

- Department of Neurosurgery, Centre Clinical de Soyaux, Soyuax, France,
- Department of Neurosurgery, Carl Thiem Klinikum, Cottbus, Germany.
Correspondence Address:
Keyvan Mostofi, Department of Neurosurgery, Centre Clinical de Soyaux, Soyuax, France.
DOI:10.25259/SNI_996_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Keyvan Mostofi1, Morad Peyravi2. Modified anterior retropharyngeal approach for C2-C3 disc herniation. 02-Dec-2022;13:568
How to cite this URL: Keyvan Mostofi1, Morad Peyravi2. Modified anterior retropharyngeal approach for C2-C3 disc herniation. 02-Dec-2022;13:568. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=12033
Date of Submission
30-Oct-2022
Date of Acceptance
21-Nov-2022
Date of Web Publication
02-Dec-2022
Abstract
Background: C2-C3 disc herniations are rare, but occur more frequent in the elderly population. As the classical anterior Cloward approach to these lesions is not optimal, we propose an alternative modified retropharyngeal approach to these disc herniations that were successfully utilized in two patients.
Methods: Two patients with C2-C3 disc herniations underwent anterior cervical surgery utilizing the modified retropharyngeal approach.
Results: Surgery was successful is two cases with C2-C3 disc herniation and no patient sustained a perioperative complication.
