

- Department of Neurosurgery, San Salvatore City Hospital L’Aquila, Italy
- Department of Life, Health and Environmental Sciences (MESVA), University of L’Aquila, L’Aquila, Italy
Correspondence Address:
Danilo De Paulis
Department of Life, Health and Environmental Sciences (MESVA), University of L’Aquila, L’Aquila, Italy
DOI:10.4103/2152-7806.198728
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Alessandro Ricci, Hambra Di Vitantonio, Danilo De Paulis, Mattia Del Maestro, Massimo Gallieni, Soheila Raysi Dechcordi, Sara Marzi, Renato Juan Galzio. Parasagittal meningiomas: Our surgical experience and the reconstruction technique of the superior sagittal sinus. 19-Jan-2017;8:1
How to cite this URL: Alessandro Ricci, Hambra Di Vitantonio, Danilo De Paulis, Mattia Del Maestro, Massimo Gallieni, Soheila Raysi Dechcordi, Sara Marzi, Renato Juan Galzio. Parasagittal meningiomas: Our surgical experience and the reconstruction technique of the superior sagittal sinus. 19-Jan-2017;8:1. Available from: http://surgicalneurologyint.com/surgicalint_articles/parasagittal-meningiomas-our-surgical-experience-and-the-reconstruction-technique-of-the-superior-sagittal-sinus/
Date of Submission
01-Jun-2016
Date of Acceptance
08-Nov-2016
Date of Web Publication
19-Jan-2017
Abstract
Background:The radical resection of parasagittal meningiomas without complications and recurrences is the goal of the neurosurgeon. Nowadays, different managements are proposed. This study describes our surgical technique during the lesional excision and the reconstruction of the superior sagittal sinus (SSS).
Methods:The total removal (Simpson I and II) of parasagittal meningiomas (WHO grade I and II) was obtained in 75 patients from September 2000 to January 2010. The indocyanine green videoangiography was used before the dural opening and, when necessary, to identify and preserve the cortical veins. The surgery of the SSS was performed in accordance with Sindou's classification, and its reconstruction was achieved through the use of a patch of galea capitis.
Results:We had no cases of recurrence and thrombotic occlusion of the SSS in 5 years after the reconstruction. No complications were observed in 65 patients, and no cases of mortality were reported. Neurological focal deficits were observed in 5 patients. A brain swelling and a venous infarction were observed in 1 patient. Only one case of thrombotic occlusion was observed. A cerebrospinal fluid leak was observed in 2 patients, and a systemic complication was found in 1 patient.
Conclusion:Several factors contribute to the success of the parasagittal meningioma surgery. We consider the preservation of the cortical veins to be important, and, when possible, we recommend the reconstruction of the anterior third of the SSS. Our experience has led us to believe that until now surgery is a winning choice if practiced by expert hands.
Keywords: Collateral and cortical veins, galea capitis, parasagittal meningioma, superior sagittal sinus
INTRODUCTION
The radical resection of the parasagittal meningiomas without complications is the goal of the neurosurgeon.[
Moreover, because of the lack of a published large series regarding the parasagittal meningiomas invading the superior sagittal sinus (SSS), there are no definitive guidelines for the management of these complex cases.[
Nowadays, different managements are proposed. Some neurosurgeons consider the SSS invasion as a contraindication for a complete resection, although the subtotal resection is associated with a high rate of tumor recurrence,[
In this study, we describe our experience during the surgical excisions of the parasagittal meningiomas involving the anterior, middle, and posterior third, as well as in detail the surgical technique used for the sinus reconstruction and the preoperative and perioperative patient management. Finally, we examine the frequency and nature of the complications.
MATERIALS AND METHODS
This study is a retrospective review of 75 parasagittal meningiomas operated at our center by the senior author between September 2000 and January 2010. In all the patients included in the study, a total removal of the meningiomas equivalent to Simpson grade I or II and a histopathological diagnosis of the meningiomas with WHO grade I and II were obtained.
