

- Department of Neurosurgery, Govind Ballabh Pant Institute of Postgraduate Medical Education and Research, Delhi, India.
- Department of Radiodiagnosis, Govind Ballabh Pant Institute of Postgraduate Medical Education and Research, Delhi, India.
- Department of Pathology, Govind Ballabh Pant Institute of Postgraduate Medical Education and Research, Delhi, India.
Correspondence Address:
Abhishek Katyal, Department of Neurosurgery, Govind Ballabh Pant Institute of Postgraduate Medical Education and Research, Delhi, India.
DOI:10.25259/SNI_168_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Abhishek Katyal1, Anil Jadhav1, Aparna Katyal2, Anita Jagetia1, Shaam Bodeliwala1, Ghanshyam Das Singhal1, Wajid Nazir1, Vineeta Batra3, Arvind Kumar Srivastava1, Daljit Singh1. Occipital transtentorial approach for pineal region lesions: Addressing the controversies in conventional teaching. 06-Oct-2021;12:503
How to cite this URL: Abhishek Katyal1, Anil Jadhav1, Aparna Katyal2, Anita Jagetia1, Shaam Bodeliwala1, Ghanshyam Das Singhal1, Wajid Nazir1, Vineeta Batra3, Arvind Kumar Srivastava1, Daljit Singh1. Occipital transtentorial approach for pineal region lesions: Addressing the controversies in conventional teaching. 06-Oct-2021;12:503. Available from: https://surgicalneurologyint.com/surgicalint-articles/11157/
Date of Submission
15-Feb-2021
Date of Acceptance
07-Sep-2021
Date of Web Publication
06-Oct-2021
Abstract
Background: The occipital transtentorial (OT) approach is well-established approach for pineal region tumors and can be of choice for the lesions located around the suboccipital part of tentorium such as the quadrigeminal plate, posterior part of thalamus, tentorial surface of cerebellum, splenial region, posterior falx, and lesions around the tentorial incisura. However, it is not very much extensively used in the above-mentioned locations other than the pineal region.
Methods: Thirty-one patients of pineal region lesions were operated by OT approach, the role of conventional preoperative evaluation of the anatomy of the venous sinuses, deep venous system, and tentorial angle was investigated.
Results: A variety of lesions were operated using this approach achieving gross and near total resection in majority of the cases (76.6%), with acceptable postoperative mean modified Rankin scales (1.8).
