

- Emily Rosenorn-Laang Research Officer, Faculty of Health and Social Sciences, Psychiatric Social Work, Bournemouth BH1 3 LT, UK
- Bournemouth University, Bournemouth BH1 3 LT, UK
Correspondence Address:
Colin Pritchard
Bournemouth University, Bournemouth BH1 3 LT, UK
DOI:10.4103/2152-7806.161420
Copyright: © 2015 Pritchard C. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Pritchard C, Rosenorn-Lanng E. Neurological deaths of American adults (55–74) and the over 75's by sex compared with 20 Western countries 1989–2010: Cause for concern. Surg Neurol Int 23-Jul-2015;6:123
How to cite this URL: Pritchard C, Rosenorn-Lanng E. Neurological deaths of American adults (55–74) and the over 75's by sex compared with 20 Western countries 1989–2010: Cause for concern. Surg Neurol Int 23-Jul-2015;6:123. Available from: http://surgicalneurologyint.com/surgicalint_articles/neurological-deaths-of-american-adults-55-74-and-the-over-75s-by-sex-compared-with-20-western-countries-1989-2010-cause-for-concern/
Abstract
Background:Have USA total neurological deaths (TNDs) of adults (55-74) and the over 75's risen more than in twenty Western Countries?
Methods:World Health Organization TND data are compared with control mortalities cancer mortality rates (CMRs) and circulatory disease deaths (CDDs) between 1989-1991 and 2008-2010 and odds ratios (ORs) and confidence intervals calculated.
Results:Neurological Deaths - Twenty country (TC) average 55-74 male rates per million (pm) rose 2% to 503 pm, USA increased by 82% to 627 pm. TC average females rose 1% to 390 pm, USA rising 48% to 560 pm. TC average over 75's male and female increased 117% and 143%; USA rising 368% and 663%, significantly more than 16 countries. Cancer mortality - Average 55-74 male and female fell 20% and 12%, USA down 36% and 18%. TC average over 75's male and female fell 13% and 15%, the USA 29% and 2%. Circulatory deaths - TC average 55-74 rates fell 60% and 46% the USA down 54% and 53%. Over 75's average down 46% and 39%, USA falling 40% and 33%. ORs for rose substantially in every country. TC average 75's ORs for CMR: TND male and females were 1:2.83 and 1:3.04 but the USA 1:5.18 and 1:6.50. The ORs for CDD: TND male and females TC average was 1:3.42 and 1:3.62 but the USA 1:6.13 and 1:9.89.
Conclusions:Every country's neurological deaths rose relative to the controls, especially in the USA, which is a cause for concern and suggests possible environmental influences.
Keywords: Age, gender, international comparison, neurological deaths
INTRODUCTION
Neurological disease has increased in recent years throughout the developed world.[
Earlier research found that dementia morbidity was occurring earlier and had disproportionately increased in some Western countries in people aged 45–74 years, with relatively larger increases in women[
However, as neurological diseases are classically “diseases of the elderly,” it has been argued that the Gompertzian theory on longevity was operating, namely people are now living longer to develop diseases that they would not have lived long enough to have acquired in previous times.[
Conversely, changes or improvements in diagnosis have been thought to be a possible factor,[
Previous work that highlighted earlier dementia deaths,[
However, to try to account for the Gompertzian effect, other “diseases of the elderly,” cancer mortality rates (CMRs) and circulatory disease deaths (CDDs),[
Theoretically therefore, if the two biggest classical diseases of old age, are mainly due to longevity and not changes in lifestyle, treatment advances and the environment, it would be expected that there would be little difference in the patterns of neurological, cancer, and circulatory deaths over the period under review.
The latest available WHO data (July 2014) for the USA is data up to 2010,[
There are two working null hypothesis, that between baseline 1989–1991 and index 2008–10 years there would be no significant differences between:
TND and cancer and circulatory diseases death rates by age or sex in each country, and Between the USA and the other 20 Western in regard to TNDs.
METHODS
World Health Organization standardized mortality data[
One important change in the current WHO reporting is that the previously separate age groups of 55–64 and 65–74 have now been combined into the 55–74 age band[
Cancer mortality rate and CDD rates by age bands and gender are contrasted against TND over the period first to compare each country against itself and then with the USA, twenty country (TC) average being calculated for of each of the age bands and mortalities.
However, when using multi-national data it has to be acknowledged that there are inherent problems in terms of reporting, possible “fashions” in diagnosis and the problem of concomitant diagnoses across different disease conditions. Moreover, when comparing three broad diagnostic categories such as these, raises the issue of different countries having varied health policy strategies, which to a degree might influence treatment priorities and therefore changes of mortality rates over time. In part, this is controlled for by measuring each country against itself which provide a degree of reliability of each country's results over the period. The WHO acknowledges that some countries, but not usually the 21 countries review here, can have problems of reporting, while lead times are usually 4 or more years behind the year of publication, example, WHO report up to 2010 published in July 2014. Furthermore, it is stressed that “it is the underlying cause of death in accordance with the rules of the ICDs that is, reported and data are included only for countries reporting data properly code” (sited in WHO mortality database documentation document), which seems as accurate as is feasible, not least because of the uniformity of collation.[
Statistical analysis
The three mortalities are presented for each age band by sex, and a ratio of change is calculated for any changes over the period. Odds ratios (ORs) are calculated to explore whether TNDs and CMR and CDD have changed proportionally over the 21 years.
A TC average death rate is calculated to be compared with changes in the USA mortality rates over the period.
Confidence intervals (CIs) to ± 95% level of significance are used to determine any statistical significant difference between the USA and each of the other TCs.
RESULTS
Total neurological deaths 55–74
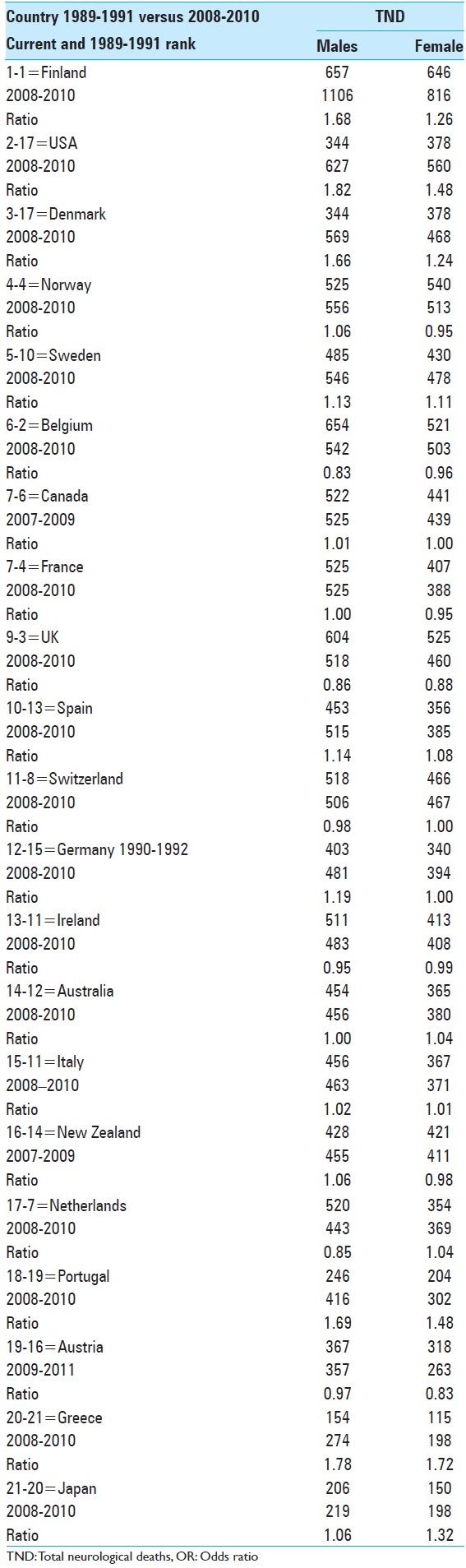
The highest current male 55–74 TND rates ranged from Finland at 1106 pm, down to Japan 219 pm. In 1989–1991, the TC average rate was 495 pm, increasing to 503 pm over the period, equivalent to a 2% rise.