The data regarding the topography of meningiomas, sex, and average age of the patients are reported in
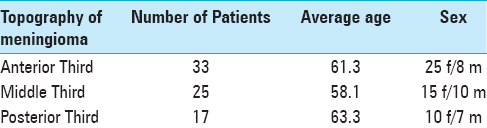
The preoperative diagnosis of the meningioma was done on computed tomography (CT) scan and contrast-enhancement magnetic resonance imaging (MRI). The patients also underwent a preoperative vascular imaging with the venous MRI angiography (vMRI), however, we did not use the digital subtraction angiography (DSA) with any of them.
The intraoperative neurophysiologic monitoring with electroencephalography (EEG), somatosensory evoked potentials (SSEPs), motor evoked potentials (MEPs) and, in selected cases, visual evoked potentials (VEPs) were performed.
A computerized neuronavigation was used to plan the skin incision and the craniotomy to completely remove the lesion avoiding damages to the SSS.
In all cases of treated meningiomas, a flap of galea capitis was always prepared during the surgical approach both for the possibility of reconstructing the SSS and substituting the dura mater infiltrated by the meningioma. In the last case, if the galea capitis was not sufficient, the author used a flap of autologous fat.[
The indocyanine green videoangiography (ICGV) was used during the following: before opening the dura,[
The degree of invasion of the sinus was defined according to the Sindou's classification,[

Figure 1
Reproduction of the Sindou classification. Type I: Meningioma attached to the outer surface of the sinus wall; Type II: lateral recess invaded; Type III: lateral wall invaded; Type IV: entire lateral wall and roof of the sinus both invaded; Type V: sinus totally invaded with one wall being free; Type VI: sinus totally invaded without any wall being free

In most patients, the anti-edema therapy with dexamethasone was used for 48–72 hours after the surgery, and the enoxaparin was administered for 20 days after the surgery; no antiplatelet therapy was prescribed after the hospitalization.
A postoperative contrast-enhancement MRI and a vMRI were performed within 24 hours after the surgery. After the hospitalization, the postoperative radiological follow-up consisted of an MRI with contrast, plus a vMRI at 6 months and once a year for 5 years.
Surgical technique
The patient is placed under total intravenous anesthesia-target controlled infusion (TIVA-TCI) of propofol and remifentanil.
For the parasagittal meningiomas of the anterior third and the anterior portion of the middle third, the patient is positioned in the supine position, whereas for the tumors of the posterior third and the posterior portion of the middle third we use the prone position.
The preparation of the galea capitis begins with the skin infiltration. The infiltration is made with carbocaine 2% and 20 cc of saline solution and it is performed in two steps. The superficial infiltration is performed between the dermis and the galea capitis and the second one under the periostium. The skin incision is performed up to the dermis for separating it from the superficial layer of the galea [
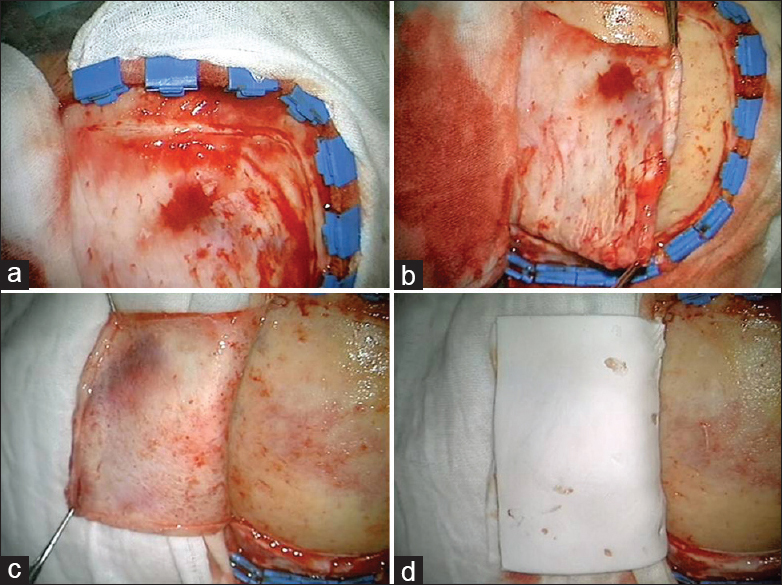