Conclusion: The OT is a preferable approach for pineal region lesions for patients of all ages and can be tailored for achieving high resectability rates irrespective of the status of the deep venous system and tentorial angle, with reasonable postoperative surgical outcome.
Keywords: Deep venous system, Occipital transtentorial, Pineal region, Tentorial angle, Vein of Galen
INTRODUCTION
Pineal region can be described as pineal gland and adjacent area such as tentorial incisura, quadrigeminal plate, and posterior part of thalamus, tentorial surface of cerebellum, splenial region, posterior falx, and torcula.[
This approach is relatively difficult as it deals with three big sinuses, namely, superior sagittal sinus (SSS), transverse sinus (TS), and straight sinus (SS) along with venous channels in the tentorium which may be present in some cases. Besides that, the cutting of the tentorium also has to be mastered. Moreover, if one learns to deal with these issues, it is the approach, which can address many lesions in the pineal region, and would provide wider exposure; main surgeon can get the help of assistant surgeons in vascular cases. However, it can be difficult and disorienting for some surgeons due to lateral/prone positioning, particularly in cases with aberrant and anomalous anatomy of venous sinuses. We are presenting our experience with this approach in pineal region lesions with special emphasis on location of veins in relation to lesion, cutting the tentorium, the tentorial angle, and the surgical outcome.
MATERIALS AND METHODS
All the of cases of pineal region lesions both benign and malignant as diagnosed by computed tomography (CT), magnetic resonance imaging (MRI) contrast, irrespective of age, and location of deep venous system were operated by OT approach. MR or CT Venogram was done to see occipital veins and TS dominance to decide the side of craniotomy, which was performed on the side with lesser number of occipital veins. The tentorial angle (n) [
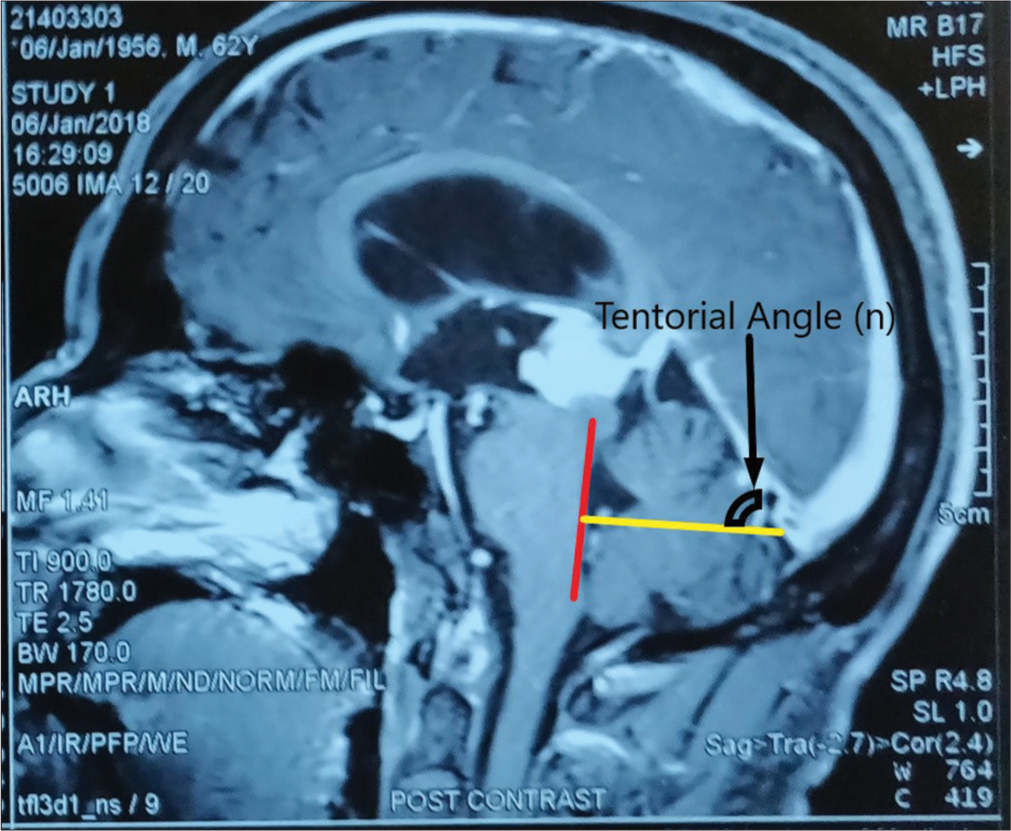
Figure 1:
Measurement of tentorial angle (n). The floor of the fourth ventricle is marked by the line in red, extending inferiorly from just under the inferior colliculus. The new reference line, in yellow, is drawn perpendicular to this red line, extending through the torcula. The tentorial angle is measured against this yellow line.
