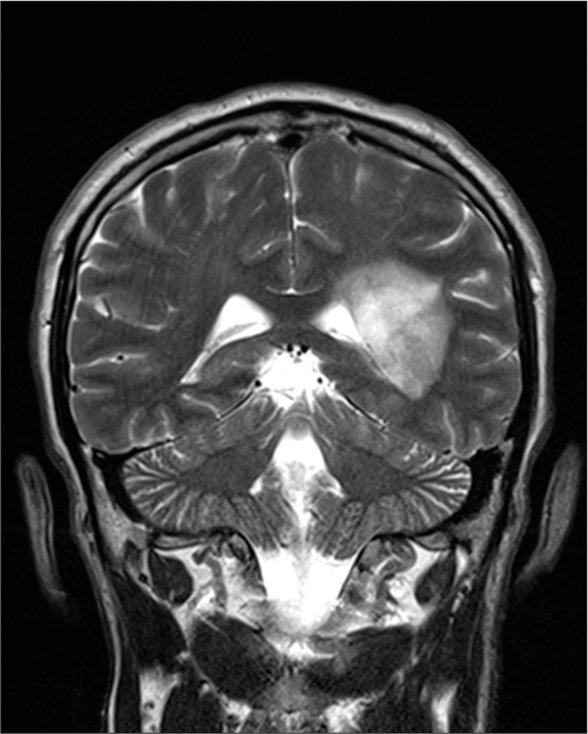
His neurological examination was remarkable for a motor language blockade with phonemic paraphasias and a right homonymous quadrantanopia. He did not improve with corticosteroid therapy. A full body computed tomography was performed to rule out a possible primary tumor, this being normal.
Surgical resection with craniotomy was then recommended with the presumptive diagnosis of glioblastoma. He was not considered to be a good candidate for awake brain surgery due to his language dysfunction.
The patient underwent brain biopsy and remained well with no new deficits after the procedure.
He was discharged and followed up at the outpatient department awaiting a definitive diagnosis.
Histopathological examination showed foamy histiocitary infiltration with intense PAS positive granular and rod-like cytoplasmic material, suggestive of WD [
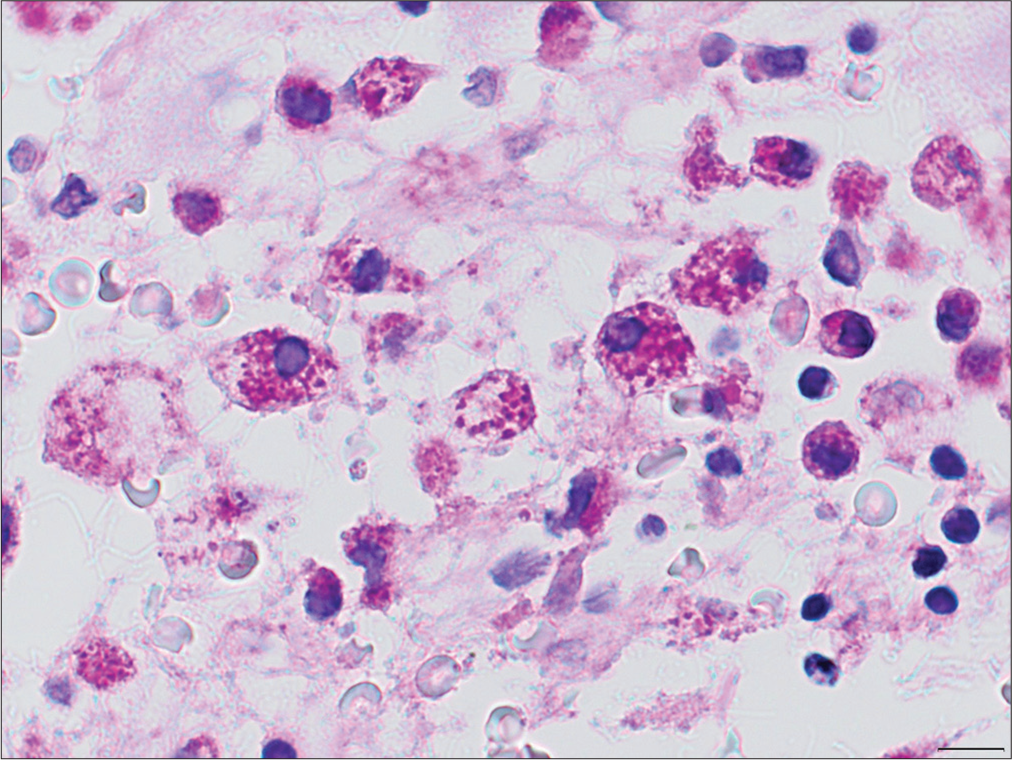
Figure 2:
×100 magnification. The samples were composed mainly by white matter and revealed an extensive infiltration by many perivascular foamy histiocytes which were immunoreactive for CD68 and CD163 and showed excentric, large, and “bean-like” nucleus within a wide, granular, and eosinophilic cytoplasm. PAS staining revealed intense and granular staining in the cytoplasm of the histiocytes. Zhiel staining was negative. Other findings of relevance were the presence of gliosis and small clusters of mature lymphocytes. No signs of malignancy were found.