Initially, the USA rate was 344 pm, and was 17th highest out of 21 countries but is now second highest at 627 pm, and had the biggest increase of all countries at 82%.
Females aged 55–74 current TND rates ranged from Finland 816 pm to Greece and Japan 198 pm. The TC average 1989–1991 was 387 pm rising to 390 pm, up 1% whereas the USA rate went from 378 pm to 560 pm, an increase of 48% over the period, which was third largest rise, only Greece had a bigger increase but from a much lower baseline [
Total neurological death over 75's
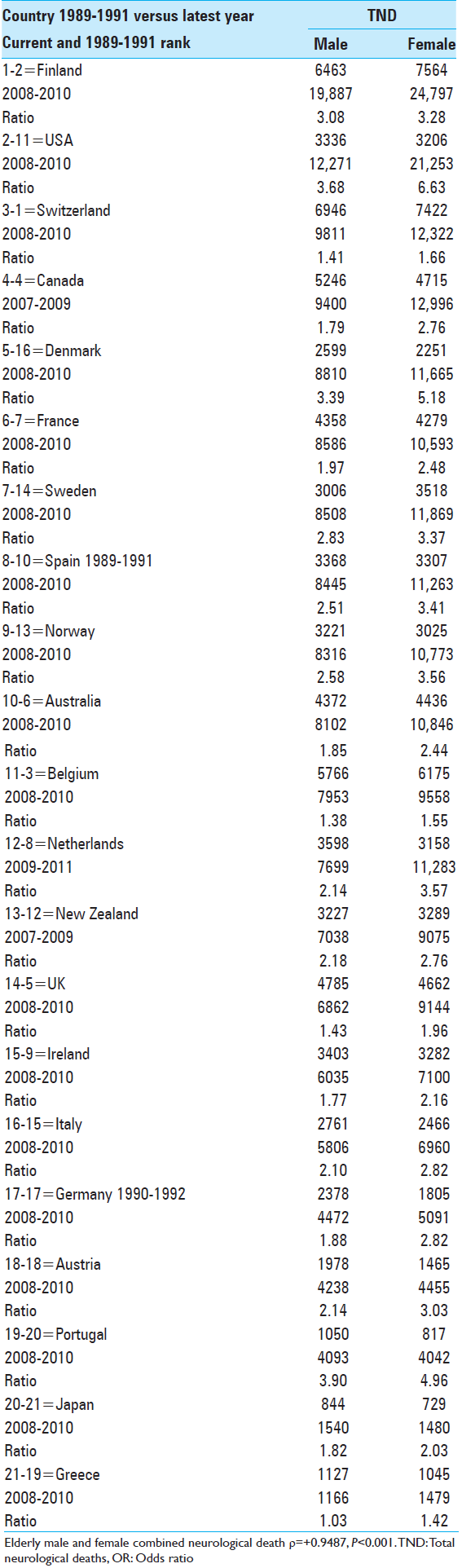
Current male over 75's TND rates were highest in Finland 19,887 pm to the lowest in Greece 1166 pm, with the TC average rising by 114% with rates more than doubling in 11 countries.
The USA rate increased from 3336 pm to 12,271 pm, more than a two-fold (368%) rise over the period and had the biggest increase than all countries.
Current female
The over 75's TND rates ranged from Finland 24,797 pm to lowest in Greece at 1479 pm, with the TC average increasing by 185%, with a doubling of rates in 17 countries. It should be noted that in every country female rates rose more than males over the period.
The USA rate rose from 3206 pm to 21,253 pm, a more than five-fold (663%) increase, which was the largest rise of all countries under review [
Control mortalities
Cancer mortality rates 55–74
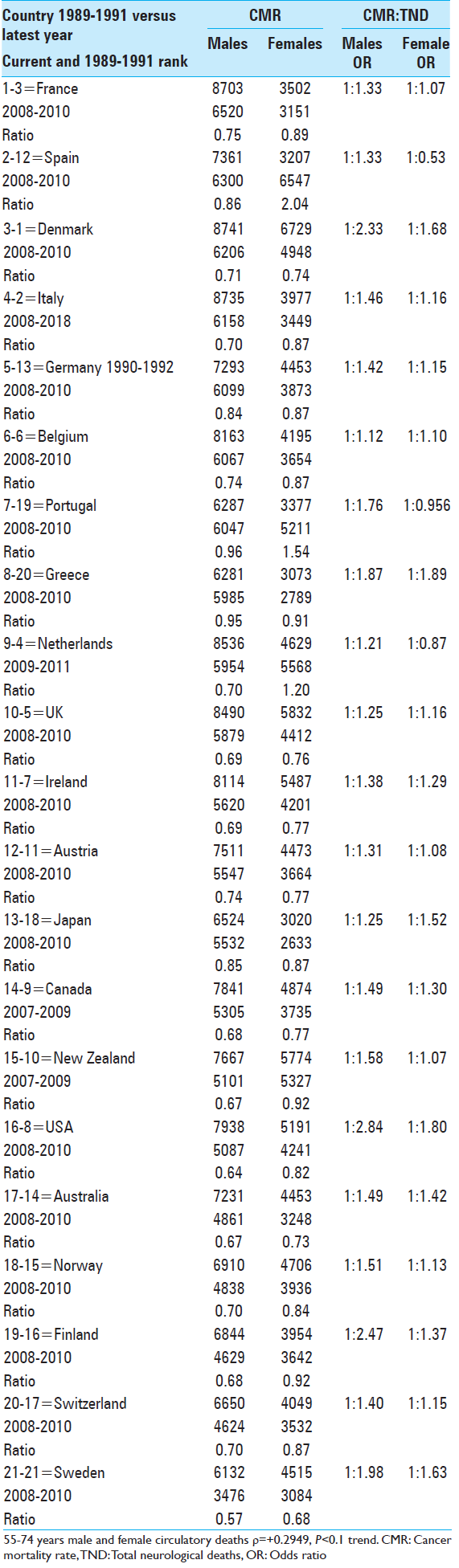
Male CMR fell in every country, the TC average fell from 7501 pm to 6008 pm, a 20% decrease. USA rates went from 7938 pm to 5080 pm, a 36% reduction.