Preoperative ventriculoperitoneal shunt was carried out in patients who presented with acute features of raised intracranial pressure. Patients were operated in prone or lateral position. In patients where prone position was used, after craniotomy, head was rotated to make the operative side dependent. Skin incision was U-shaped with vertical limb just lateral to midline [
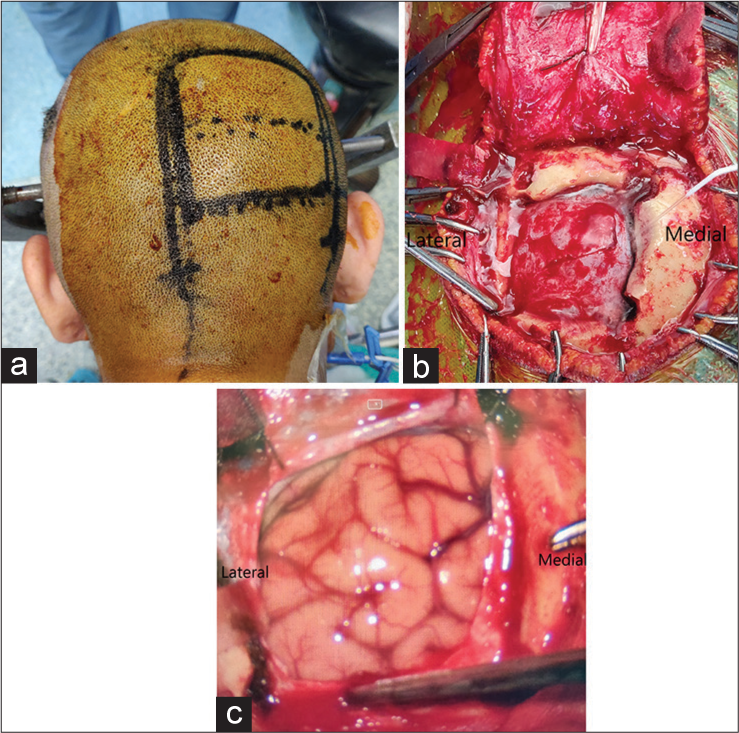
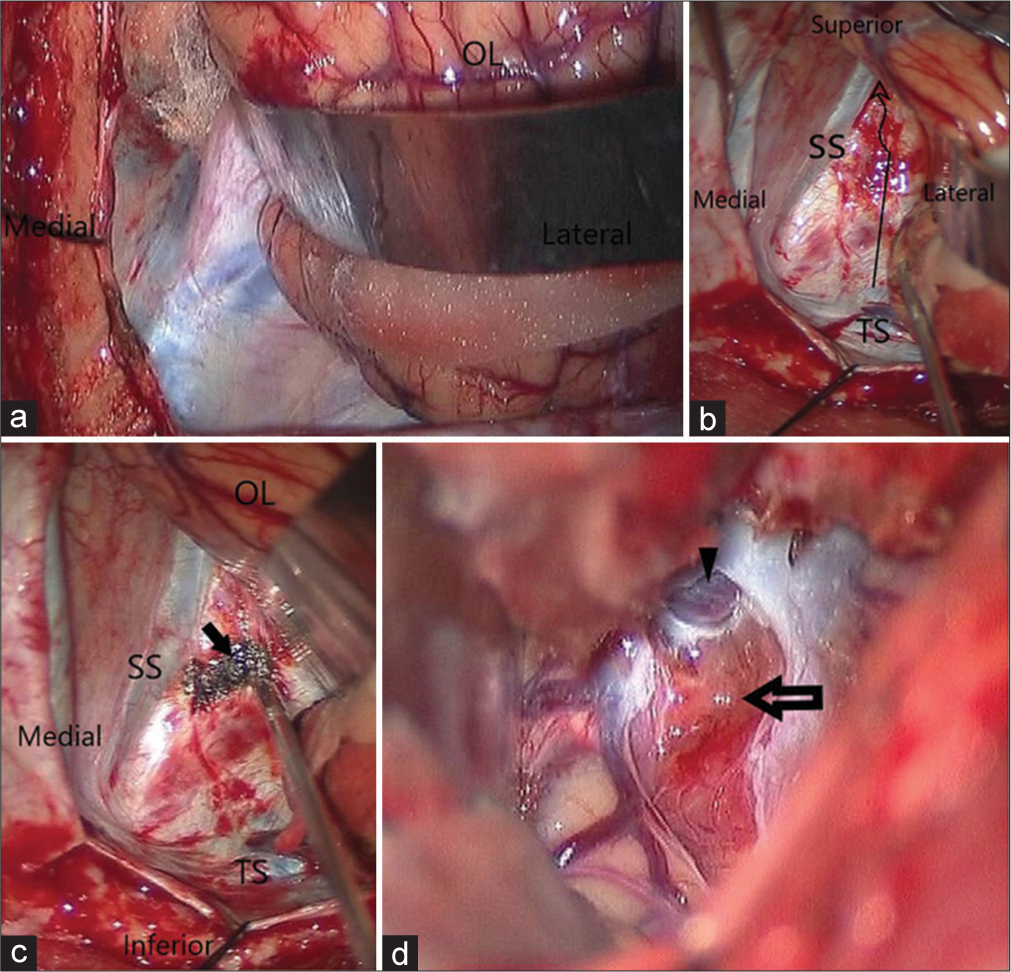
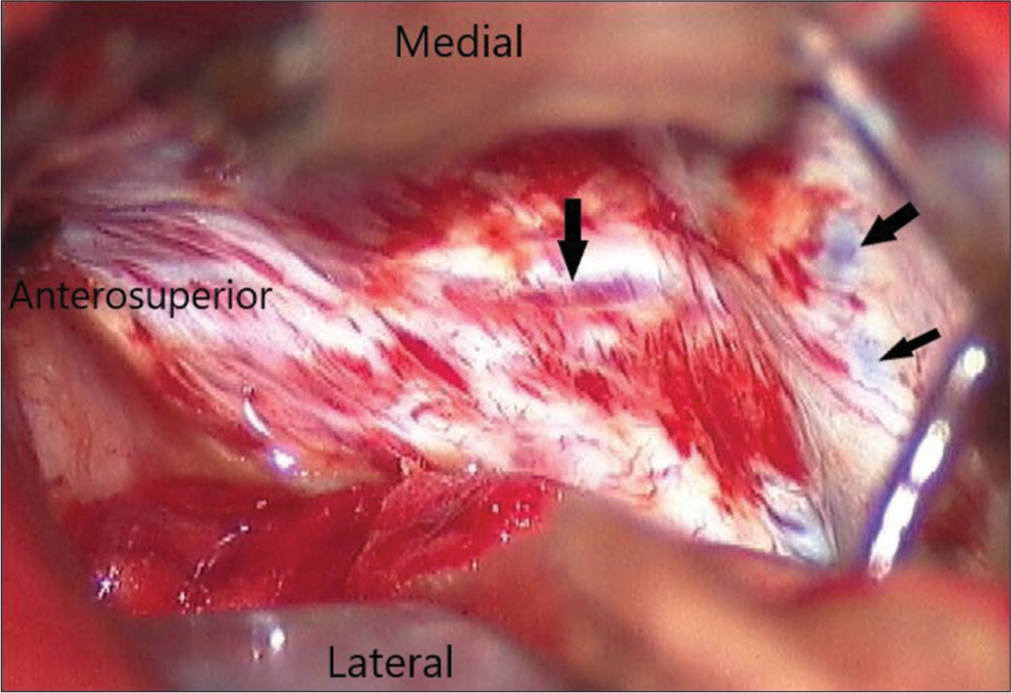
Figure 3:
(a) Intraoperative view of tentorium cerebelli on retracting the occipital lobe (OL). (b) Method of cutting the tentorium cerebelli in antero superomedial direction. (c) Tentorium cauterised at the site of incision. (d) Intraoperative transtentorial view of pineal region lesion after incising the tentorium (arrow). Vein of galen with intact surrounding arachnoid can be seen (arrowhead). OL: Occipital lobe, SS: Straight sinus, TS: Transverse sinus.
For large tumors, falcotentorial, and posterior thalamic, PIH was combined with OT. The resection was defined as gross total, if the lesion was completely removed with no residual lesion detected on the postoperative CT scan, near total resection if more than 90% of the lesion was removed and subtotal resection if <90% of the lesion was removed. Assessment of surgical outcome was done in terms of anatomical accessibility, extent of tumor resection and histopathological diagnosis, and postoperative recovery evaluation was done by Modified Rankin Scale and the postoperative follow-up was done periodically after a week, 1 month, and 3 months.
RESULTS
Thirty-one patients, 15 females and 16 males, age group between 2 and 67 years (mean age 26.4 years) were operated by OT approach for lesions located in pineal region. The procedures were performed in prone and lateral positions because these were simple, safe, and significantly decreased the operative distance. This included one patient where surgery was abandoned due to excessive bleeding from sinuses during craniotomy. Hence, excluding this patient, the study was carried out in the remaining 30 subjects. In a patient with residual tumor who presented with regrowth, intact arachnoid around deep venous system was a good landmark to recognize neighboring structures and helped in tumor removal. There was no difficulty in retracting occipital lobe also.