Figure 2
The skin incision is performed up to the dermis for separating it from the superficial layer of the galea (a). The galea capitis is incised along the edge of the skin flap up to the underlying bone (b). In the end, a pedicled galea flap is made (c). It is conserved inside a sandwich of collagen sponge or wet gauzes and then is turned on the skin flap (d)
Based on the neuronavigation data, we perform a craniotomy slightly larger than that of the meningioma of approximately 1.5 cm. Then, owing to a bone flap which extends laterally, the SSS is completely exposed at least 2 cm beyond the SSS to permit the visualization of both sides of the sinus. This is done by making two or more burr holes placed laterally at the SSS and then connected with the craniotome. Before removing the bone flap, the bone is carefully separated from the dura with a periosteal elevator.
Before the dural opening, under microscopic vision, a saline solution with indocyanine green (ICG) is injected as intravenous bolus[
In general, no brain retraction is used.
During the tumor resection, when possible, the collateral veins are recognized and preserved, whereas the tumor drainage veins are coagulated. Through the use of other injections of ICG (the maximal daily dose should not exceed 5 mg/kg), it is possible to distinguish the veins that drain the tumor from the collateral pathways. According to Ferroli et al.,[
The tumor is dissected free from the brain parenchyma throughout its circumference if necessary it is used an ultrasonic aspirator to perform the lesion debulking. The last part of the procedure is directed at the portion of the tumor invading the SSS.
Based on Sindou's classification,[
Type I: peeling of the external layer keeping the inner layer clean, and coagulation of the site of the dura attachment;[ Type II: resection of the intraluminar fragment within the lateral recess,[ Type III: resection of the invaded wall, and repair with a patch of galea capitis sutured with ePTFE No. 6-0; Type IV: resection of the invaded wall and, when possible, peeling with coagulation of the site of the dura attachment, or subtotal resection of the SSS roof. Subsequent reconstruction with a patch of the galea capitis sutured with ePTFE No. 6-0; Type V: after a direct surgical exploration of the sinus lumen, based on the absence or presence of the cortical veins draining in the SSS, it is possible to choose between the two different surgical strategies: Resection of both invaded walls, without reconstruction, with closure of the SSS at a distance of at least 1 cm from the bridging veins; Removal of both invaded walls and reconstruction with a patch of galea capitis sutured with ePTFE No. 6-0. Type VI: removal of the entire involved portion of the sinus without venous bypass.
When the reconstruction is performed, under microscopic vision, a patch of galea capitis is harvested from the previously prepared pedicled galea flap. The size of the patch depends on the size of the repair and the patch is conserved temporarily in a saline solution.