The final column in
USA male 55–74 TND to cancer deaths ratio in 1989–1991 was one to 27.08 cancer deaths by 2008–2010 this had narrowed to 1:8.1.
Female 55–74 average
Apart from the Netherlands, Portugal, and Spain female CMR fell in 18 countries, as the TC average went from 4414 pm to 3703 pm, decrease of 16%. The USA rates fell from 5191 pm to 4241 pm, an 18% reduction.
USA female TND to cancer deaths ratio in 1989–1991 was 1:13.73 by 2008–2010 this had reduced to 1:7.6.
Cancer mortality rate people over 75's+
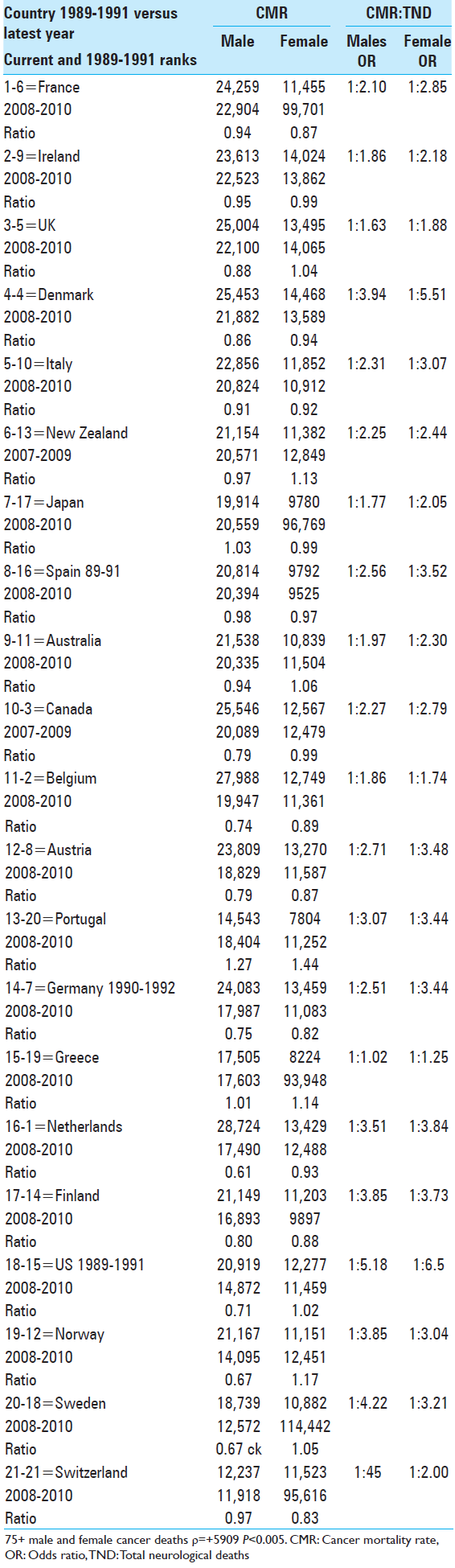
The TC male over 75's CMR moved from 22,666 pm to 19,831 pm, a reduction of 13%. The US rates fell from 20,919 pm to 14,872 pm a fall of 29%.
USA male TND to CMR ratios initially were 1:6.3 by the index years they had narrowed to 1:1.2.
Female over 75's CMR for the TC average fell from 13,038 pm down to 10,989 pm, a 16% reduction. USA over 75's female went from 11,277 pm to 11,040 pm, a 2% decline.
USA TND to CMR ratios in 1989–1991 had been 1:3.53 but by the 2008–2010 this had been reversed so that for every female over 75 cancer death there were 1.85 neurological deaths [
Changes over the period odds ratios cancer mortality rate to total neurological death
Neurological to cancer deaths
In
55–74-year-old
Male 55–74 CMR: TND ratios of >1:1.20 occurred in 20 countries, with a TC average OR of 1:1.53 over the period.
The USA CMR: TND OR was 2.84 and had the widest OR of all countries.
Female 55–74 CMR: TND ORs of >1:1.20 occurred in 9 countries, the TC average OR was 1:1.25.
The USA female OR was 1:1.80 and was the highest of all the countries.
Over 75's
Male CMR: TND ORs for over 75's was >1:2.00 in 14 countries, with a TC average of 1:2.83.
The USA CMR: TND ratio was 1:5.18 and was highest of all countries under review.
Over 75's female ORs more than doubled in 17 countries, the TC average being 1:3.04.
The USA cancer to neurological death for the over 75's female OR was 1:6.50 and was the largest of all countries.
Circulatory disease deaths 55–74
Male 55–74 CDD TC average of 10,103 pm fell to 3936 pm a 61% reduction, the USA fell from 10,165 pm to 4685 pm a 54% reduction.
In the baseline years, USA TND to CDD was one to 29 (1:29.6) by 2008–10 they had narrowed to <1 in 8 (1:7.5).
Female 55–74 CDD TC average rates fell from 4343 pm to 2361 pm, a decline of 46%. American female rates fell from 5191 pm to 2461 pm a 53% reduction.