In one girl child, tuberculomas were located on tentorial surface of cerebellum, but intact large suboccipital venous plexus while approaching from posterior suboccipital approach was the hindering factor to approach this lesion through posterior fossa approach, therefore removed through OT approach. One patient had multiple tuberculomas both supra and infratentorial suboccipital region. Posterior thalamic masses were approached after cutting tent, through suboccipital interhemispheric route.
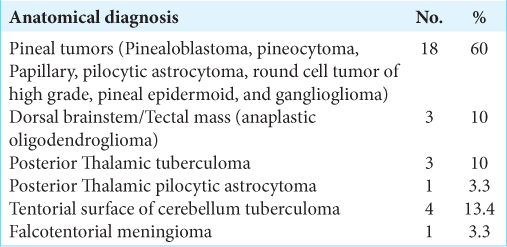
Location of lesion and pathological diagnosis is mentioned in [
The mean angle between the tentorium and occipital surface of cerebellum (tentorial angle) was measured. The 51 degrees minimum and 83 degrees maximum tentorial angle was observed with a mean of 62.08 ± 7.17 degrees. All cases irrespective of the acuteness of tentorial angle and location of the deep venous system were operated by same approach.
Out of 30 study subjects, TS was found to be dominant on the right side in 13 (47.1%) cases and the left side in 17 (52.9 %) cases [

Histopathological diagnosis of the lesions that were operated using this approach was five pineocytomas, three pinealoblastomas, five pilocytic astrocytomas, two pineal epidermoid, seven tuberculomas, three anaplastic oligodendrogliomas, one PNET, one ganglioglioma, one metastatic small cell carcinoma, one pineal parenchymal tumor, and one meningioma [
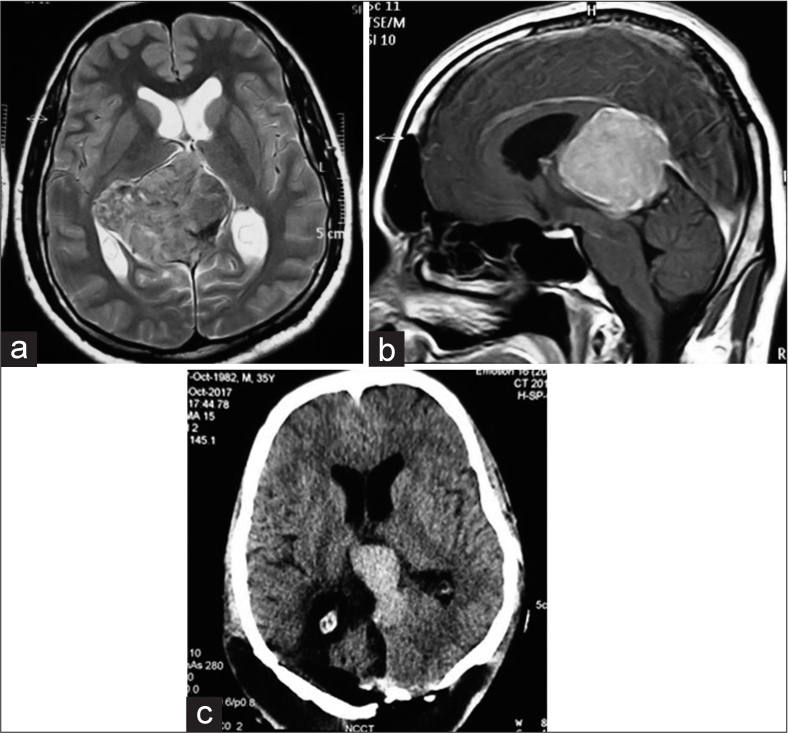
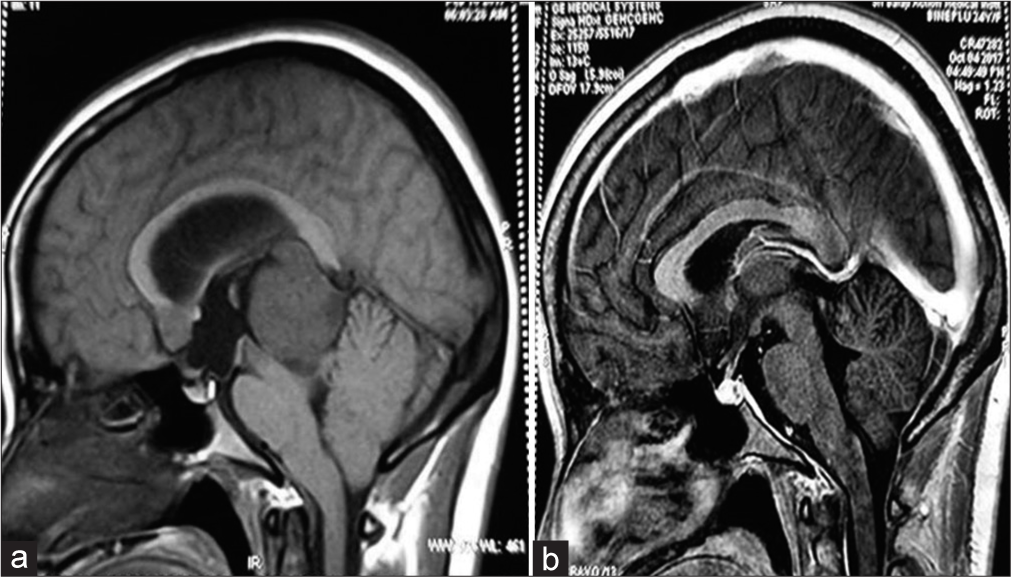
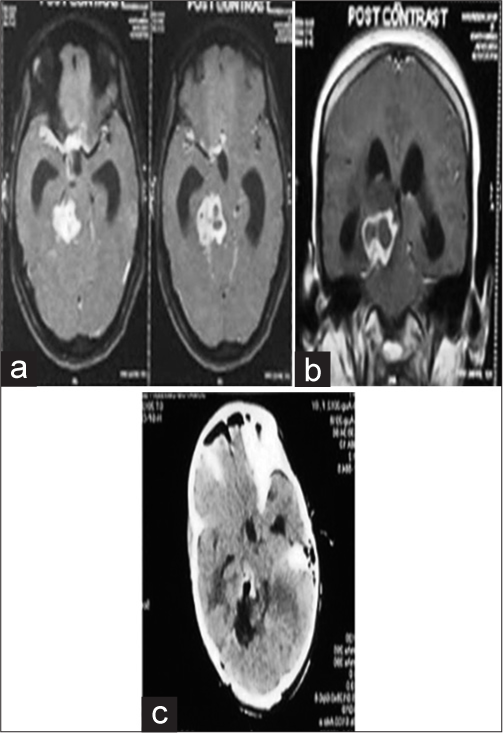
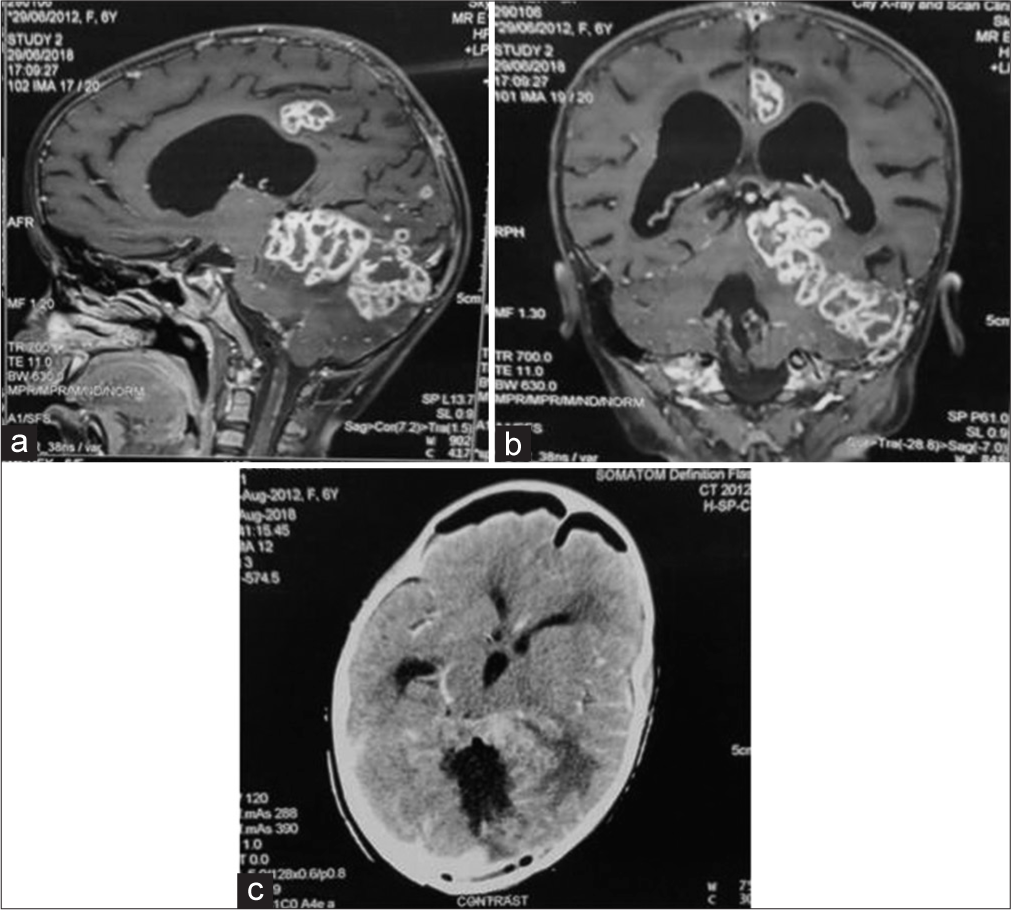
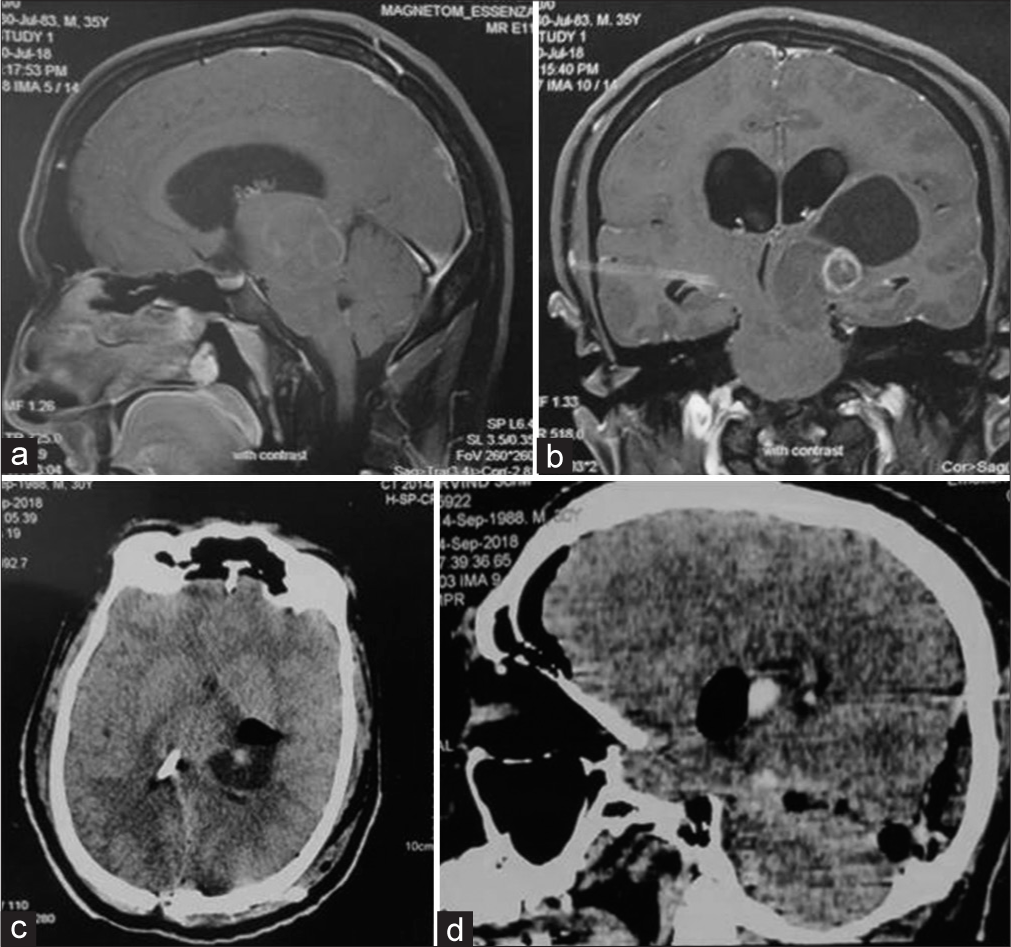
Figure 9:
(a) A case of posterior thalamic pilocytic astrocytoma with both supra and infratentorial extension, with involvement of midbrain. (b) Coronal view. (c) Postoperative image of same patient showing gross total tumor removal, vp shunt tube is seen in situ. (d) Postoperative computed tomography scan in sagittal view of the same patient.
