

- Department of Obstetrics & Gynecology, AIIMS, Bhubaneshwar, Odisha, India
- Department of Neurosurgery, AIIMS, Bhubaneshwar, Odisha, India
- Department of Anesthesiology, AIIMS, Bhubaneshwar, Odisha, India
- Department of Radiology, AIIMS, Bhubaneshwar, Odisha, India
- Department of Pathology, AIIMS, Bhubaneshwar, Odisha, India
Correspondence Address:
Ashis Patnaik
Department of Pathology, AIIMS, Bhubaneshwar, Odisha, India
DOI:10.4103/sni.sni_271_17
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Singh S, Patnaik A, Sahu RN, Jena SS, Mohakud S, Purkait S. Rare case of meningeal tuberculoma mimicking meningioma in term pregnancy and its management. Surg Neurol Int 03-Sep-2018;9:178
How to cite this URL: Singh S, Patnaik A, Sahu RN, Jena SS, Mohakud S, Purkait S. Rare case of meningeal tuberculoma mimicking meningioma in term pregnancy and its management. Surg Neurol Int 03-Sep-2018;9:178. Available from: http://surgicalneurologyint.com/surgicalint-articles/8993/
Date of Submission
24-Jul-2017
Date of Acceptance
28-Feb-2018
Date of Web Publication
03-Sep-2018
Sir,
Brain tumors during pregnancy are rare. Meningiomas comprise most of them possibly due to the role of excess estrogen during pregnancy causing their growth. We present an interesting case of dural or meningeal tuberculoma resembling a meningioma both radiologically and on intra-operative findings. Literature shows few cases undergoing same stage caesarean section and excision of brain lesion.[
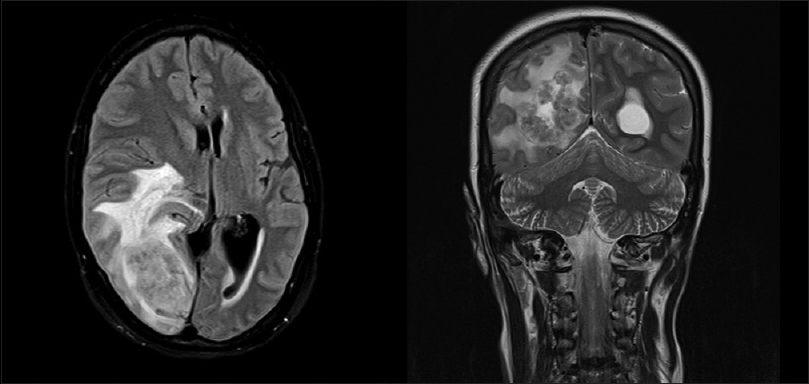
A 31-year-old woman, gravida 3 para 1 with one previous abortion, at 37 weeks and 4 days of gestation, presented in emergency hours with complaints of blurring of vision for 15 days and headache with vomiting for the past 12 h. She had irregular antenatal check-ups. Her first pregnancy was 5 years back and was a full-term normal institutional delivery. Her second pregnancy 2 years back resulted in a medication abortion at 6 weeks, and this was her third pregnancy. She had availed of three antenatal check-ups in this pregnancy. She was treated at her local hospital for vomiting in pregnancy for the past 12 h with intravenous fluids and antacids. Her previous menstrual cycles were regular with average flow. Her past and family history were not significant. On examination, she was conscious, oriented with Glasgow Coma Scale (GCS) of 15. Her vitals were stable. Thyroid, respiratory, and cardiovascular system examinations were normal. On abdominal examination, uterus was term in size, relaxed, with a live singleton fetus in longitudinal lie and cephalic presentation, vertex being mobile. Patient was managed conservatively with intravenous fluids, antiemetics, and proton pump inhibitor. However, as there was no symptomatic improvement for blurring of vision, fundoscopy was done which showed mild disc edema. Magnetic resonance imaging (MRI) of brain was done, which showed a T2 heterogeneous and FLAIR hyperintense lesion of size 4.0 × 3.7 × 3.5 cm in the right occipital lobe, with gross edema in the occipito-parietal lobe with mass effect and contralateral midline shift by 11.7 mm [

Neurosurgical disorders during pregnancy are rare and pose risk to two lives and create special diagnostic and therapeutic challenges. Tumors, intracranial hemorrhage due to arteriovenous malformations (AVMs), aneurysms, and intracranial bleeding due to eclampsia, hydrocephalus, and trauma are the most common lesions seen during pregnancy period.[
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Aggarwal A, Patra DP, Gupta K, Sodhi HB. Dural Tuberculoma Mimicking Meningioma: A Clinicoradiologic Review of Dural En-Plaque Lesions. World Neurosurg. 2016. 88: 686-
2. DeAngelis LM. Central nervous system neoplasms in pregnancy. Adv Neurol. 1994. 64: 139-52
3. Dias MS, Sekhar LN. Intracranial hemorrhage from aneurysms and arteriovenous malformations during pregnancy and the puerperium. Neurosurgery. 1990. 27: 855-6
4. Khurana T, Taneja B, Saxena KN. Anesthetic management of a parturient with glioma brain for cesarean section immediately followed by craniotomy. J Anaesthesiol Clin Pharmacol. 2014. 30: 397-9
5. Lindner A, Schneider C, Hofmann E, Soerensen N, Toyka KV. Isolated meningeal tuberculoma mimicking meningioma: Case report. Surg Neurol. 1995. 43: 81-3
6. Shindo A, Honda C, Baba Y. A case of an intracranial tuberculoma, mimicking meningioma that developed during treatment with anti-tuberculous agents. No Shinkei Geka. 1999. 27: 837-41
7. Shiota N, Satomoto M, Hakusui T, Nakazawa K, Makita K. Anesthetic management of a pregnant woman with brain tumor. Masui. 2014. 63: 1142-5

