

- Department of Neurosurgery, Jessa Hospital Hasselt, Hasselt, Belgium.
DOI:10.25259/SNI_163_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Sven Bamps, Gert Roosen, Eric Put, Mark Plazier, Steven Vanvolsem, Maarten Wissels, Peter Donkersloot, Wim Duyvendak. Retro-odontoid pseudotumor (pannus) with Forestier’s disease presenting with severe tetraparesis: A case report and literature review. 16-May-2020;11:111
How to cite this URL: Sven Bamps, Gert Roosen, Eric Put, Mark Plazier, Steven Vanvolsem, Maarten Wissels, Peter Donkersloot, Wim Duyvendak. Retro-odontoid pseudotumor (pannus) with Forestier’s disease presenting with severe tetraparesis: A case report and literature review. 16-May-2020;11:111. Available from: https://surgicalneurologyint.com/surgicalint-articles/10027/
Date of Submission
07-Apr-2020
Date of Acceptance
21-Apr-2020
Date of Web Publication
16-May-2020
Abstract
Background: A retro-odontoid pannus is often associated with inflammatory diseases. It can also have a noninflammatory cause due to chronic atlantoaxial instability.
Case Description: Here, we report a patient with diffuse idiopathic skeletal hyperostosis and a severe noninflammatory retro-odontoid pannus who rapidly improved after posterior craniocervical decompression and arthrodesis.
Conclusion: Transoral resection of the pannus, followed by posterior stabilization, is a common treatment for this condition. The pannus can, however, also reduce after posterior stabilization alone (e.g., craniocervical decompression).