According to Louis 1996 diagnostic criteria, he was diagnosed of WD with exclusive CNS involvement. Antibiotic therapy was then started with intravenous ceftriaxone and cotrimoxazole P.O. for a year.[
In the outpatient follow-up, his language and visual field improved. He only had occasional headaches. In the first 6-month follow-up, the MRI also showed an improvement with a decreased size and mass effect as well as a loss of contrast-enhancement. He was then assessed in the rehabilitation outpatient clinic, with no significant language dysfunction but an ejective dysfunction with difficulty in maintaining concentration and work memory. His auditive comprehension capabilities, planification, social chatting, and daily activities were affected. In his last MRI, there was a stable white matter lesion, left paraventricular in location, residual to an inflammatory lesion due to WD, and with slight enlargement of the adjacent atrium. There was no contrast-enhancement.
After 2-year follow-up, the patient remains well; he has now resumed his previous job as a music teacher. The main symptom he notices is the difficulty in composing new pieces of music.
He is progressively regaining his usual activities (musical composition) although he feels a bit insecure. He still occasionally gets confused with words. In this case, respecting the patient’s autonomy principle in preferring to undertake biopsy has permitted to reach the diagnosis with a low probability of sequelae.
Case 2
A 78-year-old-patient was referred because of a 4-day history of weakness in his left side that was most prominent in the left inferior limb. No sensitive, language, or visual defects were found in the physical examination. His medical history was remarkable for rheumatoid arthritis, and he was receiving chronic treatment with salazopyrine at a daily dose of 2 g.
A CT scan of the brain showed a mass located in the deep white matter of the right frontal lobe, which was suggestive of metastases. Sequences of perfusion in the MRI demonstrated that the focal mass in the white matter of right precentral corona radiata behaved like an inflammatory lesion.
A brain biopsy was performed; an interstitial histocyte infiltration at white matter and cortex was evident with microgranuloma formation and no necrosis, as well as bacillar cytoplasmic structures that were all consistent with WD.
No alterations were found in body computed tomography, upper and lower tract endoscopies, lumbar puncture, or multiplex PCR for CNS pathogens.
He received intravenous treatment with daily ceftriaxone for a month, and then cotrimoxazole 800/160 mg orally every 12 h for 1 year. At 2-year follow-up, the patient has partially recovered strength in his left lower limb and remains stable up to date, with significant improvement in MRI.