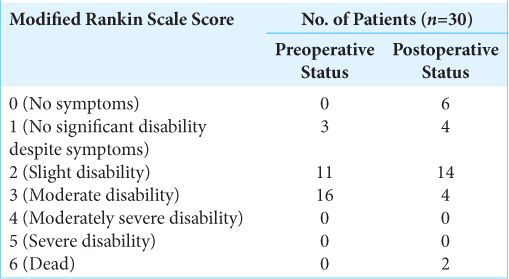
Few complications were encountered in the postoperative period. Superior gaze palsy was present preoperatively as well as postoperatively in two patients. Visual field defects in the form of homonymous hemianopia developed in two patients at the end of 1 week (P = 0.47). At the end of 1 and 3 months, however, only one patient had residual homonymous hemianopia (P = 0.98). The modified Rankin scale in the postoperative period for majority of the patients (14) was 2. The mean modified Rankin scale score was 1.8 which indicated slight postoperative disability. There were 2 postoperative mortalities due to uncontrolled postoperative seizure and acute hydrocephalus each [
DISCUSSION
The pineal region can be the site of many central nervous system lesions, being responsible for 3–8% of the pediatric brain tumors and 0.4–1% of adult tumors.[
Historical perspective
The OT approach was described by Heppner in 1959 and popularized by Poppen. He was an American neurosurgeon, who operated a case of pinealoma using this approach in 1966 and published a series of 25 patients of pineal region lesions along with Marino in 1968.[
Ausman et al. described a modified 3/4 prone, operated side down, occipitalparietal, transtentorial approach to the pineal region in which surgery was performed with the head placed in the threequarter prone position with the operated side down.[
The present series includes both pediatric and elderly patients with mean age of 26.47 years. The youngest patient in this series was 3 years old, and maximum of 67 years, with a mean age of 26.47 years. Maselli et al.[
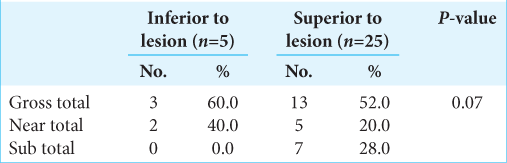
As suggested by Joaquim et al.,[