In the baseline years, female USA TND to CDD had been 1:13.73 at the end of the period they were 1:4.39 [
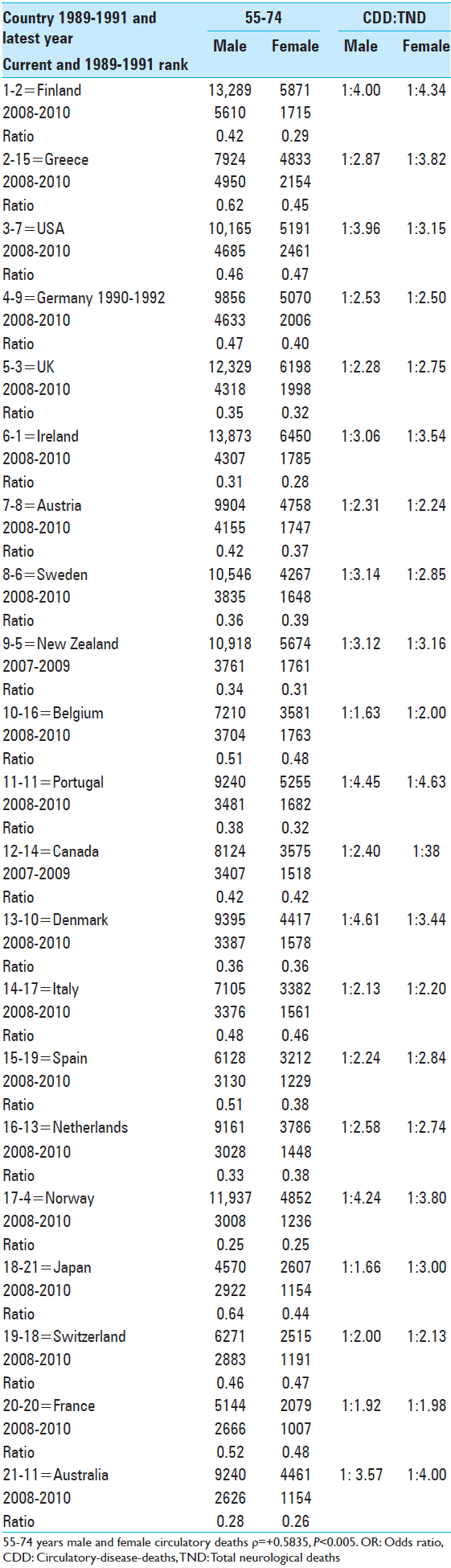
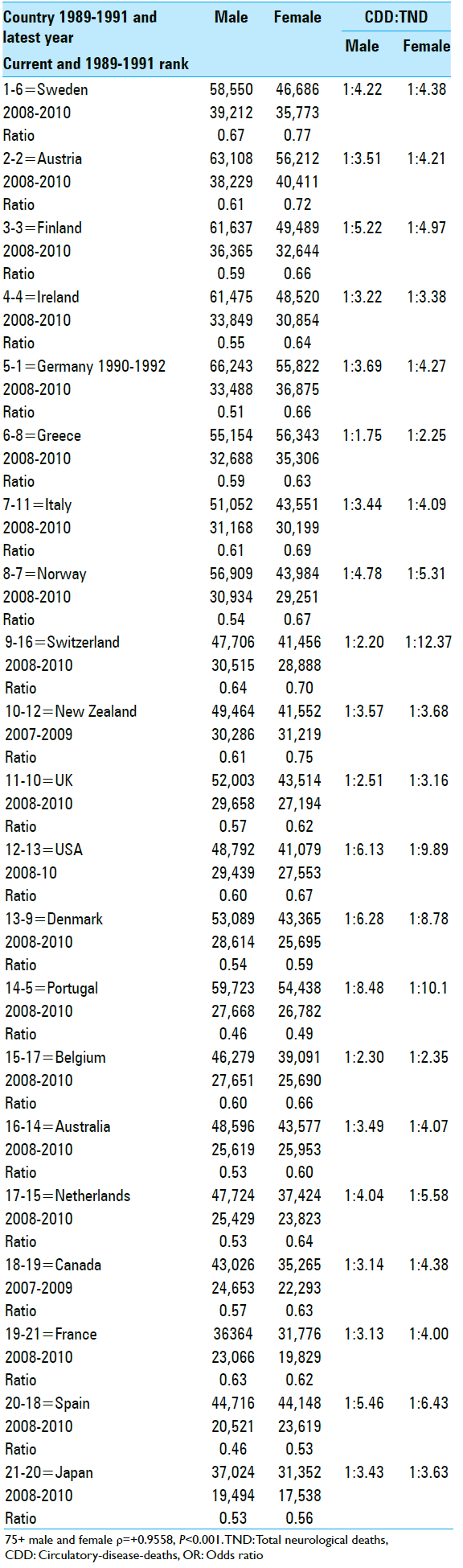
Circulatory disease death the over 75's
Male over 75's TC average CDD rates went from 49,784 pm to 29,429 pm a fall of 41% and rates fell by than 25% in every country. The USA male CDD rate fell from 48,792 pm to 29,439 pm a 40% reduction.
In 1989–1991 USA 75's TND to CCD had been 1:14.63 and now is 1:2.40.
Female over 75's rates also fell substantially (>22%) in every country, the TC average was 44,378 pm and fell to became 28,505 pm a decline of 361%, with USA rates falling from 41,079 pm to 27,553 pm, a 33% reduction.
In 1989–1991 female USA over 75's TND to CDD ratio was 1:12.85 by 2008–2010 it is 1:1.65 [
Neurological to circulatory deaths odds ratios of total neurological death: Circulatory disease death [Tables 5 and 6 ]
Odds ratios 55–74
Male 55–74 TND: CDD ORs have more than doubled in 18 countries, an average of 1:2.83. The USA was 1:3.96, which was fifth largest of 21 countries.
Female 55–74 TND to CDD ORs more than doubled in 19 countries with an average OR of 1:2.74, while USA female was 1:3.15 and was the ninth largest.
Odds ratios over 75's
In regard to the over 75's TND to CDD ORs males more than doubled in 20 countries, with an average of 1:3.84.
The USA OR was 1:6.13 and was third highest of all countries.
Female over 75's OR doubled in every countries, overall ORs were 1:5.05.
The USA OR at 1:9.89 was the third biggest of all countries.
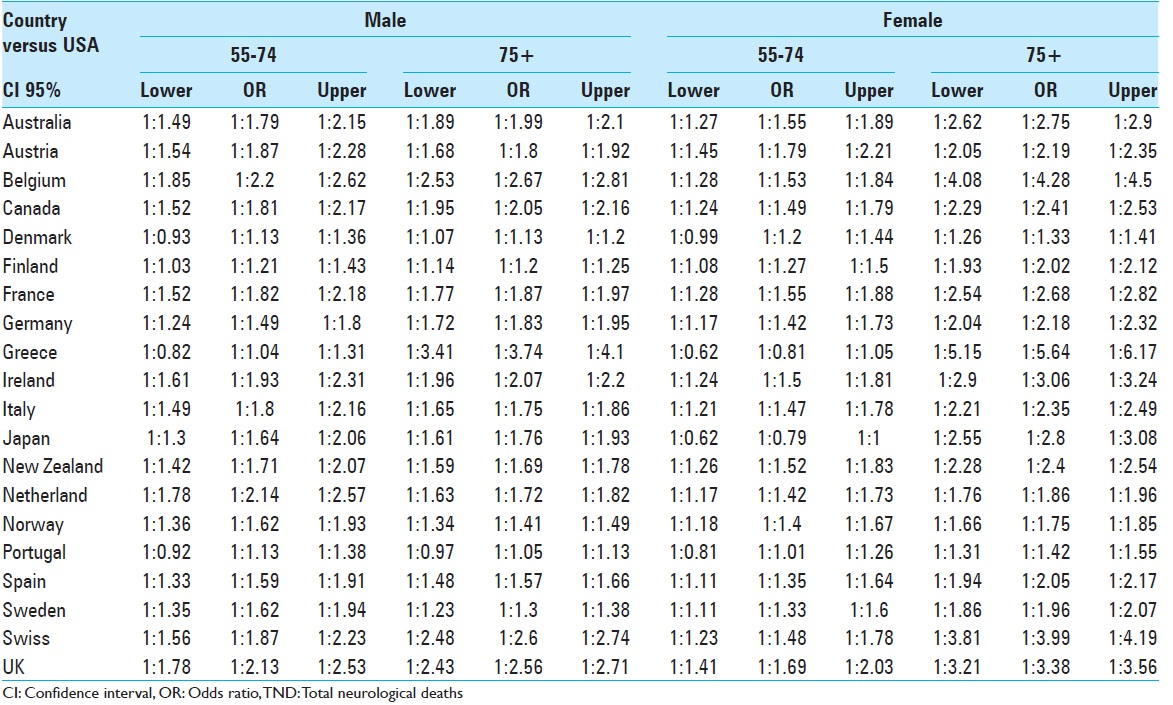
Comparison of USA total neurological death rates versus other countries
DISCUSSION
Main findings
The first null hypothesis, that there would be no significant differences between neurological and the control mortalities over the period can be rejected for both sexes and age bands. The control mortalities fell in every country, whereas the TND, for male and female over 75's rates rose considerably and more than doubled in 13 and 17 countries, respectively.