Keywords: Craniocervical – Posterior stabilization, Decompression, Pannus
INTRODUCTION
The retro-odontoid pseudotumor or pannus is often associated with inflammatory diseases.[
Typically, these lesions are treated utilizing combined transoral resection of the pannus, followed by posterior stabilization.[
Here, we present a 79-year-old male and reviewed the literature documenting that diffuse idiopathic skeletal progressive tetraparesis attributed to a noninflammatory retro-odontoid pannus rapidly improved following posterior decompression/fusion alone.
CASE REPORT
History
A 79-year-old male presented with the acute onset of severe tetraparesis following minor trauma. The neurological examination showed a left hemiplegia (MRC 2/5) with the right-sided neurological weakness without sensory abnormalities. The Preoperative Nurick Grade was V.
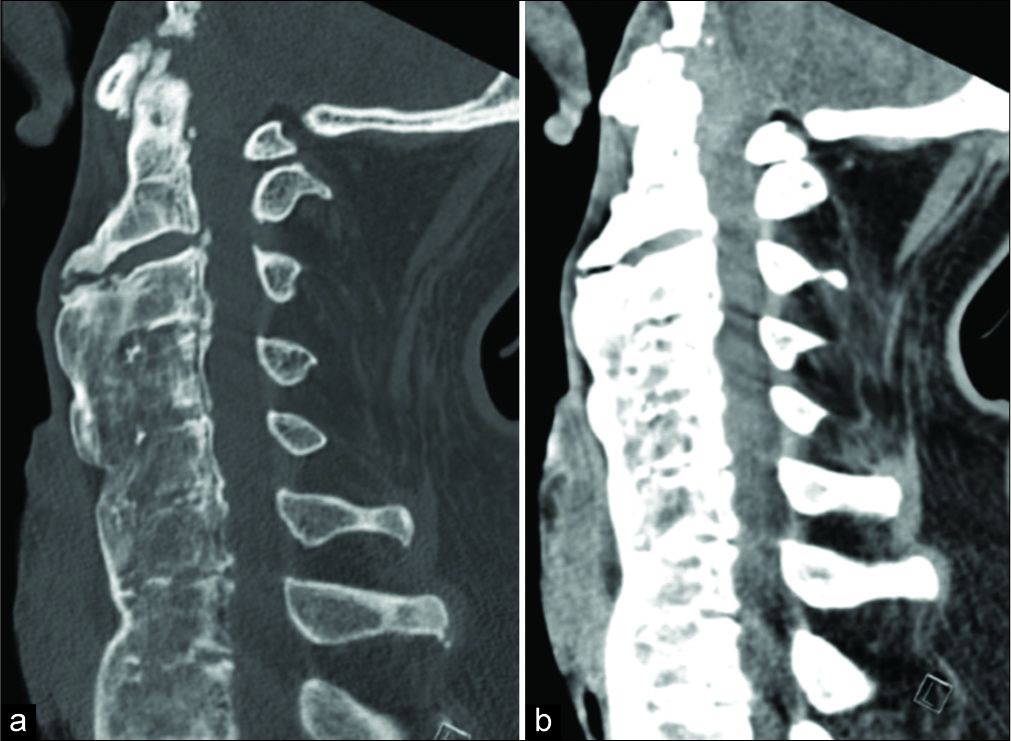
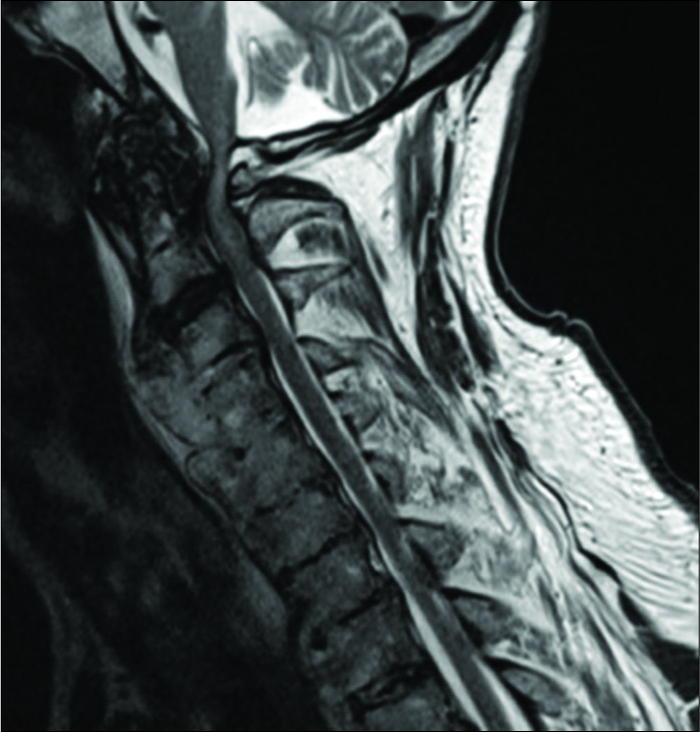
The CT [
Surgery
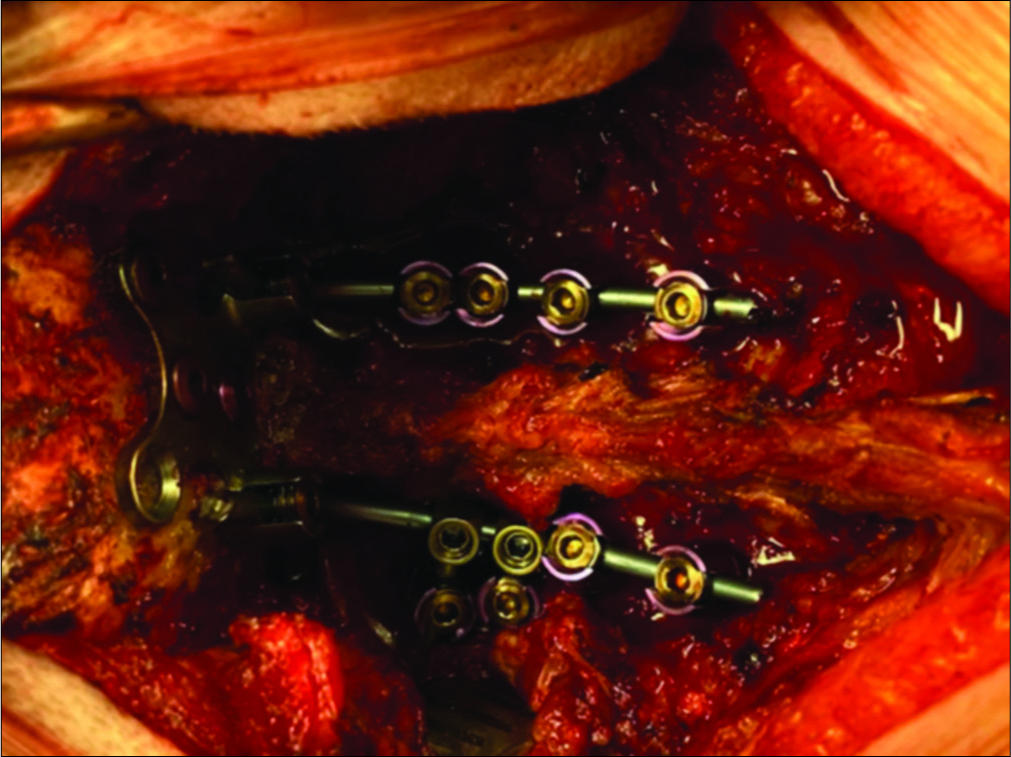
The patient underwent an urgent posterior C0–C5 arthrodesis with C1 and C2 laminectomy and bilateral lateral mass screws at C1, C3, C4, and C5 levels and with bilateral pars screws at C2 [
The postoperative course was uneventful and the neurological symptoms improved rapidly with normalization of strength in the right arm and leg and a clear improvement in the left arm and leg (MRC 4/5). Within 3 weeks, he was able to walk independently (i.e. Nurick Grade II).
