

- Department of Neurosurgery, Perelman School of Medicine, Hospital of the University of Pennsylvania, Philadelphia, Pennsylvania, USA
- Center for Neuroengineering and Therapeutics, University of Pennsylvania, Philadelphia, Pennsylvania, USA
Correspondence Address:
Kalil G. Abdullah
Department of Neurosurgery, Perelman School of Medicine, Hospital of the University of Pennsylvania, Philadelphia, Pennsylvania, USA
Center for Neuroengineering and Therapeutics, University of Pennsylvania, Philadelphia, Pennsylvania, USA
DOI:10.4103/2152-7806.195227
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Kalil G. Abdullah, H. Isaac Chen, Timothy H. Lucas. Safety of topical vancomycin powder in neurosurgery. 05-Dec-2016;7:
How to cite this URL: Kalil G. Abdullah, H. Isaac Chen, Timothy H. Lucas. Safety of topical vancomycin powder in neurosurgery. 05-Dec-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/safety-of-topical-vancomycin-powder-in-neurosurgery/
Date of Submission
02-Feb-2016
Date of Acceptance
28-Mar-2016
Date of Web Publication
05-Dec-2016
Abstract
Surgical site infections (SSIs) remain an important cause of morbidity following neurosurgical procedures despite the best medical practices. In addition, hospital infection rates are proposed as a metric for ranking hospitals safety profiles to guide medical consumerism. Recently, the use of topical vancomycin, defined as the application of vancomycin powder directly into the surgical wound, has been described in both cranial and spinal surgeries as a method to reduce SSIs. Early results are promising. Here, we provide a concise primer on the pharmacology, bacterial spectrum, history, and clinical indications of topical vancomycin for the practicing surgeon.
Keywords: Cranial infection, spine infection, surgical site infection, vancomycin powder
INTRODUCTION
Surgical site infections (SSIs) adversely affect patients, providers, and hospitals. Despite the best practices of perioperative systemic antibiotics and sterile technique, SSIs persist. These adverse events, even in relatively low “acceptable” percentages, constitute a significant burden to clinical practice.
Beyond the obvious adverse consequences for patients and providers, SSIs are associated with significant cost and have been proposed as a metric to rank hospitals. These “safety rating” schemes pit hospitals and practices against one another without the benefit of contextual information, such as practice mix, patient demographics, and complexity of care.
It is incumbent upon practicing clinicians to reduce the incidence of SSI to the greatest extent possible. Further, surgeons must also be ready to counsel discerning patients who are increasingly savvy to the issue of hospital-acquired infections and SSI during preoperative visits. A growing body of literature surrounds the use of topical antibiotic administration as a surgical adjunct to reduce SSI. Topical vancomycin has been examined in spine and, now recently, in cranial surgery. In this review, we summarize the pharmacology, bacterial spectrum, indications, and safety of topical vancomycin for practicing neurosurgeons.