The second null hypothesis that the USA would not be significantly different from the other countries can also be largely rejected, as USA 55–74 male neurological rates had been equal 17th highest but had risen to being second highest, while USA females went from 10th to being highest out of 21 countries. Moreover, apart from Portugal, over the 20 years the USA had statistically significant greater rises in TND than 16 other countries, indicating disproportionate changes in neurological morbidity and mortality in American adults (55–74) and the over 75's.
Limitations
A core limitation in any study of international mortality rates is the reliability in the reporting of the causes of death and diagnoses where there may be changes in fashion or recording methods. For example, WHO mortality data was previously reported in separate age bands 55–64 and 65–74 but since 2008 they have been combined into 55–74, which made it impossible to directly compare the earlier rates for 55–64-year-olds, which had risen significantly in some countries.[ The differential changes over the period of the three mortalities will likely have been influenced by local health priorities for treatment and the differentials between the neurological deaths and the other mortalities. This would have also been affected by the advances in health policy and treatment of cancer and the circulatory disease and perhaps by a higher priority given to these conditions compared to the neurological. Country specific research would be needed to determine such influences Research on MND, which is part of TND, has yielded some inconsistencies for while some studies found little change in MND rates, and some attributed to the rises to improved categorization,[ The disproportionate rises in TND compared to CMR and CDD might be attributed to more effective treatment of these conditions, as there have been national campaigns to reduce these diseases in many countries, so the possible main reason for the divergence has been more effective treatments? However, would this account for the doubling of TND in most countries in such a relatively short-time, and for the remarkable rises in the USA? Possible interactive factors that have contributed to the increases in TND may be related to the emerging increase in “early-onset dementia,” that could be related to lifestyle changes, rather than wider environmental factors, such as greater alcohol dependence and possible drug-related neurological disturbances[ Neurological diseases are considered to be “diseases of the elderly”[
Overall, therefore, despite the above limits, the neurological changes found when contrasted against cancer and CDDs, all of whom shared the multiple environmental changes, are suggestive that multiple interactive factors are affecting human neurology.
There is much this study cannot explain, seen in three brief examples; the marked differences between countries over time; women's older rate increasing more than males and what accounts for the remarkable two and five-fold increases in older American neurological deaths, which should stimulate a range of hypotheses, which again will require country-specific research. Nonetheless, despite the relatively short period of 20 years, paradoxically, with the relative decline of CMR and CDD deaths, especially in the older group, what if anything has opened the way for any possible latent neurological pathology to develop, we just do not know but is an area for future research.
CONCLUSIONS
The Gompertzian explanation appears limited, not least because it does not explain the USA position, but we avoid the temptation to speculate but point toward a number of studies indicating possible epigenetic factors influencing neurological morbidity,[
The nature of any environmental factors are uncertain but there have been major environmental changes; including increased population, economic activity, substantial rises in road and air travel; increased home technology involving background electromagnetic fields (mobile phones, microwave ovens, computers), which are unique to these later years and these possible environmental factors cannot be ignored, especially as they probably interact.[
IMPLICATIONS
The recognition that increased longevity caries new problems is well accepted, however, the extent of the disproportionate increase in neurological morbidity in comparison with other diseases of the elderly, puts further pressure on already stretched health and social care services but may not yet be fully recognized in regard to neurology. The substantial earlier onset of neurological disorders will have profound psychosocial and economic implications for patients, families, and front-line services that must add to the burden of disease within society, with inevitable psycho-socioeconomic impact upon all involved.[
Crucially therefore, relative to other specialties, the present configuration of services may require re-organization, especially for specialist neurological services and for community psychosocial provision, to meet the challenge. While increases in Alzheimer disease is recognized in many Western countries, there have also been rises in other neurological diseases,[
References
1. Alonso A, Logroscino G, Jick SS, Hernán MA. Incidence and lifetime risk of motor neuron disease in the United Kingdom: A population-based study. Eur J Neurol. 2009. 16: 745-51
2. Alonso V, Villaverde-Hueso A, Hens MJ, Morales-Piga A, Abaitua I, de la Paz MP.editors. Increase in motor neuron disease mortality in Spain: Temporal and geographical analysis (1990-2005). Amyotroph Lateral Scler. 2011. 12: 192-8
3. . Alzheimer's Association. Alzheimer's disease facts and figures. Alzheimers Dement. 2013. 9: 208-45
4. Bergen DC, Silberberg D. Nervous system disorders: A global epidemic. Arch Neurol. 2002. 59: 1194-6
5. Callaghan B, Feldman D, Gruis K, Feldman E. The association of exposure to lead, mercury, and selenium and the development of amyotrophic lateral sclerosis and the epigenetic implications. Neurodegener Dis. 2011. 8: 1-8
6. Chang PA, Wu YJ. Motor neuron diseases and neurotoxic substances: A possible link?. Chem Biol Interact. 2009. 180: 127-30
7. Chio A, Magnani C, Schiffer D. Gompertzian analysis of ALS mortality in Italy 1957-1987: Application to birth cohorts. Neuroepidemiology. 1995. 14: 269-77
8. Cima V, Logroscino G, D’Ascenzo C, Palmieri A, Volpe M, Briani C. Epidemiology of ALS in Padova district, Italy, from 1992 to 2005. Eur J Neurol. 2009. 16: 920-4