DISCUSSION
In about 5% of all patients with WD, the disease is isolated or primary.[
WD is most likely to affect Caucasian middle-aged (the median age at diagnosis was 43.5 [IQR 31.5–51.5]) men (8 men: 1woman) who live in rural areas (20) and are human leukocyte antigen-B27-positive.[
The bacterium has been isolated in duodenal (4.8%) and gastric (11.4%) biopsies of healthy carriers suggesting that it might be a commensal organism.[
Reduced pro-inflammatory cytokines associated with inflammatory macrophages have been implicated in the establishment of T. whipplei in the host.[
Exclusive confinement to the CNS is extremely rare.[
In a small study by Compain et al., mild weight loss in isolated CNS WD was described, as well as distinct patterns of brain MRI lesions: normal,[
The symptoms of cerebral WD include oculomotor abnormalities,[
The most reported CNS symptoms are cognitive changes, affecting 71% of patients with CNS manifestations.[
The brain lesions detected by computed tomography and MRI are particularly heterogeneous:[
MR imaging of neuroWD may be diverse,[
Louis et al. (1996) proposed diagnostic criteria for CNS WD. They consider a definite diagnosis if a patient meets at least one of three criteria:[
OMM or oculofacioskeletal myorhythmia A positive CNS tissue biopsy or a positive biopsy of another tissue associated with neurologic signs consistent with WD[ A positive PCR tissue.
Even though CNS WD is rare and challenging to diagnose,[
According to Delarbre et al., T. whipplei infection should be considered in the absence of clinical response or in case of worsening of inflammatory rheumatism under tumor necrosis factor inhibitor treatment, especially in case of atypical features.[
In the absence of PCR positivity, it is not possible to make a definitive isolated WD diagnosis. Although, supportive findings including the presence of rapidly progressive encephalitis[
Fenollar et al. proposed a classification system for chronic Whipple’s encephalitis patients. According to this system, patients with positive PCR of CSF and/or brain biopsy are regarded to have definite CNS WD and with positive staining of PAS and electron microscopy of brain biopsy is regarded to have possible isolated cerebral WD.[
Although there are no clear guidelines about the best first line therapy, one group with some of the most extensive clinical experience in the treatment of Whipple’s endocarditis recommends a combination of doxycycline plus hydroxychloroquine for treatment, which is the only bactericidal regimen in a tissue culture.[
To clear T. whippelii from the CNS, patients need primary treatment for 2 weeks with antibiotics that attain high CSF levels (e.g., ceftriaxone or penicillin G), followed by oral cotrimoxazole for 12 months.[
Since CNS relapses carry a poor prognosis, antibiotics should not be reduced or discontinued. They should be prescribed at least for 1 year to prevent relapses.[
The rate of relapse is particularly high with tetracycline (up to 35%) and one of the cases of chronically relapsing CNS Whipple’s was successfully treated with recombinant interferon along with conventional antibiotics.[
Several articles commented on the efficacy of trimethoprim– sulfamethoxazole and initial ceftriaxone treatment.[
In our review of the literature, we have found 35 cases of isolated CNS WD. They were published between 1975 and 2017. Twenty-two of them were men and 13 women. The mean age was 42 years old with a median of 43 years old. The most common signs and symptoms were cognitive impairment and memory loss, ataxia, seizures, cranial nerve palsies, nausea, behavioral change, headache, sleep disturbances,[
CONCLUSION
In the differential diagnosis of glioblastoma, we should consider anaplastic astrocytoma, toxoplasmosis, cavernoma, cerebral abscess, CNS lymphoma, encephalitis, intracranial hemorrhage, metastasis, oligodendroglioma, radionecrosis, and WD.
Isolated CNS WD is a clinical challenge and should be considered in the differential diagnosis in unusual cases of encephalitis. Brain biopsy is necessary to establish the diagnosis of isolated CNS WD. It is stressed in the literature that an extended antibiotic course is required to prevent relapses and to control the disease.[
Declaration of patient consent
Patients’ consent not required as patients’ identities were not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflict of interest
There are no conflicts of Interest.