BASIC PHARMACOLOGY AND CLINICAL USE
The compound, now known as vancomycin, was first isolated by Eli Lilly in soil samples collected from Borneo in 1953.[
Resistance to vancomycin among enterococci colonies was first reported in the mid-1980s, with strains of S. aureus reported as either resistant (e.g., vancomycin-resistant S. aureus [VRSA]) or intermediately susceptible to vancomycin (e.g. vancomycin intermediate S. aureus [VISA]) in the late 1990s.[
Specific guidelines for vancomycin use are hospital-specific and tailored to the antibiotic spectrum and susceptibilities of the local patient population by hospital infection control programs. The Centers for Disease Control (CDC) provides guidance for the prevention of healthcare-associated infections (including SSI).[
Vancomycin has not received widespread adoption as a first-line treatment for infections despite its efficacy. This is due, in part, to the fact that has very poor bioavailability. No appreciable absorption occurs through the gastrointestinal system following oral administration. This aids in the treatment of Clostridium difficile infections which are sequestered in the gut. All other infections, however, require parenteral administration. Following infusion, the half-life of the drug is tri-exponential: The half-lives of the initial phase, second phase, and terminal phase are 7 min, 0.5–1 h, and 3–9 h, respectively.[
Neurosurgeons encounter patients with infections within the cerebrospinal fluid (CSF). Vancomycin levels within the CSF levels are highly variable following parenteral administration. In general, they peak at <30% of the serum concentration. Accordingly, treating CSF-based infections requires higher systemic dosing.[
Systemic toxicity
The available toxicity data of this drug are primarily related to end-organ effects following parenteral administration. Vancomycin is well tolerated with appropriate dosing. The overall incidence of side effects is approximately 10%.[
Management consists of discontinuation of the drug and administration of antihistamines, systemic steroids, intravenous fluids, and epinephrine as needed. More gradual administration of the drug over an hour may reduce to likelihood of red man syndrome. More common side effects include thrombophlebitis, fever, rash, and reversible neutropenia.[
Otoxocity and nephrotoxicity are considered more serious, but rare, complications of vancomycin use. In limited studies, these hair cells appear to be sensitive to vancomycin. A study of vancomycin ear droplets showed an association between direct application of the compound and increased thresholds for high-frequency auditory detection.[
In both instances of end-organ damage, hair cells and renal glomeruli, host susceptibility appears to be a factor. Older patients predisposed to high-frequency hearing loss are most susceptible to vancomycin-related ototoxicity, and patients with preexisting renal dysfunction or concurrent nephrotoxic medications are most susceptible to further renal injury.[
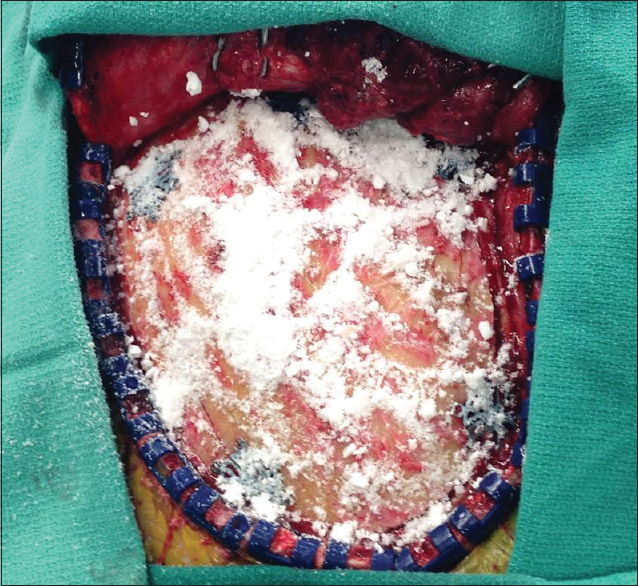
TOPICAL APPLICATION OF VANCOMYCIN
Historical precedent
The concept of direct application of antibiotics to surgical wounds has a long history. Over 60 years ago, surgeons experimented with antibiotic irrigation as a means to cleans the wound. Subsequent decades witnessed significant decreases in SSIs with the routine application of antibiotic irrigation, laying the historical foundation for the modern practice of antibiotic irrigation in most operating rooms.[
In its current formulation, topical vancomycin was first used in 1989 by cardiac surgeons applying the drug to the cut bone edges after sternotomy. In a randomized, controlled investigation, topical vancomycin significantly reduced infections when compared to a hemostatic placebo.[
The use of topical vancomycin has only recently been extended to cranial surgery.[
These findings have motivated a prospective randomized controlled trial on cranial vancomycin use to provide Class I evidence on the matter.
Vancomycin powder - physical properties
In crystalized form, vancomycin exists as vancomycin hydrochloride. This “powder” is supplied by pharmaceutical companies in a sterile vile and has the consistency of household baking soda [
Cost is an important consideration. A 1 g vial of vancomycin hydrochloride has a direct cost between $2 and $12 for most institutions.[
SAFETY CONSIDERATIONS
Local side effects following topical administration
Vancomycin is crystallized as a salt with hydrochloride. This preparation results in hydrogen ion disassociation in solution. When mixed with interstitial fluid or saline, the resultant pH varies with the volume of solution. Accordingly, wound pH has been monitored in a number of studies using wound drains to measure fluid acidity.[
Parental administration of vancomycin is associated with phlebitis at a rate of 0–18%.[
No direct adverse effects of vancomycin were noted in the only published study in cranial surgery.[
Systemic side effects following topical administration
Systemic effects of topical vancomycin application have been most extensively studied in spinal surgery. Of the >2000 of vancomycin administration during spine surgery in the past several years, only two complications directly attributable to vancomycin application were reported, to the best of our knowledge.