The SSS is opened with excision of the wall infiltrated [Figure
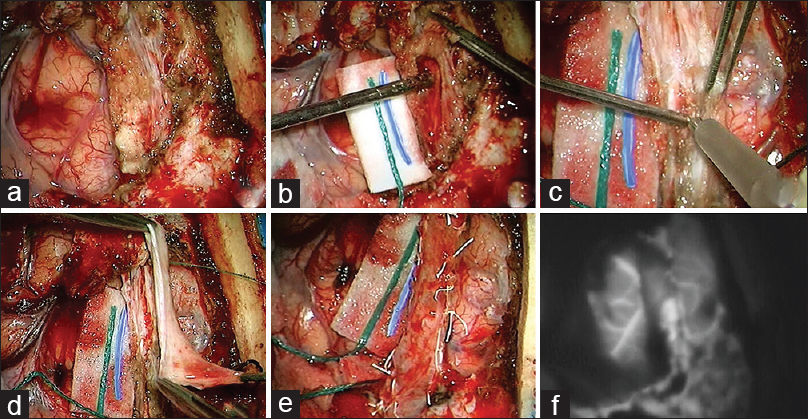
Figure 3
The lesion was exposed through a tailored craniotomy (a), with optimal exposition of the superior sagittal sinus (SSS). The lesion was progressively debulked with removal of the infiltrated dura mater, sparing all the perilesional veins. The SSS was opened (b) with excision of its superolateral wall and both the extremities were filled with micropads. The intrasinusal part of the tumor was removed using an ultrasonic aspirator (c). Then, the sinus was reconstructed with a patch of autologous galea capitis sutured with a running ePTFE No. 6-0 suture. Subsequently, micropatties were pulled out with restoration of the blood flow (d, e). At the end of the procedure, the patency of the SSS and bridging veins was evidenced by intraoperative ICGV (f)
During the running locked suture, the edges of the galea capitis must be stretched [
In all cases of reconstruction, another injection of ICG is performed to confirm the patency of the reconstructed SSS [
When possible, to avoid the risk of a thrombotic occlusion, in type V and VI meningiomas it is important to close the SSS at a distance of 1 cm from the bridging veins. This is particularly important in the bridging veins of the central group in the middle-third portion of the sagittal sinus.
In the end, the infiltrated dura mater is reconstructed with another patch of galea capitis or of abdominal autologous fat.[
ILLUSTRATIVE CASE
A 53-year-old female patient with a parasagittal meningioma of the middle third (type V of Sindou's classification) was operated. The preoperative brain MRI, in axial, coronal, and sagittal T1 weighted images with Gadolinium, revealed a left parasagittal extra-axial tumor with a homogeneous enhancement, originating from the middle-third of the superior sagittal sinus [Figure
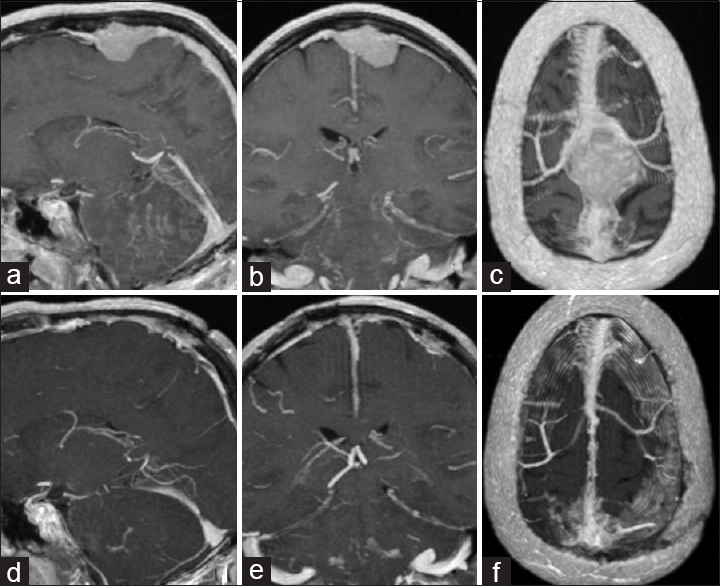
Figure 4
Preoperative brain MRI in axial, coronal, and sagittal T1 weighted images with gadolinium revealed a left parasagittal extra-axial tumor, with homogeneous enhancement, originating from the third median part of the superior sagittal sinus (a-c). Postoperative brain MRI in axial, coronal and sagittal T1 weighted images with gadolinium revealed the complete removal of the lesion and the patency of the reconstructed superior sagittal sinus (d-f)
A double skin infiltration and a pedicled flap of galea capitis were performed [
Using neuronavigation, the lesion was exposed through a tailored craniotomy to permit an optimal exposition of the SSS [
RESULTS
At our institute, between September 2000 and January 2010, 75 patients underwent the excision of a parasagittal meningioma obtaining Simpson grade I or II and a histopathological diagnosis WHO grade I or II. In 21 cases, we performed the reconstruction of SSS with the galea capitis. The technique was applied in all cases for the types III and IV. For the presence of suppletive venous drainage, in type V, we performed the SSS reconstruction only in 4 patients; 2 cases of anterior third, 1 case of middle third, and 1 case of posterior third.