In this study, the VOG was found superiorly located with respect to the lesion in 25 (83.3%) cases, and inferiorly in 5 (16.7%) of cases. Gross and near total resection was achieved in all cases where the VOG was inferiorly located and in 72% of cases where the VOG was superiorly located in relation to the lesion. The subtotal resection happened due to infiltrative nature of the tumor and or unfavorable consistency of the tumor. In OT approach, the tumor and the venous system are visible in the same field on cutting the tentorium unlike infratentorial supra-cerebellar approach where venous system is visible or encountered after removing the tumor. This avoids the need of dissecting arachnoid encasing the veins. This may leave this area untouched and act as landmark to reach this site in recurrent surgery as was seen in one case in this study. The location of deep venous system had never been the limiting factor in removing the tumor in all the cases in this study which is in contrast to the conventional teaching, that is, if the deep venous system is superiorly placed in relation to lesion, SCIT and if below the lesion OT approach is indicated. We can preserve the precentral cerebellar vein in this approach which is sacrificed in other approaches; however, its sacrifice may not affect the outcome. This was in contrast with the observations made by Goto et al.[
The lesions extending lateral to the midline with supratentorial extensions above the deep venous system, that is, those involving the lateral ventricle, posterior thalamus, or splenium of the corpus callosum require exposure to avoid undue retraction of brain which was achieved by this approach. In these cases combining PIH with OT may provide wider exposure. Lesions that extend dorsolateral to the brainstem, near the ambient cistern, and that extend inferiorly into the depths of the precentral cerebellar fissure near the fourth ventricular roof, inferior colliculus, and anterior vermis can also be exposed by the said approach as was also done in this series. Infiltration into surrounding structures was the limiting factor in complete tumor removal.