References
1. Abreu PM, Azevedo EP, Lobo LA, Moura CS, Pontes CR. Cerebral Whipple disease without gastrointestinal symptoms. Rev Neurol. 2005. 40: 255
2. Adams M, Rhyner PA, Day J, DeArmond S, Smuckler EA. Whipple’s disease confined to the central nervous system. Ann Neurol. 1987. 21: 104-8
3. Anderson M. Neurology of Whipple’s disease. J Neurol Neurosurg Psychiatry. 2000. 68: 2-5
4. Bakkali N, Fenollar F, Biswas S, Rolain JM, Raoult D. Acquired resistance to trimethoprim-sulfamethoxazole during Whipple disease and expression of the causative target gene. J Infect Dis. 2008. 198: 101-8
5. Black DF, Aksamit AJ, Morris JM. MR imaging of central nervous system Whipple disease: A 15-year review. AJNR Am J Neuroradiol. 2010. 31: 1493-7
6. Compain C, Sacre K, Puéchal X, Klein I, Vital-Durand D, Houeto JL. Central nervous system involvement in Whipple disease: Clinical study of 18 patients and long-term follow-up. Medicine (Baltimore). 2013. 92: 324-30
7. Coria F, Cuadrado N, Velasco C, Carmena JJ, Jiménez MI, Mena FJ. Whipple’s disease with isolated central nervous system symptomatology diagnosed by molecular identification of Tropheryma whippeli in peripheral blood. Neurologia. 2000. 15: 173-6
8. De Coene B, Gilliard C, Indekeu P, Duprez T, Trigaux JP. Whipple’s disease confined to the central nervous system. Neuroradiology. 1996. 38: 325-7
9. Delarbre D, Gan L, Antoine C, Poisnel E, Cambon A, Dutasta F. Diagnostic issues of Whipple’s disease during chronic inflammatory rheumatism: About three cases. Rev Med Interne. 2021. 42: 801-4
10. Dönmez FY, Ulu E, Başaran C, Unlükaplan M, Uyuşur A, Yildirim M. MRI of recurrent isolated cerebral Whipple’s disease. Diagn Interv Radiol. 2010. 16: 112-5
11. Duprez TP, Grandin CB, Bonnier C, Thauvoy CW, Gadisseux JF, Dutrieux JL. Whipple disease confined to the central nervous system in childhood. AJNR Am J Neuroradiol. 1996. 17: 1589-91
12. Durand DV, Lecomte C, Cathébras P, Rousset H, Godeau P. Whipple disease Clinical review of 52 cases The SNFMI research group on Whipple disease. Société nationale française de médecine interne. Medicine (Baltimore). 1997. 76: 170-84
13. Dutly F, Altwegg M. Whipple’s disease and. “Tropheryma whippeli”. Clin Microbiol Rev. 2001. 14: 561-83
14. Fenollar F, Nicoli F, Paquet C, Lepidi H, Cozzone P, Antoine JC. Progressive dementia associated with ataxia or obesity in patients with Tropheryma whipplei encephalitis. BMC Infect Dis. 2011. 11: 171
15. Fenollar F, Rolain JM, Alric L, Papo T, Chauveheid MP, van de Beek D. Resistance to trimethoprim/sulfamethoxazole and Tropheryma whipplei. Int J Antimicrob Agents. 2009. 34: 255-9
16. Feurle GE, Junga NS, Marth T. Efficacy of ceftriaxone or meropenem as initial therapies in Whipple’s disease. Gastroenterology. 2010. 138: 478-86 quiz 11-2
17. Feurle GE, Marth T. An evaluation of antimicrobial treatment for Whipple’s disease. Tetracycline versus trimethoprimsulfamethoxazole. Dig Dis Sci. 1994. 39: 1642-8
18. Feurle GE, Moos V, Schinnerling K, Geelhaar A, Allers K, Biagi F. The immune reconstitution inflammatory syndrome in Whipple disease: A cohort study. Ann Intern Med. 2010. 153: 710-7
19. Feurle GE, Moos V, Schneider T, Fenollar F, Raoult D. The combination of chloroquine and minocycline, a therapeutic option in cerebrospinal infection of Whipple’s disease refractory to treatment with ceftriaxone, meropenem and co-trimoxazole. J Antimicrob Chemother. 2012. 67: 1295-6