No perioperative complications were observed in 65 patients and no cases of mortality were reported. We had no cases of recurrence and thrombotic occlusion of the SSS in 5 years after the reconstruction.
The summary of the complications according to the types of meningiomas is discussed in
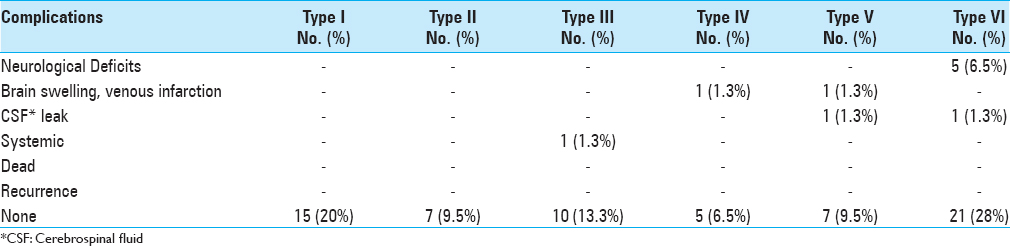
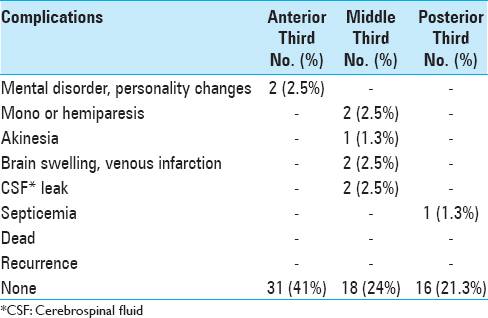
A brain swelling and a venous infarction were observed in 1 patient with type IV meningioma of the middle third, which were caused by an infarction secondary to the injury of the collateral veins. After the re-operation, the patient survived with severe neurological disabilities.
Another thrombotic occlusion with consequent infarction was observed in a parasagittal meningioma of the middle third (Type V, without reconstruction of the SSS). In this case, the patient was re-operated with a complete restoring of the neurological abilities.
Neurological deficits were observed in 5 patients with meningiomas type VI. These deficits were observed in 2 patients with meningiomas of the anterior-third and in 3 patients with meningiomas of the middle-third. The patients with anterior-third meningiomas presented permanent mental disorders and personality changes due to the coagulation of the frontal veins. In the middle-third meningiomas, neurological deficits were transient.
A cerebrospinal fluid (CSF) leak was observed in 2 patients with middle-third meningiomas, and a systemic complication (septicemia) was found in 1 patient.
No cases of intracranial hypertension, progressive loss of vision, and/or encephalopathy were observed after the removal of the meningiomas type V and VI located in the posterior third of the SSS.
DISCUSSION
Cushing and Eisenhardt defined parasagittal meningiomas as tumors filling the parasagittal angle with no brain tissue between the tumors themselves and the SSS. Sometimes, they partially or completely invade the SSS.[
Nowadays, radiosurgery offers a valuable aid,[
We recommend the preparation of a galea capitis flap because it is an autologous material, inexpensive, well-tolerated, easy to obtain, and useful for the reconstruction of the SSS. Furthermore, the use of a pericranium patch avoids the heterologous material implant or the need for a levy of autologous veins.