Conclusion: Our modified anterior retropharyngeal approach for C2-C3 disc herniations resulted in good outcomes without perioperative complications.
Keywords: Cervical disc herniation, Degenerative diseases, Spine surgery, Upper cervical instrumentation, Disc herniation
INTRODUCTION
C2-C3 disc herniation is rare. We were able to identify <50 such cases have in the literature.[
MATERIALS AND METHODS
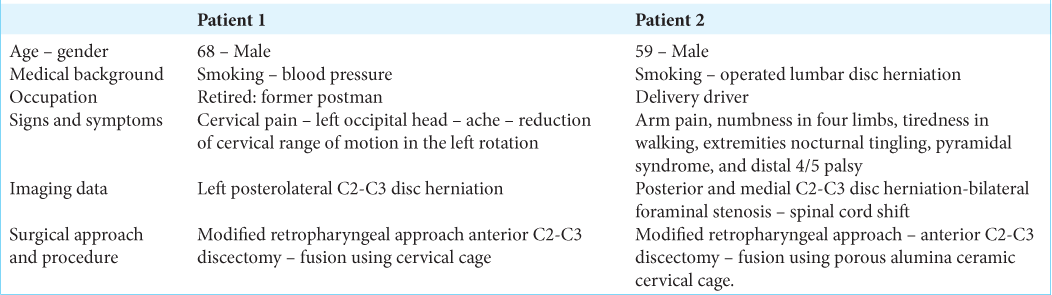
Two patients, ages 68 and 59, presented with C2-C3 disc herniations. The first patient had a cervical MRI that sowed a left posterolateral C2-C3 disc herniation compressing the C3 nerve root. He underwent a modified retropharygeal anterior C2-C3 discectomy/fusion using an intersomatic porous alumina ceramic cervical cage with good resolution of his pain a few weeks after surgery. The second patients cervical MRI demonstrated a posterior/central C2-C3 disc herniation with bilateral foraminal stenosis and cord compression but without a high intramedullary cord signal. He too had a modified retropharyngeal C2-C3 discectomy employing an intersomatic porous alumina ceramic cervical cage, and returned to work 2 months after surgery [
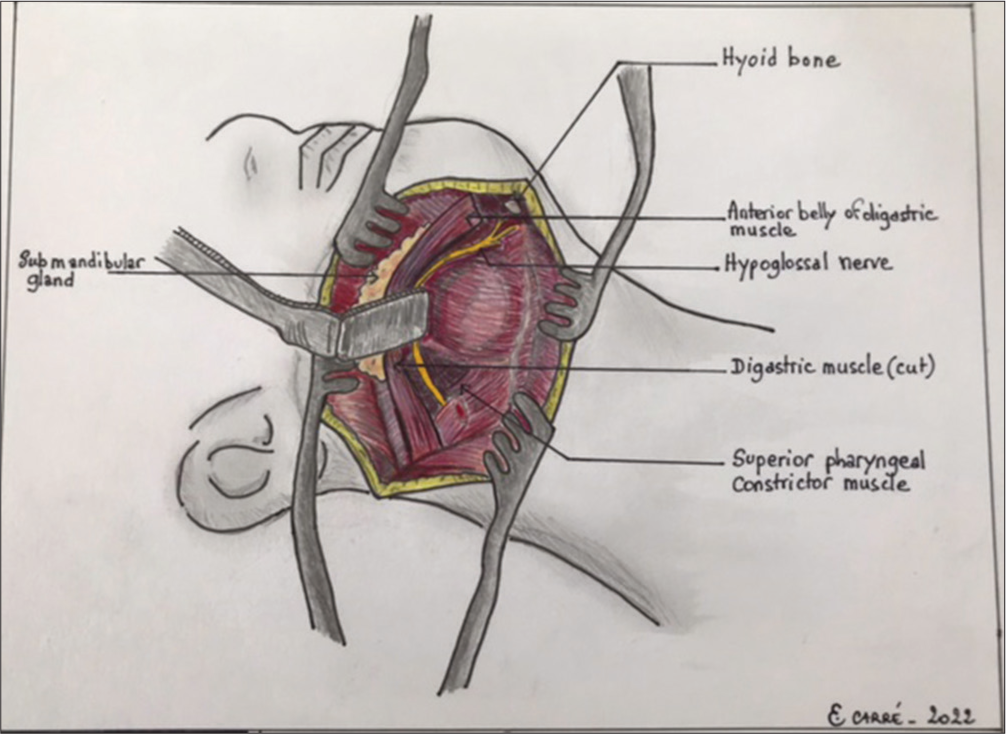
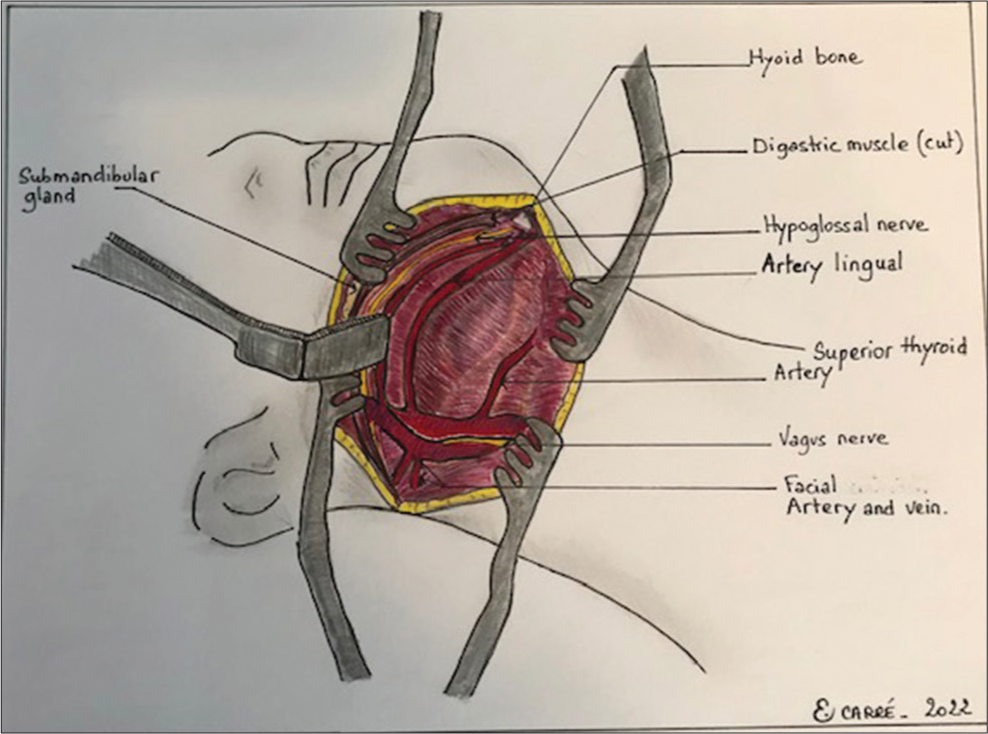