The parieto-occipital craniotomy is challenging as it requires exposure of SSS, TS, and SS. While cutting the bone, dura should be totally reflected from underlying bone to avoid injury to any of the sinus mentioned as was also the cause of abandoning a case in this series. Big tumors definitely require dural hitch sutures at SSS and TS level to avoid posttumor removal bleeding from hanging draining veins, which can be life threatening. Suzuki et al.[
Retraction of occipital lobe can be started first from the inferior side to locate the SS, SSS, TSs and starting the cutting of the tentorium 1–1.5 cm parallel to SS. In the middle of cutting of the tent, the microscope is angulated and the incision is preceded supero-medially toward the splenium and is completed till the free edge of tentorium cerebelli. These steps would help in keeping the trajectory toward deep venous system, as was done in all the cases in this series and was successful in all the cases. Our method differed from the original Poppen’s method where the tentorium was cut in a wedge shape with ligation of bridging veins; after a trephine craniotomy.[
There is paucity in the literature regarding extent of resection and functional outcome for various lesions requiring OT approach, most likely as a consequence of the relatively low frequency of the pineal region lesions, understanding the tentorial angulation, and technique of cutting the tent. OT approach requires retraction of occipital lobe and cutting of tentorium which can be performed in either lateral or prone position. Splitting the tentorium offers a panoramic supra- and infratentorial view of the tumor, the surrounding deep venous structures and the collicular plate of the midbrain; hence, the lesions with both supra and infratentorial extension can be resected by this approach.
Moreover, this position is better than sitting, that is, occipital approach is preferable if the tumor is vascular and in patients with associated comorbidities where sitting position is a relative contraindication. The OT is advocated in pineal region lesions mainly with steep tentorial angle, which limits the resection through the SCIT approach where excessive retraction or even resection of part of the upper cerebellar vermis may be necessary to reach the lesion.[
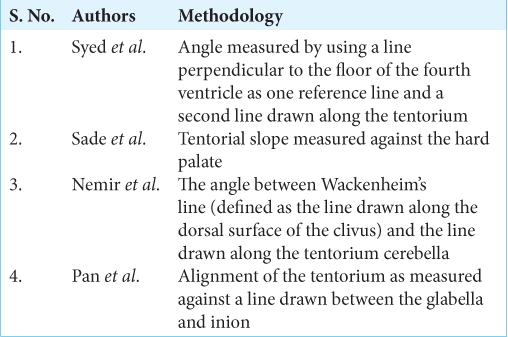
The tentorial angle was measured against a line joining the torcula to the plane of the fourth ventricle. The advantage of this method was its ability to accurately describe the slope of the tentorium, without underestimating it in case of a low lying torcula.[
Few complications were encountered in the study. In one case, surgery was abandoned due to excessive bleeding from the SSS and torcula during craniotomy. Visual field defects in the form of homonymous hemianopia developed in two patients postoperatively and persisted at the end of 1 week. At the end of 1 and 3 months; however, only one patient had residual homonymous hemianopia. This was probably due to prolonged retraction followed by ischemic insult of the inferomedial surface of the occipital lobe and due to firm tumor consistency leading to increased operating time in these cases. However, the retraction associated deficits can be minimized by using multiple retractors, preoperative CSF diversion procedures (as used in the present series), intraoperative CSF drainage by ventricular puncture of the occipital horn and intermittent retraction.[
The postoperative surgical outcome as assessed by modified Rankin scale in majority of the patients (14) was 2. The mean modified Rankin scale score was 1.8 which indicated slight postoperative disability. Similar results were obtained by Maselli et al.[
Limitations
It is an institutional study which focuses on OT approach (mainly in prone or lateral positions) based on surgeon’s preference and hence it is imperative to consider established studies which advocate variation in position for the OT approach (i.e. three quarter prone position) for better and satisfactory surgical outcomes. Moreover, no comparative analysis is done among the various other surgical approaches for pineal region lesions in this series.
CONCLUSION
The pineal region masses occur in both extremes of age, that is, in pediatric and elderly population. The OT approach can be tailored to achieve high rates of resectability irrespective of the status of the deep venous system. The anatomical angles such as the tentorial angle have no correlation with tumor resectability and postoperative surgical outcome in the patients of pineal region mass operated by the OT approach.