The skin flap and the craniotomy must be wider than the meningioma.[
The use of the neuronavigation is always recommended because it first allows to perform a surgical approach tailored to each patient, second to decrease the recurrence rate, the blood loss, and the length of stay, and finally to improve the recurrence-free survival and the performance status.[
According to Nussbaum,[
During the excision of the tumor, it is mandatory to preserve the bridging, especially those of the rolandic area through their dissection from the tumor and adjacent brain.[
According to the literature data, the anterior third of the SSS has traditionally been thought expendable.[
To our knowledge, before the reconstruction of the SSS with a galea capitis, a temporary occlusion of the distal and proximal lumen of the sinus can be performed with surgical patties without the use of small pledgets of haemostatic material. Sindou[
Sindou et al.[
CONCLUSIONS
We have presented our surgical experience and technique of reconstruction of the SSS during the removal of parasagittal meningiomas. The success of this surgery is achieved through a management that starts from the patient's position. It is a surgery that requires a limited and careful manipulation of the venous structures. The use of the ICGV plays a valuable aid in the preservation of collateral veins and it allows to avoid the DSA.
Sindou's classification provides a great help. It allows to establish an appropriate operative scheme during the surgery. Furthermore, we also recommend the reconstruction of the anterior-third of the SSS to avoid changes in personality or mental disorders. In this manner, the respect for the patient's quality of life is prime.
Although new technologies are not available for most neurosurgical centers around the world, in our opinion intraoperative neurophysiologic monitoring (EEG, VEPs, SSEPs, MEPs), ICGV, burst suppression, control hypotension, and hypothermia facilitate the success of the surgery, even though they are not mandatory for a good result.
The absence of mortality, the recurrence at 5 years, and low complications in low-grade meningiomas let us believe that at present surgery is a winning choice, if practiced by expert hands.
Consent
Written informed consent was obtained from the patients for publication of this technical report and any accompanying images.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
The authors thank Maria Silvia Marottoli for her assistance in the translation.
References
1. Bederson JB, Eisenberg MB. Resection and replacement of the superior sagittal sinus for treatment of a parasagittal meningioma: Technical case report. Neurosurgery. 1995. 37: 1015-8
2. Bir SC, Konar SK, Maiti TK, Thakur JD, Guthikonda B, Nanda A. Utility of Neuronavigation in Intracranial Meningioma Resection: A Single-Center Retrospective Study. World Neurosurg [Epub ahead of print]. 2016. p.
3. Bonnal J, Brotchi J. Surgery of the superior sagittal sinus in parasagittal meningiomas. J Neurosurg. 1978. 48: 935-45
4. Brotchi J. Should we pursue superior sagittal sinus grafting in parasagittal meningiomas in 2013?. World Neurosurg. 2014. 82: 325-6
5. Caroli E, Orlando ER, Mastronardi L, Ferrante L. Meningiomas infiltrating the superior sagittal sinus: Surgical considerations of 328 cases. Neurosurg Rev. 2006. 29: 236-41
6. Cushing H, Eisenhardt L.editors. Meningiomas: Their Classification, Regional Behavior, Life History, and surgical End Results. Springfield, IL: Charles C. Thomas; 1938. p.