These isolated case reports failed to meet inclusion criteria for the meta-analysis cited above and were therefore not included. Mariappan et al.[
Peripheral levels of vancomycin and antibiotic resistance
The use of antibiotics carries the incumbent risk of antibiotic resistance. Vancomycin-resistant strains of Enterococcus, for example, may colonize the intestine. For this reason, CDC generally advises against the routine use of vancomycin in irrigation solutions. To examine whether vancomycin penetrates the systemic circulation following topical application, serum levels of vancomycin have been measured. Following cranial application of 1 g in adults, serum vancomycin levels remain undetectable at numerous time points following surgery.[
Naturally, the question of antibiotic resistance must be considered when introducing additional prophylactic antibiotic exposure. Data on antibiotic resistance to vancomycin suggest that overuse of vancomycin alone does not breed vancomycin resistance. Vancomycin-resistant strains (VRSA) have been found only to occur in the presence of a coinfection of enterococci.[
The available evidence suggests that topical vancomycin significantly reduces the incidence of SSIs. Due to the peptide's selective action against Gram-positive cell wall assembly, one might logically hypothesize that the Gram-negative bacterial flora would account for a higher proportion of subsequent SSIs. While this question has not been rigorously examined in a prospective trial, Ghobrial et al.[
CONCLUSIONS
Vancomycin is a well-established antibiotic against Gram-positive bacterial strains. Its use in spine surgery, and recently cranial surgery, provide convincing evidence that vancomycin is safe in neurosurgical procedures. SSIs are reduced when it is applied in addition to standard antibiotic prophylaxis. Known side effects associated with parenteral administration do not appear to occur when the drug is applied topically into a surgical wound. There is insufficient evidence to suggest that routine single-use vancomycin powder leads to antibiotic resistance. Routine use of vancomycin powder as a surgical adjunct is supported by the available literature and warrants further examination in randomized controlled trials.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Abdullah KG, Attiah MA, Olsen AS, Richardson A, Lucas TH. Reducing surgical site infections following craniotomy: Examination of the use of topical vancomycin. J Neurosurg. 2015. 123: 1600-4
2. Aoki FY.editors. Principles of antimicrobial therapy and the clinical pharmacology of antimicrobial drugs. Principles of Critical Care. New York: The McGraw-Hill Companies; 2005. p.
3. Armaghani SJ, Menge TJ, Lovejoy SA, Mencio GA, Martus JE. Safety of topical vancomycin for pediatric spinal deformity: Nontoxic serum levels with supratherapeutic drain levels. Spine (Phila Pa 1976). 2014. 39: 1683-7
4. Bakhsheshian J, Dahdaleh NS, Lam SK, Savage JW, Smith ZA. The use of vancomycin powder in modern spine surgery: Systematic review and meta-analysis of the clinical evidence. World Neurosurg. 2015. 83: 816-23
5. . Beckman Coulter Incorporated: Emit 2000 vancomycin assay. OSR4W229. 2010. p.
