

- Department of Neurological Surgery, Juntendo University Urayasu Hospital, Urayasu, Japan.
Correspondence Address:
Satoshi Tsutsumi, Department of Neurological Surgery, Juntendo University Urayasu Hospital, Urayasu, Japan.
DOI:10.25259/SNI_29_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Hideaki Ueno, Satoshi Tsutsumi, Yasutoshi Akasaki, Kohei Yoshida, Natsuki Sugiyama, Hisato Ishii. Penetrating orbitocranial injury by shoji frame: A rare indoor accident in a Japanese style house. 10-Feb-2023;14:51
How to cite this URL: Hideaki Ueno, Satoshi Tsutsumi, Yasutoshi Akasaki, Kohei Yoshida, Natsuki Sugiyama, Hisato Ishii. Penetrating orbitocranial injury by shoji frame: A rare indoor accident in a Japanese style house. 10-Feb-2023;14:51. Available from: https://surgicalneurologyint.com/surgicalint-articles/12147/
Date of Submission
10-Jan-2023
Date of Acceptance
29-Jan-2023
Date of Web Publication
10-Feb-2023
Abstract
Background: To the best of our knowledge, there are no reports of penetrating orbitocranial injury (POCI) caused by a shoji frame.
Case Description: A 68-year-old man fell in his living room and was stuck headfirst by a shoji frame. At presentation, marked swelling was noted in the right upper eyelid, with the edge of the broken shoji frame exposed superficially. Computed tomography (CT) revealed a hypodense linear structure located in the upper lateral sector of the orbit, partially protruding into the middle cranial fossa. Contrast-enhanced CT revealed intact ophthalmic artery and superior ophthalmic vein. The patient was managed with frontotemporal craniotomy. The shoji frame was extracted by pushing out the extradurally located proximal edge from the cranial cavity and simultaneously pulling the distal edge from the stab wound in the upper eyelid. Postoperatively, the patient received intravenous antibiotic therapy for 18 days.