TECHNICAL NOTE: ANTERIOR-MODIFIED RETROPHARYNGEAL SURGICAL APPROACH TO C2-C3 DISC HERNIATIONS
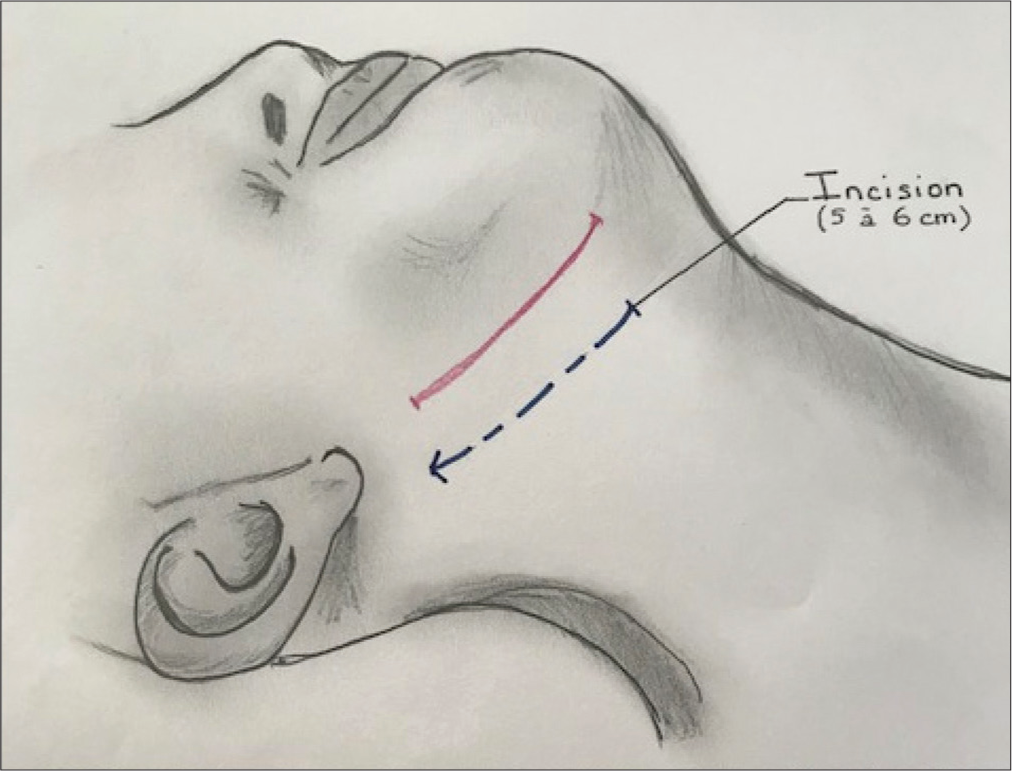
Patient is in supine position with the neck in extension and head fixed on a Mayfield headrest and rotated 45° to contralateral side. This approach utilized an oblique anterior incision parallel to the mandible [


DISCUSSION
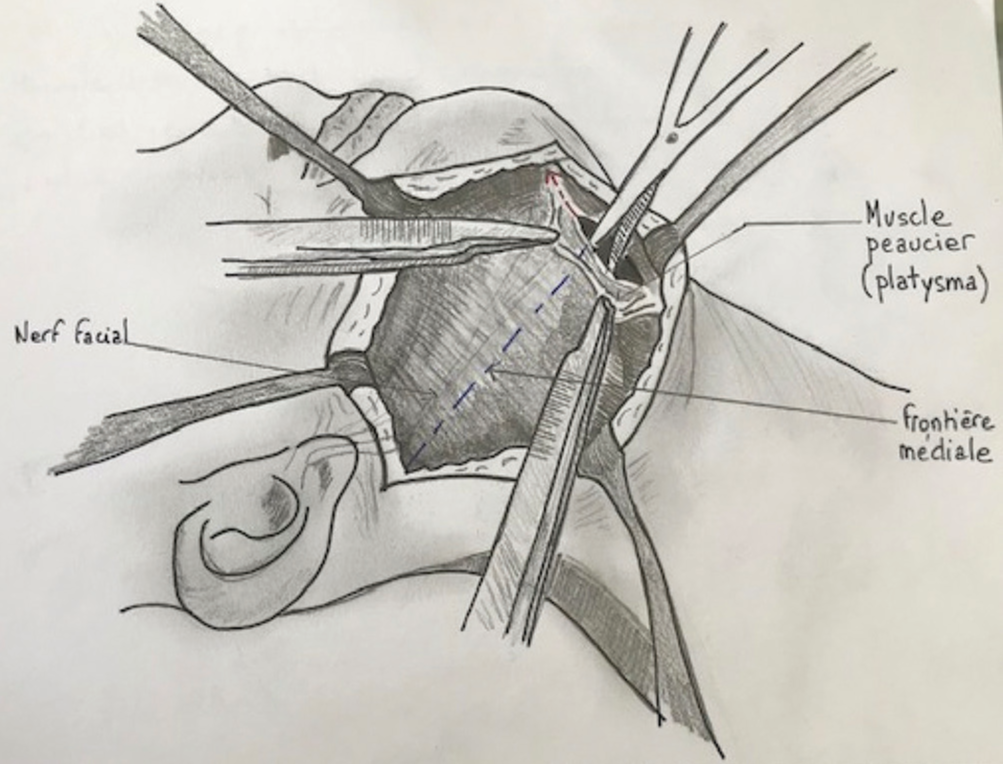
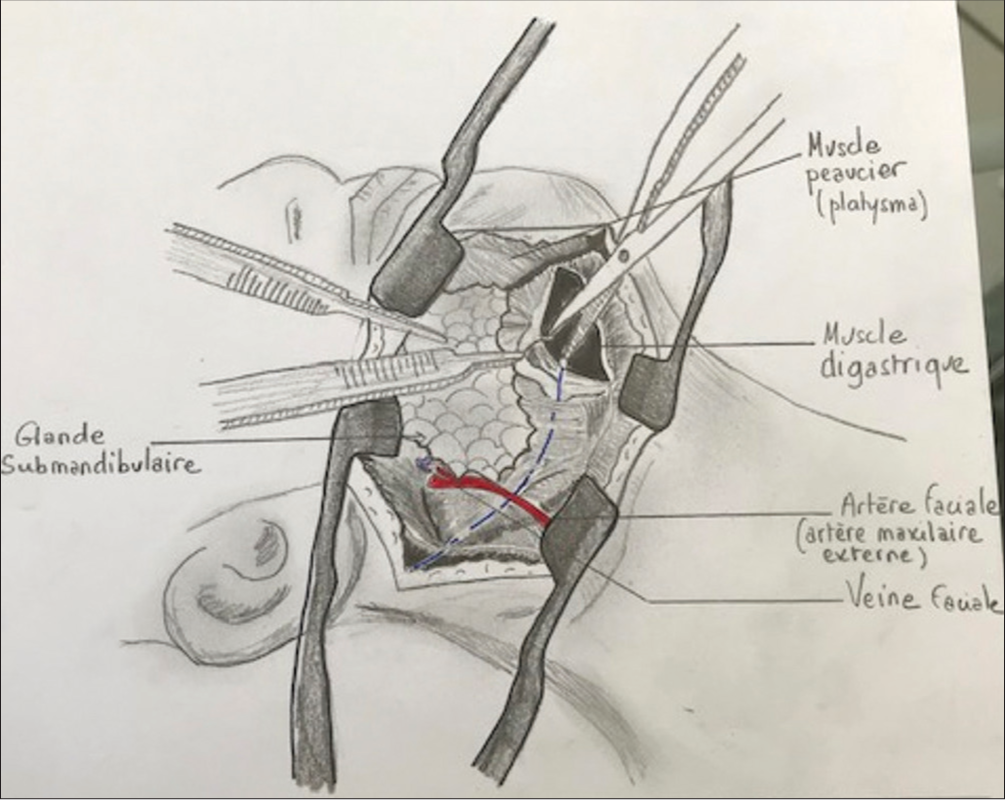
The anterior approach to a C2-C3 cervical disc herniation is difficult due to the complex regional anatomy; the presence of mandible, cranial nerves, critical veins, and arteries.[
CONCLUSION
Our modified anterior retropharyngeal approach for C2-C3 disc herniation is better tailored to the complex regional anatomy and would likely lower complication rates associated with anterior C2-C3 disc resections.
Declaration of patient consent
Patients’ consent not required as patients’ identities were not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
Acknowledgment
We would like to thank Mrs. Estelle CARRE for these magnificent drawings which contribute to the better understanding of our paper.
References
1. Antich PA, Sanjuan AC, Girvent FM, Simó JD. High cervical disc herniation and Brown-Sequard syndrome. A case report and review of the literature. J Bone Joint Surg Br. 1999. 81: 462-3