6. Bibbo C, Patel DV. The effect of demineralized bone matrix-calcium sulfate with vancomycin on calcaneal fracture healing and infection rates: A prospective study. Foot Ankle Int. 2006. 27: 487-93
7. Black FO, Gianna-Poulin C, Pesznecker SC. Recovery from vestibular ototoxicity. Otol Neurotol. 2001. 22: 662-71
8. Caparas JV, Hu JP. Safe administration of vancomycin through a novel midline catheter: A randomized, prospective clinical trial. J Vasc Access. 2014. 15: 251-6
9. Caroom C, Tullar JM, Benton EG, Jones JR, Chaput CD. Intrawound vancomycin powder reduces surgical site infections in posterior cervical fusion. Spine (Phila Pa 1976). 2013. 38: 1183-7
10. Last accessed on 2014 Dec 11. Available from: http://www.cdc.gov/HAI/prevent/top-cdc-recs-prevent-hai.html.
11. Chen K, Wu Y, Wang Q, Wang J, Li X, Zhao Z. The methodology and pharmacokinetics study of intraventricular administration of vancomycin in patients with intracranial infections after craniotomy. J Crit Care. 2015. 30: 218.e1-5
12. Cui L, Ma X, Sato K, Okuma K, Tenover FC, Mamizuka EM. Cell wall thickening is a common feature of vancomycin resistance in Staphylococcus aureus. J Clin Microbiol. 2003. 41: 5-14
13. Deck DH, Winston LG.editors. Beta-lactam & other cell wall & membrane-active antibiotics. Basic and Clinical Pharmacology. New York: The McGraw-Hill Companies; 2012. p.
14. Desmond J, Lovering A, Harle C, Djorevic T, Millner R. Topical vancomycin applied on closure of the sternotomy wound does not prevent high levels of systemic vancomycin. Eur J Cardiothorac Surg. 2003. 23: 765-70
15. Drouet M, Chai F, Barthélémy C, Lebuffe G, Debaene B, Décaudin B. Influence of vancomycin infusion methods on endothelial cell toxicity. Antimicrob Agents Chemother. 2015. 59: 930-4
16. Emohare O, Ledonio CG, Hill BW, Davis RA, Polly DW, Kang MM. Cost savings analysis of intrawound vancomycin powder in posterior spinal surgery. Spine J. 2014. 14: 2710-5
17. Ghobrial GM, Thakkar V, Andrews E, Lang M, Chitale A, Oppenlander ME. Intraoperative vancomycin use in spinal surgery: Single institution experience and microbial trends. Spine (Phila Pa 1976). 2014. 39: 550-5
18. Ghobrial GM, Thakkar V, Singhal S, Oppenlander ME, Maulucci CM, Harrop JS. Efficacy of intraoperative vancomycin powder use in intrathecal baclofen pump implantation procedures: Single institutional series in a high risk population. J Clin Neurosci. 2014. 21: 1786-9
19. Gibson RM. Application of antibiotics (polybactrin) in surgical practice, using the aerosol technique. Br Med J. 1958. 1: 1326-7
20. Godil SS, Parker SL, O’Neill KR, Devin CJ, McGirt MJ. Comparative effectiveness and cost-benefit analysis of local application of vancomycin powder in posterior spinal fusion for spine trauma: Clinical article. J Neurosurg Spine. 2013. 19: 331-5
21. Guglielmo BJ, Papadakis MA, McPhee SJ.editors. Anti-infective chemotherapeutic & antibiotic agents. CURRENT Medical Diagnosis and Treatment. New York: The McGraw-Hill Companies; 2014. p.