9. Last accessed on 2014 Jun 06. Available from: http://www.cjd.ac.uk/figures.htm .
10. Costa LG, Giordano G, Faustman EM. Domoic acid as a developmental neurotoxin. Neurotoxicology. 2010. 31: 409-23
11. D’Alton S, Hunter S, Whitehouse P, Brayne C, George D. Adapting to dementia in society: A challenge for our lifetimes and a charge for public health. J Alzheimers Dis. 2014. 42: 1151-63
12. Day TG, Scott M, Perring R, Doyle P. Motor neuron disease mortality in Great Britain continues to rise: Examination of mortality rates 1975 - 2004. Amyotroph Lateral Scler. 2007. 8: 337-42
13. Diekstra FP, Beleza-Meircles A, Leigh NP, Shaw CE, Al-Chalabi A. Interaction between PONI and population density in amyotrophic lateral sclerosis. Neuroreport. 2009. 20: 186-90
14. Easton DM. Gompertzian growth and decay: A powerful descriptive tool for neuroscience. Physiol Behav. 2005. 86: 407-14
15. Ferri CP, Prince M, Brayne C, Brodaty H, Fratiglioni L, Ganguli M. Global prevalence of dementia: A Delphi consensus study. Lancet. 2005. 366: 2112-7
16. Flint-Richter P, Sadetzki S. Genetic predisposition for the development of radiation-associated meningioma: An epidemiological study. Lancet Oncol. 2007. 8: 403-10
17. Forbes RB, Colville S, Parratt J, Swingler RJ. The incidence of motor nueron disease in Scotland. J Neurol. 2007. 254: 866-9
18. Goldacre MJ, Duncan M, Griffith M, Turner MR. Trends in death certification for multiple sclerosis, motor neuron disease, Parkinson's disease and epilepsy in English populations 1979-2006. J Neurol. 2010. 257: 706-15
19. Gordon PH, Artaud F, Aouba A, Laurent F, Meininger V, Elbaz A. Changing mortality for motor neuron disease in France (1968-2007): An age-period-cohort analysis. Eur J Epidemiol. 2011. 26: 729-37
20. Graham AJ, Macdonald AM, Hawkes CH. British motor neuron disease twin study. J Neurol Neurosurg Psychiatry. 1997. 62: 562-9
21. Hebert LE, Weuve J, Scherr PA, Evans DA. Alzheimer disease in the United States (2010-2050) estimated using the 2010 census. Neurology. 2013. 80: 1778-83
22. Horton R. GBD 2010: Understanding disease, injury, and risk. Lancet. 2012. 380: 2053-4
23. Hugo J, Ganguli M. Dementia and cognitive impairment: Epidemiology, diagnosis, and treatment. Clin Geriatr Med. 2014. 30: 421-42
24. Imaizumi Y. Longitudinal gompertzian analysis of mortality from prostate cancer in Japan, 1955-1996. Cancer Detect Prev. 2000. 24: 473-84
25. Imaizumi Y. Longitudinal Gompertzian analysis of Parkinson's disease mortality in Japan, 1950-1993. Mech Ageing Dev. 1995. 85: 15-23
26. James BD, Leurgans SE, Hebert LE, Scherr PA, Yaffe K, Bennett DA. Contribution of Alzheimer disease to mortality in the United States. Neurology. 2014. 82: 1045-50
27. Johansen C. Electromagnetic fields and health effects – Epidemiologic studies of cancer, diseases of the central nervous system and arrhythmia-related heart disease. Scand J Work Environ Health. 2004. 30: 1-30
28. Kasai M, Nakamura K, Meguro K. Alzheimer's disease in Japan and other countries: Review of epidemiological studies in the last 10 years. Brain Nerve. 2010. 62: 667-78
29. Kelley BJ, Boeve BF, Josephs KA. Young-onset dementia: Demographic and etiologic characteristics of 235 patients. Arch Neurol. 2008. 65: 1502-8
30. Ladogana A, Puopolo M, Croes EA, Budka H, Jarius C, Collins S. Mortality from Creutzfeldt-Jakob disease and related disorders in Europe, Australia, and Canada. Neurology. 2005. 64: 1586-91
31. Llibre Rodriguez JJ, Ferri CP, Acosta D, Guerra M, Huang Y, Jacob KS. Prevalence of dementia in Latin America, India, and China: A population-based cross-sectional survey. Lancet. 2008. 372: 464-74
32. Lunke S, El-Osta A. The emerging role of epigenetic modifications and chromatin remodeling in spinal muscular atrophy. J Neurochem. 2009. 109: 1557-69
33. Maiovis P, Ioannidis P, Konstantinopoulus E, Karacostas D. Early onset dementias: Demographic characteristics and etiological classification in a tertiary referral centre. Acta Neurol Belg. 2014. 115: 27-31
34. Mercy L, Hodges JR, Dawson K, Barker RA, Brayne C. Incidence of early-onset dementias in Cambridgeshire, United Kingdom. Neurology. 2008. 71: 1496-9
35. Murphy M, Quinn S, Young J, Parkin P, Taylor B. Increasing incidence of ALS in Canterbury, New Zealand: A 22-year study. Neurology. 2008. 71: 1889-95
36. Panegyres PK, Chen HY. Coalition against Major Diseases (CAMD). Early-onset Alzheimer's disease: A global cross-sectional analysis. Eur J Neurol. 2014. 21: 1149-54
37. Prince MJ, Wu F, Guo Y, Gutierrez Robledo LM, O’Donnell M, Sullivan R. The burden of disease in older people and implications for health policy and practice. Lancet. 2015. 385: 549-62
38. Pritchard C, Baldwin D, Mayers A. Changing patterns of adult (45-74 years) neurological deaths in the major Western world countries 1979-1997. Public Health. 2004. 118: 268-83
39. Pritchard C, Evans B. Population density and cancer mortality by gender and age in England and Wales and the Western World 1963-93. Public Health. 1997. 111: 215-20
40. Pritchard C, Hickish T. Comparing cancer mortality and GDP health expenditure in England and Wales with other major developed countries from 1979 to 2006. Br J Cancer. 2011. 105: 1788-94
41. Pritchard C, Mayers A, Baldwin D. Changing patterns of neurological mortality in the 10 major developed countries – 1979-2010. Public Health. 2013. 127: 357-68
42. Retsky MW, Swartzendruber DE, Bame PD, Wardwell RH. Computer model challenges breast cancer treatment strategy. Cancer Invest. 1994. 12: 559-67
43. Riggs JE, Schochet SS Jr. Rising mortality due to Parkinson's disease and amyotrophic lateral sclerosis: A manifestation of the competitive nature of human mortality. J Clin Epidemiol. 1992. 45: 1007-12
44. Rizzi L, Rosset I, Roriz-Cruz M. Global epidemiology of dementia: Alzheimer's and vascular types. Biomed Res Int 2014. 2014. p.
45. Rose MR, Rauser CL, Mueller LD, Benford G. A revolution for aging research. Biogerontology. 2006. 7: 269-77
46. Schaller S, Mauskopf J, Kriza C, Wahister P, Kolominisky-Rabas P. Pay me now or pay me later: Dementia and the cost of health care. Int J Geriatr Psychiatry. 2015. 30: 111-29
47. Scott KM, Abhinav K, Wijesekera L, Ganesalingam J, Goldstein LH, Janssen A. The association between ALS and population density: A population based study. Amyotroph Lateral Scler. 2010. 11: 435-8
48. Woodburn KJ, Johnstone EC. Early-onset dementia in Lothian, Scotland: An analysis of clinical features and patterns of decline. Health Bull (Edinb). 1999. 57: 384-92
49. .editors. World Health Organization. International Classification of Diseases. Geneva: World Health Organization; 1992. p.
50. . Available from: http://www.whoint/whosis/mort/table1.process.cfm .


Miguel A. Faria, M.D.
Posted July 28, 2015, 3:32 pm
The findings of this study — namely that tremendous increases in Total Neurological Deaths (TND) over a 20-year period in twenty countries, particularly the United States — are quite disturbing. This new medical challenge is worrisome even in the face of the remarkable decline in cancer mortality rates (CMR) and circulatory disease deaths (CDS) for males and females in both age groups, 55-74 and 75 and over.
It is ironic that the reduced mortality rates in CMR and CDD, particularly in the over age 75 group, cannot be celebrated, but instead has to be compared to increased TND mortality rates that threaten to cancel out the improvement in longevity achieved from better health in almost all other diseases. TND threaten to curtail life expectancy in the future, particularly in the United States.
Consider the fact that in the U.S. for males and females (Ages 55-74) CMR fell 36% and 18% respectively; and CDD, 40% and 33%. Yet, TND for males and females (ages 75 and over) increased 368% and 663% respectively.