The OT approach is a reasonably safe approach provided the craniotomy is made cautiously for the surgical management of pineal region lesions where high resectability rates can be achieved, with slight postoperative morbidity.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Publication of this article was made possible by the James I. and Carolyn R. Ausman Educational Foundation.
Conflicts of interest
There are no conflicts of interest.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Publication of this article was made possible by the James I. and Carolyn R. Ausman Educational Foundation.
Conflicts of interest
There are no conflicts of interest.
References
1. Ausman JI, Malik GM, Dujovny M, Mann R. Three-quarter prone approach to the pineal-tentorial region. Surg Neurol. 1988. 29: 298-306
2. Azab WA, Nasim K, Salaheddin W. An overview of the current surgical options for pineal region tumours. Surg Neurol Int. 2014. 5: 39
3. Bloomfield SM, Sonntag VK, Spetzler RF. Pineal region lesions. Barrow Neurol Inst Q. 1985. 1: 10-23
4. Brotchi J, Levivier M, Raftopoulos C, Dewitte O, Pirotte B, Noterman J. Three-quarter prone approach to the pinealtentorial region. Report of seven cases. Acta Neurochir Suppl (Wien). 1991. 53: 144-7
5. Goto T, Ohata K, Morino M, Takami T, Tsuyuguchi N, Nishio A. Falcotentorial meningioma: Surgical outcome in 14 patients. J Neurosurg. 2006. 104: 47-53
6. Isaac JA, Brian H, Jason B, Martin M, Richard GE. A single-institution experience with pineal region tumors: 50 tumors over 1 decade. Oper Neurosurg (Hagerstown). 2017. 13: 566-75
7. Jamieson KG. Excision of pineal tumors. J Neurosurg. 1971. 35: 550-3
8. Joaquim AF, dos Santos MJ, da Silva ÉG, Tedeschi H. Interhemispheric occipital transtentorial approach to the pineal region and dorsal midbrain. J Bras Neurocir. 2009. 20: 22-6
9. Kobayashi S, Sugita K, Tanaka Y, Kyoshima K. Infratentorial approach to the pineal region in the prone position: Concorde position. Technical note. J Neurosurg. 1983. 58: 141-3
10. Li D, Zhang H, Jia W, Zhang L, Zhang J, Liu W. Significance of the tentorial alignment in protecting the occipital lobe with the poppen approach for tentorial or pineal area meningiomas. World Neurosurg. 2017. 108: 453-9
11. Maselli G, Paulis D, Ricci A, Galzio R. Posterior cranial fossa tumours: Results and prognostic factors in a consecutive series of 14 operated patients by occipital transtentorial approach. Surg Neurol Int. 2012. 3: 85
12. Matsuo S, Baydin S, Güngör A, Middlebrooks EH, Komune N, Iihara K. Prevention of postoperative visual field defect after the occipital transtentorial approach: Anatomical study. J Neurosurg. 2018. 129: 188-97
13. Moshel Y. A occipital transtentorial approach to the precentral cerebellar fissure and posterior incisural space. Neurosurgery. 2009. 65: 554-64
14. Mottolese C, Szathmari A, Beuriat PA. Incidence of pineal tumours. A review of the literature. Neurochirurgie. 2015. 61: 65-9
15. Nemir J, Njirić N, Ivanković D, Barl P, Domazet I, Radoš M. Tentorial alignment and its relationship to cisternal dimensions of the pineal region: MRI anatomical study with surgical implications using the new clivotentorial method. Clin Neurol Neurosurg. 2018. 172: 99-10
16. Poppen JL, Marino R. Pinealomas and tumors of the posterior portion of the third ventricle. J Neurosurg. 1968. 28: 357-64
17. Poppen JL. The right occipital approach to a pinealoma. J Neurosurg. 1966. 25: 706-10
18. Rhoton AL. The tentorial incisura. Neurosurgery. 2000. 47: 93-129
19. Sano K. Pineal region tumors: Problems in pathology and treatment. Clin Neurosurg. 1983. 30: 59-91
20. Sharma M, Madhugiri V, Nanda A, James L. Poppen and surgery of the seat of the soul: A contemporary perspective. World Neurosurg. 2014. 82: 529-34
21. Simon E, Afif A, M’Baye M, Mertens P. Anatomy of the pineal region applied to its surgical approach. Neurochirurgie. 2015. 61: 70-6
22. Suzuki Y, Nakajima M, Ikeda H, Abe T. Three-dimensional computed tomography angiography of the galenic system for the occipital transtentorial approach. Neurol Med Chir (Tokyo). 2005. 45: 387-94
23. Syed HR, Jean WC. A novel method to measure the tentorial angle and the implications on surgeries of the pineal region. World Neurosurg. 2018. 111: e213-20
24. Tanaka R, Washiyama K. Occipital transtentorial approach to pineal region tumours. Oper Tech Neurosurg. 2009. 6: 215-21



James Ausman
Posted October 9, 2021, 5:52 pm
This is an outstanding summary of a large number of personal cases on pineal region tumors with a thorough review of the literature back to the 1959. The authors describe their experience in detail so that the reader can benefit from their surgical series. The photographs are very helpful in reading this paper. The analysis of the literature in regard to their patients provides more support for their OT approach to these lesions. The reader should benefit greatly from this work in operating on these lesions. The authors do answer the controversies learned in conventional teaching. This is a first rate paper and a model for others on how a scholarly work can be accomplished anywhere in the world by thoughtful clinical neurosurgeons and scientists.