Conclusion: POCI can be caused by shoji frames as a result of an indoor accident. The broken shoji frame is evidently delineated on CT, which can result in prompt extraction.
Keywords: Indoor accident, Penetrating orbitocranial injury, Shoji frame, Treatment
INTRODUCTION
Penetrating non-missile injuries to the head are an infrequent entity that commonly occurs as an accident.[
Shoji is a traditional Japanese style architecture that typically divides the indoor rooms and the hall that faces outdoors. Shoji is commonly wooden, takes the structure of lattice frames over which Japanese papers are stuck, and slides laterally to come and out of the room. Only one penetrating head injury caused by a shoji frame has been reported in literature.[
Herein, we present such a case wherein a shoji frame was successfully extracted through frontotemporal craniotomy.
CASE PRESENTATION
A 68-year-old Japanese man fell in his living room and was stuck headfirst by a shoji frame. The patient visited a local ophthalmologist the day after the injury in the right upper eyelid, where he was suspected of penetrating orbital injury by a broken shoji frame. At presentation, the patient was well oriented. However, marked swelling and redness were noted on the right upper eyelid. In addition, the edge of the broken shoji frame was superficially exposed in the lateral part of the eyelid [

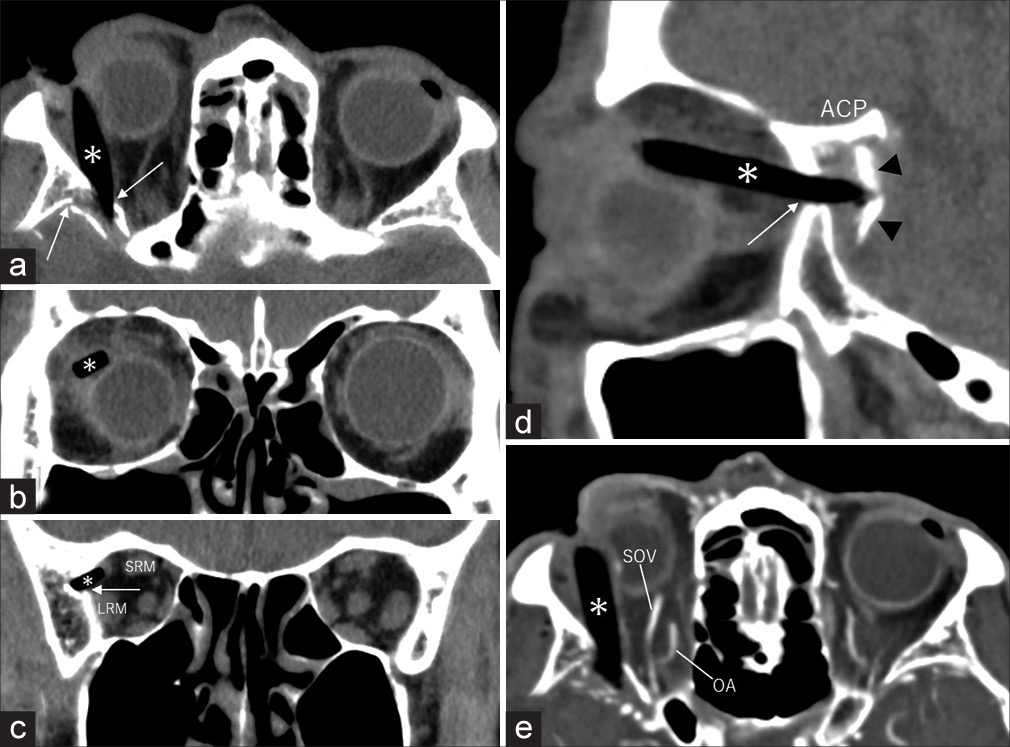
Figure 2:
Non-contrast axial (a), coronal at the equator level of the bulb (b) and orbital apex (c), and sagittal (d) computed tomography, 3 mm in slice thickness, show a homogeneously hypodense, linear structure located in the upper lateral sector of the orbit, partially protruding into the middle fossa. Contrast-enhanced axial