7. d’Avella E, Volpin F, Manara R, Scienza R, Della Puppa A. Indocyanine green videoangiography (ICGV)-guided surgery of parasagittal meningiomasoccluding the superior sagittal sinus (SSS). Acta Neurochir. 2013. 155: 415-20
8. Desse N, Malikov S, Fuentes S, Pech-Gourg G, Graillon T, Dufour H. Superior sagittal sinus reconstruction using a femoral venous graft after total removal of ameningioma. Case report. Neurochirurgie. 2013. 59: 43-6
9. Di Meco F, Li KW, Casali C, Ciceri E, Giombini S, Filippini G. Meningiomas invading the superior sagittal sinus: Surgical experience in 108 cases. Neurosurgery. 2004. 55: 1263-72
10. Di Vitantonio H, De Paulis D, Del Maestro M, Ricci A, Dechordi SR, Marzi S. Dural repair using autologous fat: Our experience and review of the literature. Surg Neurol Int. 2016. 7: S463-8
11. Ferroli P, Acerbi F, Tringali G, Albanese E, Broggi M, Franzini A. Venous sacrifice in neurosurgery: New insights from venous indocyanine green videoangiography. J Neurosurg. 2011. 115: 18-23
12. Ferroli P, Nakaji P, Acerbi F, Albanese E, Broggi G. Indocyanine green (ICG) temporary clipping test to assess collateral circulation before venous sacrifice. World Neurosurg. 2011. 75: 122-5
13. Hakuba A, Huh CW, Tsujikawa S, Nishimura S. Total removal of a parasagittal meningioma of the posterior third of the sagittal sinus and its repair by autogenous vein graft. Case report. J Neurosurg. 1979. 51: 379-82
14. Hoessly GF, Olivecrona H. Report on 280 cases of verified parasagittal meningioma. J Neurosurg. 1955. 12: 614-26
15. Kondziolka D, Flickinger JC, Perez B. Judicious resection and/or radiosurgery for parasagittal meningiomas: Outcomes from a multicenter review. Gamma Knife Meningioma Study Group. Neurosurgery. 1998. 43: 405-13
16. Lee JM, Jung S, Moon KS, Seo JJ, Kim IY, Jung TY. Preoperative evaluation of venous systems with 3-dimensional contrast-enhanced magnetic resonance venography in brain tumors: Comparison with time-of-flight magnetic resonance venography and digital subtraction angiography. Surg Neurol. 2005. 64: 128-33
17. Ma J, Song T, Hu W, Muhumuza ME, Zhao W, Yang S. Reconstruction of the superior sagittal sinus with silicone tubing. Neurosurg Focus. 2002. 12: ecp1-
18. Mantovani A, Di Maio S, Ferreira MJ, Sekhar LN. Management of meningiomas invading the major dural venous sinuses: Operative technique, results, and potential benefit for higher grade tumors. World Neurosurg. 2014. 82: 455-67
19. Marks SM, Whitwell HL, Lye RH. Recurrence of meningiomas after operation. Surg Neurol. 1986. 25: 436-40
20. Mathiesen T, Pettersson-Segerlind J, Kihlström L, Ulfarsson E. Meningiomas engaging major venous sinuses. World Neurosurg. 2014. 81: 116-24
21. Menovsky T, De Vries J. Cortical vein end-to-end anastomosis after removal of a parasagittal meningioma. Microsurgery. 2002. 22: 27-9
22. Murata J, Sawamura Y, Saito H, Abe H. Resection of a recurrent parasagittal meningioma with cortical vein anastomosis: Technical note. Surg Neurol. 1997. 48: 592-5
23. Naumann M, Meixensberger J. Factors influencing meningioma recurrence rate. Acta Neurochir. 1990. 107: 108-11
24. Nowak A, Dziedzic T, Czernicki T, Kunert P, Marchel A. Surgical treatment of parasagittal and falcine meningiomas invading the superior sagittal sinus. Neurol Neurochir Pol. 2014. 48: 174-80
25. Nussbaum ES, Defillo A, Nussbaum L. The use of indocyanine green videoangiography to optimize the dural opening for intracranial parasagittal lesions. Neurosurgery. 2012. 70: 61-3
26. Oka K, Go Y, Kimura H, Tomonaga M. Obstruction of the superior sagittal sinus caused by parasagittal meningiomas: The role of collateral venous pathways. J Neurosurg. 1994. 81: 520-4
27. Pires de Aguiar PH, Aires R, Maldaun MV, Tahara A, de Souza Filho AM, Zicarelli CA. Is sagittal sinus resection in falcine meningiomas a factor of bad surgical outcome?. Surg Neurol Int. 2010. 1: 64-