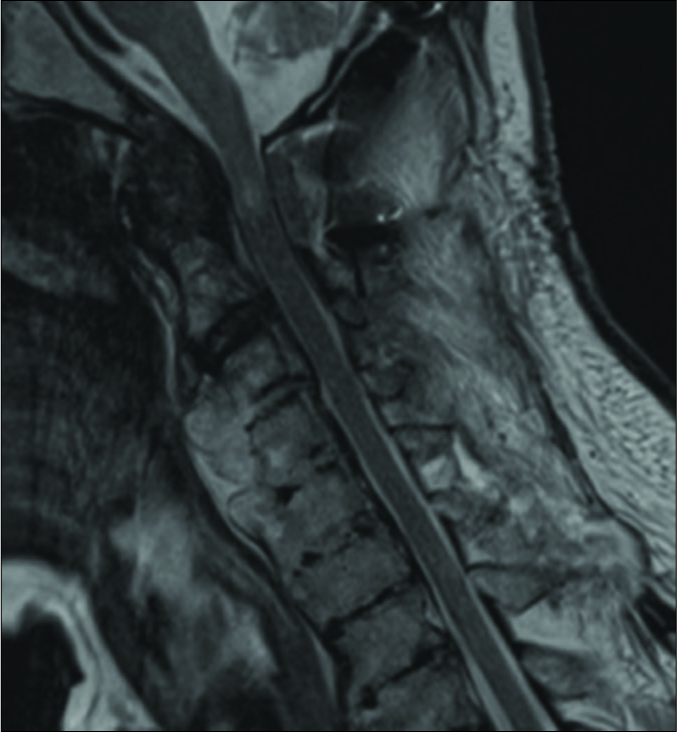
Postoperative imaging [
DISCUSSION
Retro-odontoid pseudotumors have also been reported in noninflammatory conditions such as post- traumatic pseudoarthrosis of the odontoid process, unstable odontoid fractures, os odontoideum, cervical instability, long-term hemodialysis, and craniocervical malformations.
To date, transoral spinal cord decompression followed by posterior stabilization has been a widely accepted treatment. In the past years, however, several authors have reported a pannus reduction and even regression after a posterior atlantoaxial stabilization only.[
Here, we describe a 79-year-old male who experienced a rapidly progressive tetraparesis due to a retro-odontoid pannus with diffuse idiopathic skeletal hyperostosis/ ankylosis (Forestier disease) in combination with a fracture of the anterior syndesmophytes at the C2–C3 level.
The patient underwent an urgent C1 and C2 laminectomy with posterior stabilization alone (e.g., C0–C5 fusion). Postoperatively, he rapidly improved documenting that posterior management alone may be sufficient in these patients.[
CONCLUSION
Craniocervical decompression and posterior stabilization resulted in pannus reduction and neurological improvement in a 79-year-old male.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Barbagallo G, Certo F, Visocchi M, Palmucci S, Sciacca G, Albanese V. Disappearance of degenerative, non-inflammatory, retro-odontoid pseudotumor following posterior C1-C2 fixation: Case series and review of the literature. Eur Spine J. 2013. 22: S879-88
2. Chikuda H, Seichi A, Takeshita K, Shoda N, Ono T, Matsudaira K. Radiographic analysis of the cervical spine in patients with retro-odontoid pseudotumors. Spine. 2009. 34: E110-4
3. Isono M, Ishii K, Kamida T, Fujiki M, Goda M, Kobayashi H. Retro-odontoid soft tissue mass associated with atlantoaxial subluxation in an elderly patient: A case report. Surg Neurol. 2001. 55: 223-7
4. Lagares A, Arrese I, Pascual B, Gomez P, Ramos A, Lobato R. Pannus resolution after occipitocervical fusion in a non-rheumatoid atlanto-axial instability. Eur Spine J. 2006. 15: 366-9
5. Suetsuna F, Narita H, Ono A, Ohishi H. Regression of retroodontoid pseudotumors following C1 laminoplasty. J Neurosurg Spine. 2006. 5: 455-60
6. Yamaguchi I, Shibuya S, Arima N, Oka S, Kanda Y, Yamamoto T. Remarkable reduction or disappearance of retroodontoid pseudotumors after occipitocervical fusion. Report of three cases. J Neurosurg Spine. 2006. 5: 156-60