computed tomography revealed the ophthalmic artery (OA) and superior ophthalmic vein (SOV) to be intact (e). ACP : Anterior clinoid process, LRM : Lateral rectus muscle, SRM: Superior rectus muscle, Arrow: Fracture in the sphenoid bone, Arrowheads: Displaced inner table of the sphenoid bone, Asterisk: Broken shoji frame.
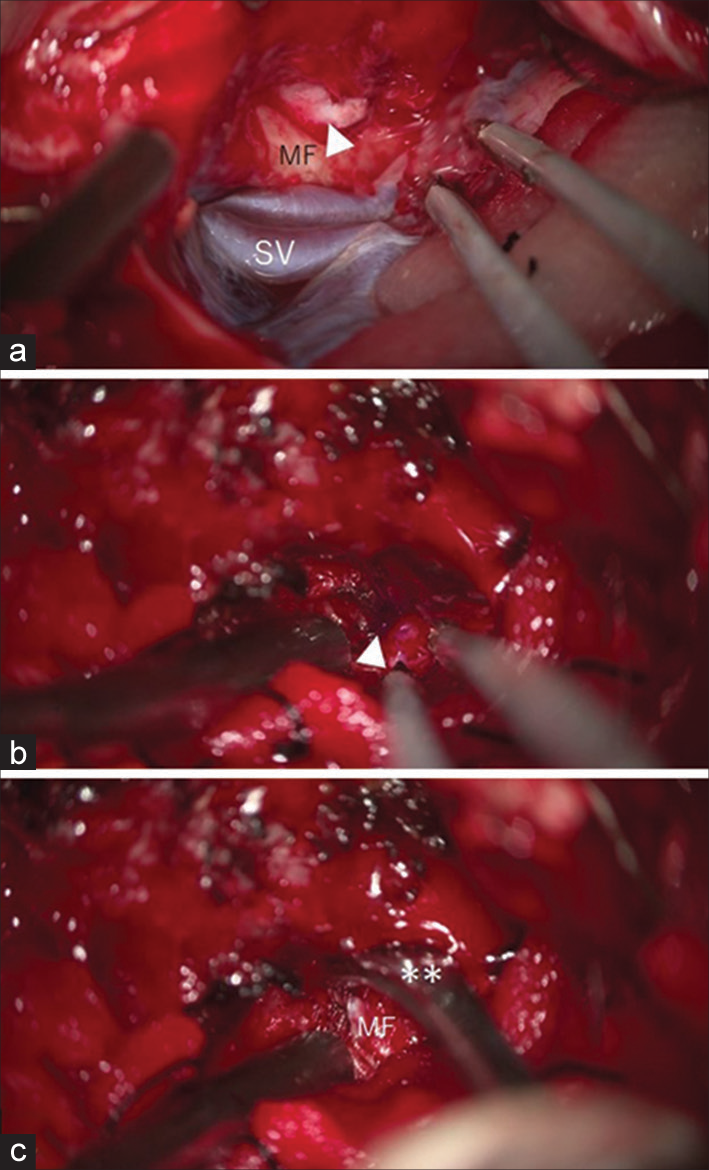
Figure 3:
Intraoperative photos present step-by-step procedures of extraction. (a) Intradural view: site of the proximal edge of broken shoji frame is identified as a localized inner protrusion of the MF dura (arrowhead). (b) Extradural view: proximal edge of the shoji frame (arrowhead) is marked with pyoktanin blue. (c) Extradural view: proximal edge of the shoji frame (arrowhead) is being pushed out from the cranial cavity using a Penfield dissector (double asterisk). SV : Sylvian vein, MF: Middle fossa.


DISCUSSION
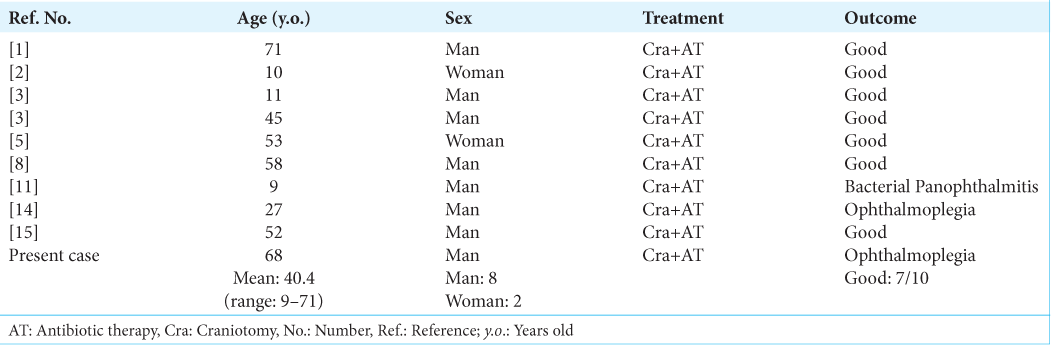
POCIs caused by wooden foreign bodies are rare. To the best of our knowledge, only ten cases including the present patient have been reported to date.[
All patients underwent a frontotemporal craniotomy or its modifications, followed by empirical antibiotic therapy. Treatment outcomes were satisfactory in seven of ten patients, while ophthalmoplegia persisted in two patients. The condition of the remaining patient was complicated by severe bacterial ophthalmitis as a result of residual foreign bodies in the orbit [
In the present case, a wooden foreign body was removed through a frontotemporal craniotomy. It was located in the upper lateral sector of the orbit, while partially protruded into the middle cranial fossa accompanied by fractures and possible dura tears. Therefore, we adopted craniotomy, instead of lateral orbitotomy, feasible for both intra-, and extradural procedures.