28. Sindou M. Meningiomas invading the sagittal or transverse sinuses, resection with venous reconstruction. J Clin Neurosci. 2001. 8: 8-11
29. Sindou M. Meningiomas involving major dural sinuses: Should we attempt at radical removal and venous repair?. World Neurosurg. 2014. 81: 46-7
30. Sindou MP, Alvernia JE. Results of attempted radical tumor removal and venous repair in 100 consecutive meningiomas involving the major dural sinuses. J Neurosurg. 2006. 105: 514-25
31. Sindou M, Auque J. The intracranial venous system as a neurosurgeon's perspective. Adv Tech Stand Neurosurg. 2000. 26: 131-216
32. Sindou M, Auque J, Jouanneau E. Neurosurgery and the intracranial venous system. Acta Neurochir Suppl. 2005. 94: 167-75
33. Sindou M, Hallacq P. Venous reconstruction in surgery of meningiomas invading the sagittal and transverse sinuses. Skull Base Surg. 1998. 8: 57-64
34. Raabe A, Beck J, Gerlach R, Zimmermann M, Seifert V. Near-infrared indocyanine green video angiography: A new method for intraoperative assessment of vascular flow. Neurosurgery. 2003. 52: 132-9
35. Raabe A, Beck J, Seifert V. Technique and image quality of intraoperative indocyanine green angiography during aneurysm surgery using surgical microscope integrated near-infrared video technology. Zentralbl Neurochir. 2005. 66: 1-6
36. Zeiler FA, Akoth E, Gillman LM, West M. Burst Suppression for ICP Control: A Systematic Review. J Intensive Care Med. 2015. p.
Commentary
Eric S. Nussbaum- Department of Neurosurgery, National Brain Aneurysm Center at the John Nasseff Neuroscience Institute, St. Paul, Minnesota, USA E-mail:
LNUSSBAUM@comcast.net
The authors should be congratulated for presenting a large series of parasagittal meningiomas treated using surgical excision with excellent results. This group has emphasized the use of reconstruction of the sagittal sinus as an important aspect of aggressive surgical treatment, and we agree with many of the thoughtful points raised by the authors.
At our center, we prefer surgery to stereotactic radiosurgery as the primary treatment modality for parasagittal meningiomas. Anecdotal evidence suggests that these lesions in particular may be at higher than average risk for radiation-induced swelling, possibly because of delayed local venous occlusion. In our experience, the preservation of cortical draining veins at the time of surgery, particularly larger vessels, is critically important. It can be difficult to predict with certainty which veins can be sacrificed safely, and we have therefore used ICGV as a surgical adjunct to help optimize the dural opening, and in particular, to avoid inadvertent injury to cortical veins stretched or distorted by the tumor.[
When the lateral wall of the sagittal sinus is invaded by tumor, we will often open the sinus, remove tumor, and oversew the opening with some form of patch graft. We agree with the authors that even the anterior one-third of the sagittal sinus deserves such reconstruction as we see no disadvantage to attempting local repair, which may be beneficial in selected cases. We have not resected long segments of the sinus using a patch to repair the sinus in an end-to-end fashion, although other centers have supported the use of this technique. When a limited amount of residual tumor is present, we will follow this closely and use radiosurgery as needed. This paradigm has worked well in our experience allowing us to achieve good long-term tumor control balanced with excellent outcomes in the majority of cases. Again, we congratulate the authors on their experience.
References
1. Nussbaum ES, Defillo A, Nussbaum LA. The use of indocyanine green videoangiography to optimize the dural opening for intracranial parasagittal lesions. Neurosurgery. 2011. 70: 61-4
2. Nussbaum ES, Defillo A, Janjua TM, Nussbaum LA. Microvascular Repair of an Injured Cortical Draining Vein. Surg Neurol. 2009. 72: 530-1