The Gompertzian effect that suggests we are getting more degenerative diseases because we are living longer, I believe, still plays a role, albeit not as significantly as we would expect. That more effective treatment for cancer and vascular diseases may play a role in these statistics again seems not to play a significant role as to the increase in TND. What this study suggests is that the two most likely possibilities for the increase in TND may be related to unknown environmental factors, or even more likely, epigenetics phenomena, as yet to be discovered. The U.S may lead the way in this trend, the authors of this study suggest, because America leads in lifestyle choices and the popular cultural — “the epitome of modern living.” If this is truly the case here, then it is a troubling and not a salutary trend for health and longevity.
On a better note, we must keep in mind, longevity continues to increase (although at a slightly slower pace) and the compression of morbidity hypothesis seems to be holding.(1) According to the National Vital Statistics Report, the life expectancy of an American in 1990 was 75. Today a newborn has an expected longevity of 79 years.(2)
Nevertheless, the findings of this study are indeed troubling and need further corroboration. Other studies need to be carried out to verify these statistics and ascertain in individual countries what environmental and epigenetic factors may be at play in escalating deaths as far as TND, and the United States will again have to lead the way in these investigations. The authors, Drs Colin Pritchard and Emily Rosenom-Lanng have done an outstanding epidemiological investigation and have my congratulations for bringing to our attention this disturbing phenomenon and presenting these observations in a convincing and elegant manner, and in a succinct scientific methodology.
Miguel A. Faria, M.D.
References
1. Faria MA. Longevity and compression of morbidity from a neuroscience perspective: Do we have a duty to die by a certain age?. Surg Neurol Int 30-Mar-2015;6:49. Available from: http://surgicalneurologyint.com/surgicalint_articles/longevity-and-compression-of-morbidity-from-a-neuroscience-perspective-do-we-have-a-duty-to-die-by-a-certain-age/
2. National Vital Statistics Report. Centers for Disease Control and Prevention. United States Life Tables, 2009. January 6, 2014; 62(7):1-63. Available from: http://www.cdc.gov/nchs/products/nvsr.htm#vol63
Dr S Prokop
Posted August 8, 2015, 3:05 pm
Where is the work of Professor Calderon-Garciduenas ?
Please see my evidence to the EAC of UK Parliament:
http://data.parliament.uk/writtenevidence/committeeevidence.svc/evidencedocument/Environmental%20Audit/Action%20on%20air%20quality/written/9765.html
Priyanka Bandara PhD
Posted August 8, 2015, 11:16 pm
Intriguing data that must be taken into urgent consideration by public health authorities to reduced environmental causes of chronic diseases that are poorly regulated at present. Of particular concern is the regulation of man-made non-ionizing radiation – both low and high frequency electromagnetic fields (EMF). High frequency EMFs in the radio-frequency part of the spectrum (mostly microwaves used for mobile, wireless, satellite communications as well as microwave cooking) have increased in human environments by over a billion fold over the last few decades. A constant RF emitter such as a cordless DECT phone or a baby monitor – a single device – can increase one’s immediate exposure by many thousand fold even today, in the current sea of RF-EMFs (electrosmog). Mobile phone use has skyrocketed over the last couple of decades and RF-EMF exposure is much more with newer smart phones and tablet computers with WiFi connectivity. Despite growing evidence of a wide range of biological effects that are induced upon exposure to low levels of EMFs, they have not been taken into account in public exposure standard setting. Most commonly used ICNIRP or IEEE guidelines in standard setting are based on thermal effects (tissue heating) of acute exposures and therefore cannot provide protection against non-thermal effects or effects induced by chronic exposures. It is time to pay urgent attention to biochemical and physiological changes induced by RF bioeffects such as disruption of ion channels, increased oxidative stress, structural and functional changes to cell components like membranes and proteins. These biochemical and physiological changes potentially affect different systems, notably the nervous, immune and endocrine functions.
RF has been demonstrated in some in vivo studies to act alone as a carcinogen as well as to increase carcinogenicity of known chemical carcinogens. The most likely pathobiological role of RF-EMR in chronic neurological diseases remain understudied, despite epidemiological evidence of increased neurological disturbance found in a dozen studies conducted on people living near RF transmitters like mobile phone base stations, not to mention the increasing incidence of childhood neuro-development disorders in the digital age.
This study provides impetus for better research in this area as well as urgent precautionary warnings to the public to reduce exposure based on the existing scientific evidence of harm.
Miguel A. Faria, M.D.
Posted August 12, 2015, 5:24 pm
As noted above everyone has ideas and alleged suspects supposedly responsible for these disturbing statistics in neurological deaths in the U.S and Western countries. In noting the comments under this article I observe that Dr. S. Prokop and Professor Calderon-Garciduenas suspect air pollution as the culprit, and supporting data is provided to that effect. Dr. Priyanka Bandara attributes the problem to man-made ionization radiation, both low-frequency and high frequency electromagnetic fields, and also cites circumstantial evidence and valuable data. Drs. Anthony Samsel and Stephanie Seneff in a study also published in SNI are blaming and (already are very prematurely) calling for the banning of the herbicide glyphosate! They not only believe their culprit is responsible for degenerative neurological diseases but for every conceivable disease process, from anxiety disorders and autism to environmental catastrophes.
Thus, the variety of suspects alone is supportive evidence that we are no closer to really pinpointing with any scientific certainty the epidemiological, or rather the pathological agent(s), responsible. Perhaps the process is multifactorial. The fact then is that more studies need to be done before any one process is definitely singled out and blamed for the disturbing claim. All of these suspects, and many others not mentioned here, need to be further studied. I think Drs. Colin Pritchard and Emily Rosenorn-Lanng should be congratulated not only for providing an elegant epidemiological study but also be praised for their wise restraint in prematurely blaming any one culprit.
Priyanka Bandara
Posted August 19, 2015, 2:28 am
I appreciate Dr. Faria’s reply and agree with the message that the environmental aspect of chronic neurological disease causation is most likely to be multi factorial. The available scientific literature certainly points to multiple factors acting synergistically to increase the total allostatic load of the exposed human bodies. I was merely drawing attention of the scientific readers to just one of the widespread man-made environmental pollutants in the 21st century – electromagnetic fields, particularly from use of microwaves for modern wireless technologies. Research evidence spanning a few decades clearly raise red flags that the clinical community must take not of.
Russell L Blaylock, M.D.
Posted August 14, 2015, 5:19 pm
This was a very interesting study and the idea that neurological diseases are increasing with a shift to the younger person has been suggested in the recent past. This is the first study to carefully document the problem. As far as the causation, microwave and other EMF exposure is a real culprit and has been discussed quite well by Dr. Faria, but there are other links that may acts synergistically, some of which are quite controversial. One of the strongest links is the Western diet, which is quite high in sugar, high glycemic carbohydrates, trans fats, excitotoxin food additives and oxidized N-6 oils. In combination, these foods and additives can produce severe and prolonged damage to multiple neurological systems. The most controversial link, and one that I have spent many hours studying, is the link to excessive vaccinations and how the vaccines are given. It is known that systemic activation of the immune system, especially if prolonged or repetitive, can activate brain microglia and under special conditions, lead to neurodegeneration. What most research shows is that systemic immune stimulation causes neurdegeneration only if the brain has been lesioned, either by pathological processes, such as scarring or congenital defects, or by brain immune activation. This could involve a great many elderly and even middle age individuals since many have a variety of preexisting brain lesions–such as micro strokes, traumatic astrogliosis, toxic metal accumulations, latent viruses and free radical and lipid peroxidation damage. It has been shown that sequential systemic immune stimulation in the elderly animal model can first prime brain microglia and then with the next vaccine, cause a more intense reaction of the microglia that is neurodestructive for prolonged periods. It is also known that as we age our microglia become primed, making subsequent immune activation infinitely more neurodestructive. With the increased number of vaccines being recommended for adults similar conditions to these experimental studies are being duplicated.