2. Chau AM, Wong JH, Mobbs RJ. Cervical myelopathy associated with congenital C2/3 canal stenosis and deficiencies of the posterior arch of the atlas and laminae of the axis: Case rport and review of the literature. Spine (Phila Pa 1976). 2009. 34: E886-91
3. Chen TY. The clinical presentation of uppermost cervical disc protrusion. Spine (Phila Pa 1976). 2000. 25: 439-42
4. Kotil K, Sengoz A. The management in the C2-C3 disc herniations: A clinical study. Turk Neurosurg. 2011. 21: 15-21
5. Oka DN, Kouakou F, Haro Y, Sarki SI. Cervical spine disc herniation at C2-C3 level: Study of a clinical observation and literature review. Rom Neurosurg. 2015. 29: 459-64
6. Shim CS, Jung TG, Lee SH. Transcorporeal approach for disc herniation at the C2-C3 level: A technical case report. J Spinal Disord Tech. 2009. 22: 459-62
7. Song Y, Tharin S, Divi V, Prolo LM, Sirjani DB. Anterolateral approach to the upper cervical spine: Case report and operative technique. Head Neck. 2015. 37: E115-9
8. Türe U, Güçlü B, Naderi S. Anterolateral extradural approach for C2-C3 disc herniation: Technical case report. Neurosurg Rev. 2008. 31: 117-21 discussion 121
9. Zhang Y, Zhang J, Wang X, Chen D, Yuan W. Application of the cervical subaxial anterior approach at C2 in select patients. Orthopedics. 2013. 36: e554-60