20. Flanagan ME, Andeen N, Lieberman J, Freeburg J, Williams JR, Hoogestraat DR. An unusual case of a young patient with Whipple’s disease involving the central nervous system. Clin Neuropathol. 2017. 36: 199-204
21. Flemmer MC, Flenner RW. Current insights in Whipple’s disease. Curr Treat Options Gastroenterol. 2003. 6: 13-6
22. Frazier JL, Quinones-Hinojosa A. Isolated Whipple disease of the brain resembling a tumour. Acta Neurochir (Wien). 2009. 151: 173-5
23. Gerard A, Sarrot-Reynauld F, Liozon E, Cathebras P, Besson G, Robin C. Neurologic presentation of Whipple disease: Report of 12 cases and review of the literature. Medicine (Baltimore). 2002. 81: 443-57
24. Halperin JJ, Landis DM, Kleinman GM. Whipple disease of the nervous system. Neurology. 1982. 32: 612-7
25. Henning S, Tings T, Schmidt H, Tergau F, Wolf S, Scholz K. A case of cerebral Whipple’s disease initially presenting with isolated focal myoclonus. Eur J Neurol. 2006. 13: 659-61
26. Hens Pérez MJ, Bengoa JF, Ruíz-Cabello JM, Gutiérrez IN, Aceituno MP, Corcoles JQ. Whipple Disease: An infrequent bacterian cause of dementia in Spanish. Rev Asoc Esp Neuropsiq. 2009. 29: 535-8
27. Hurth K, Tarawneh R, Ghoshal N, Benzinger TL, Clifford DB, Geschwind M. Whipple’s disease masquerades as dementia with Lewy bodies. Alzheimer Dis Assoc Disord. 2015. 29: 85-9
28. Kitamura T. Brain involvement in Whipple’s disease: A case report. Acta Neuropathol. 1975. 33: 275-8
29. Knox DL, Green WR, Troncoso JC, Yardley JH, Hsu J, Zee DS. Cerebral ocular Whipple’s disease: A 62-year odyssey from death to diagnosis. Neurology. 1995. 45: 617-25
30. Kundu A, Sen P, Khurana S. Isolated CNS Whipple’s disease: A diagnostic dilemma. BMJ Case Rep. 2015. 2015: bcr2015211784
31. La Scola B, Fenollar F, Fournier PE, Altwegg M, Mallet MN, Raoult D. Description of Tropheryma whipplei gen. nov., sp. nov., the Whipple’s disease Bacillus. Int J Syst Evol Microbiol. 2001. 51: 1471-9
32. Lagier JC, Fenollar F, Lepidi H, Giorgi R, Million M, Raoult D. Treatment of classic Whipple’s disease: From in vitro results to clinical outcome. J Antimicrob Chemother. 2014. 69: 219-27
33. Lagier JC, Fenollar F, Lepidi H, Raoult D. Failure and relapse after treatment with trimethoprim/sulfamethoxazole in classic Whipple’s disease. J Antimicrob Chemother. 2010. 65: 2005-12
34. Le Blay P, Rakotonirainy H, Lagier JC, Raoult D, Puechal X, Pers YM. A severe Whipple disease with an immune reconstitution inflammatory syndrome: An additional case of thalidomide efficiency. Joint Bone Spine. 2014. 81: 260-2
35. Löhr M, Stenzel W, Plum G, Gross WP, Deckert M, Klug N. Whipple disease confined to the central nervous system presenting as a solitary frontal tumor. Case report. J Neurosurg. 2004. 101: 336-9
36. Louis ED, Lynch T, Kaufmann P, Fahn S, Odel J. Diagnostic guidelines in central nervous system Whipple’s disease. Ann Neurol. 1996. 40: 561-8
37. Louis ED. Whipple disease. Curr Neurol Neurosci Rep. 2003. 3: 470-5
38. Ludwig B, Bohl J, Haferkamp G. Central nervous system involvement in Whipple’s disease. Neuroradiology. 1981. 21: 289-93
39. Marth T, Raoult D. Whipple’s disease. Lancet. 2003. 361: 239-46