Wooden foreign bodies migrated in the orbital and cranial cavities have been documented to be missed on CT, indicating the diagnostic value of MRI in POCI cases.[
Broken shoji frames could be a strong weapon that can penetrate into the skull.[
CONCLUSION
POCI can be caused by a shoji frame as a result of an indoor accident. The broken shoji frame is evidently delineated on CT, which can result in prompt extraction after injury.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Avraham E, Smolikov A, Smolyakov R, Azriel A, Sufaro Y, Kaisman-Elbaz T. Minimally invasive subtemporal intradural approach for penetrating orbitocranial injury by wooden foreign body into the lateral wall of the cavernous sinus. Front Surg. 2020. 7: 533567
2. Borkar SA, Garg K, Garg M, Sharma BS. Transorbital penetrating cerebral injury caused by a wooden stick: Surgical nuances for removal of a foreign body lodged in cavernous sinus. Childs Nerv Syst. 2014. 30: 1441-4
3. Chowdhury FH, Haque MR, Hossain Z, Chowdhury NK, Alam SM, Sarker MH. Nonmissile penetrating injury to the head: Experience with 17 cases. World Neurosurg. 2016. 94: 529-43
4. Damm A, Lauritsen AØ, Klemp K, Nielsen RV. Transorbital impalement by a wooden stick in a 3-year-old child. BMJ Case Rep. 2015. 2015: bcr2015211885
5. Dunn IF, Kim DH, Rubin PA, Blinder R, Gates J, Golby AJ. Orbitocranial wooden foreign body: A pre-, intra-, and postoperative chronicle: Case report. Neurosurgery. 2009. 65: E383-4
6. Jooma R, Bradshaw JR, Coakham HB. Computed tomography in penetrating cranial injury by a wooden foreign body. Surg Neurol. 1984. 21: 236-8
7. Kapoor AG, Vijitha VS, Fernandes M. Retained intraorbital wooden foreign body presenting with combined anterior and posterior scleritis. BMJ Case Rep. 2020. 13: e232237
8. Lee JS, Lee JE, Oum BS, Cha SH. Orbitocranial injury caused by wood. Korean J Ophthalmol. 1999. 13: 128-32
9. Okura H, Takaki Y, Makino K, Nonaka S, Tsutsumi S, Ishii H. An unprecedented case of penetrating head trauma caused by shoji (a Japanese-style paper sliding door). Trauma Case Rep. 2021. 36: 100533
10. Shoji MK, Maeng MM, Tse DT. Penetrating orbital injury due to a wooden dowel in a birthday cake. JAMA Ophthalmol. 2022. 140: 544-6
11. Specht CS, Varga JH, Jalali MM, Edelstein JP. Orbitocranial wooden foreign body diagnosed by magnetic resonance imaging. Dry wood can be isodense with air and orbital fat by computed tomography. Surv Ophthalmol. 1992. 36: 341-4
12. Taş S, Top H. Intraorbital wooden foreign body: clinical analysis of 32 cases, a 10-year experience. Ulus Travma Acil Cerrahi Derg. 2014. 20: 51-5
13. Tite DJ, Batstone MD, Lynham AJ, Monsour FN, Chapman PJ. Penetrating orbital injury with wooden foreign body initially diagnosed as an orbital floor blowout fracture. ANZ J Surg. 2002. 72: 529-30
14. Wahyudi Zaky A, Islam AA, Prihantono Rosyidi RM. An extremely rare case: Transorbital penetrating intracranial injury by wooden foreign body. Case report. Ann Med Surg (Lond). 2021. 71: 102937
15. Wu Y, He W, Yang Y, Chen J. A rare case of orbitocranial penetrating injury with intracranial wooden foreign body residue. Medicine (Kaunas). 2022. 58: 1832


John B. Harris MD FACS FAANS(L)
Posted February 17, 2023, 12:55 pm
Skier arrived at our Ski area hospital with ski-pole impaled in his brain.
ski pole removed, beyond basket, effacing the skull.
CT evidence of centrum injury, half way to midline.
Emergency brain operation for extraction, and debridement of his injury tract.
Post op, alert, mild hemiparesis, alert.
Did well, in recovery.