Most of these vaccines contain aluminum adjuvants and studies have shown that this aluminum does indeed move intro the brain with the primary site of accumulation being the microglia and astrocytes. This is not only directly neurotoxic but also is a site of content immune activation within the brain. Unlike natural infections, vaccinations produce prolonged immune activation that can persist for years. The combination of a pro -inflammatory diet and excessive immune stimulation by vaccination would raise risk considerably. The EMF, by damaging the CNS would also produce a condition in which systemic immune stimulation would produce prolonged and intense microglial activation and neurodestruction. The highest concentration of microglia are in the hippocampus, the prefrontal cortex and the substantial nigra, which would explain the link to both Parkinson’s disease and Alzheimer’s disease. Destruction of these brain sites have been produced in animals using injections of immune adjuvants (the same ones in vaccines) both directly in the nuclear areas and then followed with systemic immune stimulation. The science behind this mechanism is quite powerful but because of the vaccine controversy it is being ignored without examination.
References
1. Strunecka A. Cellular and Molecular Biology of Autism Spectrum Disorders. Bentham Science Pub, 2010
2. Strunecka A, Blaylock RL, Patocka J. Aluminofluoride complexes: Phosphate analogues and a hidden hazards for living organisms. Curr Inorg Chem 2012;2:8-18.
3. Blaylock RL. Aluminum induced immunoexictotoxicity in neurodevelopmental and neurodegenerative disorders. Curt Inorg Chem 2012;2: 46-53.
4. Blaylock RL. A possible mechanism in autism spectrum disorders, part 2. Altern There Health Med 2009;15(1):60-7.
5. Blaylock RL, Strunecka A. Immune-glutamatergic dysfunction as a central mechanism in autism spectrum disorders. Curr Med Chem 2009;16(2):157-70.
6. Blaylock RL, Maroon J. Immunoexcitotoxicity as a central mechanism in chronic traumatic encephalopathy–a unifying hypothesis. Surg Neuro Int 2011;2:107.
7. Blaylock RL. Immunology primer for neurosurgeons and neurologists part 2: innate brain immunity. Surg Neurol Int 2013;4:118.
8.Campbell A et al. Chronic exposure to aluminum in drinking water increases inflammatory parameters selectively in the brain. J Neurosci Res 2004;75(4):565-72.
9. Barrientos RM et al. Characterization of the sickness response in young and aging rats following E.Coli infection. Brain behave Immunol 2009;23:450-4.
10. Block ML et al. Microglia-mediated neurotoxicity:uncovering the molecular mechanisms. Nat Rev Neurosci 2007;8:57-69.
11. Dantzer R. Cytokine-induced sickness behavior: Mechanisms and implications. Ann NY Acad Sci 2001;933:222-34.
12. Dilger RN, Johnson RW. Aging microglial cell priming and the discordant central inflammatory response to signals from the peripheral immune system. J Leuko Biol 2008;84:932-9.
13. Dantzer R. et al. From inflammation to sickness behavior and depression: when the immune system subjugates the brain. Nat Rev Neurosci 2008;9:46-57.
P. James Seberger M.D., Ph.D.
Posted August 16, 2015, 3:32 pm
Several years ago there was very good evidence in the US from Cache County, UT, that the relative risk of Alzheimer’s disease in an “unaffected” spouse of Alzheimer’s disease was 6 fold. Thus, we have other, very strong evidence of an environmental cause. We are really barking up the wrong tree if we site genetic only causes.
We also have good evidence at autopsy provided by Judith Miklossy that spirochetal infection of periodontal origin can by found in 90% of Alzheimers’ patients.
So, how do we reconcile these very good evidences of the cause and etiology of Alzheimer’s disease?
A good mechanistic explanation may that environmental pollutants weaken the blood brain barrier, allowing for infection and inflammation to ascend into the brain. This is supported, for example, by IL-17’s effect on the blood brain barrier, in which IL-17 initiates oxidation at the blood brain barrier, ultimately resulting in increased permeability of these tight junctions. This is a single example. Clearly, air pollution is an oxidative load and has been shown to cause the changes listed above.
In fact, there is good evidence that cognitive decline can be reversed. A practical program has been described by Dale Bredesen at UCLA, in which multiple lifestyle, biochemical, and nutritional/functional/herbal supplements proved effective in reversing the early stages of mild cognitive decline. Thus, we can all be correct, and have an actual, realistic way of dealing with the problem.
Priyanka Bandara
Posted August 19, 2015, 8:55 am
Thanks to Dr. Saberger for the insightful reply. Scientific evidence overwhelmingly points to more likely environmental causation (including dietary route) than genetics in this case. However, the genetic aetiology is likely to increase with increasing environmental levels of genotoxic pollutants that are capable of inducing de novo DNA mutations. There are numerous toxic environmental agents with multiple modes of action and as well as the ability to interact with a multitude of other factors that render the elucidation of the pathobiology of any disease extremely difficult.
For example, my example of chronic “low level” microwave exposure from mobile phones and range of wireless devices has been demonstrated to:
• increase the permeability of the blood brain barrier (please refer to the collated scientific evidence by Dr Leif Salford and colleagues on Section 10 of the Bioinitiative Report 2012: http://www.bioinitiative.org/table-of-contents/). This would exposure brain to any circulating chemical toxins.
• increase the risk of developing brain tumours (section 11 of above and more recent work of Dr. Lenart Hardell’s team and the French CERENAT study ) and Morgan L et al., Int J Oncol. 2015 doi: 10.3892/ijo.2015.2908
• increase oxidative stress (recent review found 93 out of 100 studies to report this – Yakymenko et al Electromagn Biol Med. 2015 Jul 7:1-16), and this oxidative damage is likely to be exacerbated by concurrent heavy metal exposure.
• induce genotoxic effects (section 6 of the Bioinitiative report) and Ruediger, HW. Pathophysiology, 2009;16:2–3)
• disruption of membrane ion channels leading to hampered signal transduction pathways (reviews by Dr. Martin Pall: Electromagn Biol Med. 2014 Dec;33(4):251); J Cell Mol Med. 2013 Aug;17(8):958-65)
As for the mentioned 6-fold increased relative risk of Alzheimer’s disease in an “unaffected” spouse in Alzheimer’s disease, this is further evidence that we should investigate all the plausible environmental risk factors of affected individuals- including their cell phone/cordless phone usage as well as their exposure to a whole host of microwave transmitting devices. Intervention studies whereby patients’ exposure to microwaves are carefully monitored (and reduced) while monitoring clinical changes, are likely to give further insights.