40. Mendel E, Khoo LT, Go JL, Hinton D, Zee CS, Apuzzo ML. Intracerebral Whipple’s disease diagnosed by stereotactic biopsy: A case report and review of the literature. Neurosurgery. 1999. 44: 203-9
41. Misbah SA, Aslam A, Costello C. Whipple’s disease. Lancet. 2004. 363: 654-6
42. Mohamed W, Neil E, Kupsky WJ, Juhász C, Mittal S, Santhakumar S. Isolated intracranial Whipple’s disease--report of a rare case and review of the literature. J Neurol Sci. 2011. 308: 1-8
43. Moos V, Feurle GE, Schinnerling K, Geelhaar A, Friebel J, Allers K. Immunopathology of immune reconstitution inflammatory syndrome in Whipple’s disease. J Immunol. 2013. 190: 2354-61
44. Moos V, Schmidt C, Geelhaar A, Kunkel D, Allers K, Schinnerling K. Impaired immune functions of monocytes and macrophages in Whipple’s disease. Gastroenterology. 2010. 138: 210-20
45. Panegyres PK, Edis R, Beaman M, Fallon M. Primary Whipple’s disease of the brain: Characterization of the clinical syndrome and molecular diagnosis. QJM. 2006. 99: 609-23
46. Peregrin J, Malikova H. Primary Whipple disease of the brain: Case report with long-term clinical and MRI follow-up. Neuropsychiatr Dis Treat. 2015. 11: 2461-9
47. Pollock S, Lewis PD, Kendall B. Whipple’s disease confined to the nervous system. J Neurol Neurosurg Psychiatry. 1981. 44: 1104-9
48. Posada IJ, Ferreiro-Sieiro A, López-Valdés E, Cabello A, Bermejo-Pareja F. Whipple’s disease confined to the brain. A clinical case with pathological confirmation at necropsy. Rev Neurol. 2004. 38: 196-8
49. Poureisa M, Daghighi MH, Esmaili H, Mazaheri-Khameneh R. Magnetic resonance imaging of Whipple’s disease confined to the CNS presenting with multiple intracerebral mass lesions. Acta Med Iran. 2015. 53: 250-5
50. Relman DA, Schmidt TM, MacDermott RP, Falkow S. Identification of the uncultured Bacillus of Whipple’s disease. N Engl J Med. 1992. 327: 293-301
51. Romanul FC, Radvany J, Rosales RK. Whipple’s disease confined to the brain: A case studied clinically and pathologically. J Neurol Neurosurg Psychiatry. 1977. 40: 901-9
52. Schneider T, Stallmach A, von Herbay A, Marth T, Strober W, Zeitz M. Treatment of refractory Whipple disease with interferon-gamma. Ann Intern Med. 1998. 129: 875-7
53. Street S, Donoghue HD, Neild GH. Tropheryma whippeli DNA in saliva of healthy people. Lancet. 1999. 354: 1178-9
54. Sung VW, Lyerly MJ, Fallon KB, Bashir K. Isolated CNS Whipple disease with normal brain MRI and false-positive CSF 14-3-3 protein: A case report and review of the literature. Brain Behav. 2012. 2: 838-43
55. Süzer T, Demirkan N, Tahta K, Coskun E, Cetin B. Whipple’s disease confined to the central nervous system: Case report and review of the literature. Scand J Infect Dis. 1999. 31: 411-4
56. Tábuas-Pereira M, Vicente M, Coelho F, Santana I. Prosopagnosia as the presenting symptom of Whipple disease. Cogn Behav Neurol. 2016. 29: 100-6
57. Vural A, Acar NP, Soylemezoglu F, Oguz KK, Dericioğlu N, Saka E. Isolated central nervous system Whipple’s disease: Two cases. Clin Neurol Neurosurg. 2015. 139: 91-4
58. Wroe SJ, Pires M, Harding B, Youl BD, Shorvon S. Whipple’s disease confined to the CNS presenting with multiple intracerebral mass lesions. J Neurol Neurosurg Psychiatry. 1991. 54: 989-92
59. Yu C, Jiang A, Yu Y. Serial imaging changes of cerebral Whipple’s disease: From onset to the end. J Neuroimaging. 2007. 17: 81-3