22. Halasz NA. Wound infection and topical antibiotics: The surgeon's dilemma. Arch Surg. 1977. 112: 1240-4
23. Hayakawa K, Marchaim D, Vidaillac C, Lephart P, Pogue JM, Sunkara B. Growing prevalence of vancomycin-resistant Enterococcus faecalis in the region with the highest prevalence of vancomycin-resistant Staphylococcus aureus. Infect Control Hosp Epidemiol. 2011. 32: 922-4
24. Howden BP, Davies JK, Johnson PD, Stinear TP, Grayson ML. Reduced vancomycin susceptibility in Staphylococcus aureus, including vancomycin-intermediate and heterogeneous vancomycin-intermediate strains: Resistance mechanisms, laboratory detection, and clinical implications. Clin Microbiol Rev. 2010. 23: 99-139
25. Khan NR, Thompson CJ, DeCuypere M, Angotti JM, Kalobwe E, Muhlbauer MS. A meta-analysis of spinal surgical site infection and vancomycin powder. J Neurosurg Spine. 2014. 21: 974-83
26. Kim HS, Lee SG, Kim WK, Park CW, Son S. Prophylactic intrawound application of vancomycin powder in instrumented spinal fusion surgery. Korean J Spine. 2013. 10: 121-5
27. Kim HW, Knowles JC, Kim HE. Hydroxyapatite porous scaffold engineered with biological polymer hybrid coating for antibiotic Vancomycin release. J Mater Sci Mater Med. 2005. 16: 189-95
28. Klekamp J, Dawson JM, Haas DW, DeBoer D, Christie M. The use of vancomycin and tobramycin in acrylic bone cement: Biomechanical effects and elution kinetics for use in joint arthroplasty. J Arthroplasty. 1999. 14: 339-46
29. Kluytmans J, van Belkum A, Verbrugh H. Nasal carriage of Staphylococcus aureus: Epidemiology, underlying mechanisms, and associated risks. Clin Microbiol Rev. 1997. 10: 505-20
30. Lanbeck P, Odenholt I, Paulsen O. Antibiotics differ in their tendency to cause infusion phlebitis: A prospective observational study. Scand J Infect Dis. 2002. 34: 512-9
31. Levine DP. Vancomycin: A history. Clin Infect Dis. 2006. 42: S5-12
32. Levinson W.editors. Antimicrobial drugs: Mechanism of action. Review of Medical Microbiology and Immunology. New York: The McGraw-Hill Companies; 2012. p.
33. Lilikakis A, Sutcliffe MP. The effect of vancomycin addition to the compression strength of antibiotic-loaded bone cements. Int Orthop. 2009. 33: 815-9
34. Mariappan R, Manninen P, Massicotte EM, Bhatia A. Circulatory collapse after topical application of vancomycin powder during spine surgery. J Neurosurg Spine. 2013. 19: 381-3
35. Matzke GR, Zhanel GG, Guay DR. Clinical pharmacokinetics of vancomycin. Clin Pharmacokinet. 1986. 11: 257-82
36. Ng K, Mabasa VH, Chow I, Ensom MH. Systematic review of efficacy, pharmacokinetics, and administration of intraventricular vancomycin in adults. Neurocrit Care. 2014. 20: 158-71
37. Olyaei AJ, Bennett WM.editors. Acute renal failure from therapeutic agents. Current Diagnosis and Treatment: Nephrology and Hypertension. New York: The McGraw-Hill Companies; 2009. p.
38. Ozcan AV, Demir M, Onem G, Goksin I, Baltalarli A, Topkara VK. Topical versus systemic vancomycin for deep sternal wound infection caused by methicillin-resistant Staphylococcus aureus in a rodent experimental model. Tex Heart Inst J. 2006. 33: 107-10
39. Rubinstein E, Keynan Y. Vancomycin revisited – 60 years later. Front Public Health. 2014. 2: 217-
40. Rybak M, Lomaestro B, Rotschafer JC, Moellering R, Craig W, Billeter M. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm. 2009. 66: 82-98
41. Sakaguchi H, Marui A, Hirose K, Nomura T, Arai Y, Bir SC. Less-invasive and highly effective method for preventing methicillin-resistant Staphylococcus aureus graft infection by local sustained release of vancomycin. J Thorac Cardiovasc Surg. 2008. 135: 25-31
42. Stierman BLast accessed on 2014 Dec 11. Available from: http://www.clinicalcorrelations.org/?p=5810.
43. Sweet FA, Roh M, Sliva C. Intrawound application of vancomycin for prophylaxis in instrumented thoracolumbar fusions: Efficacy, drug levels, and patient outcomes. Spine (Phila Pa 1976). 2011. 36: 2084-8
44. Tange RA, Kieviet HL, von Marle J, Bagger-Sjöbäck D, Ring W. An experimental study of vancomycin-induced cochlear damage. Arch Otorhinolaryngol. 1989. 246: 67-70
45. Urabe K, Naruse K, Hattori H, Hirano M, Uchida K, Onuma K. In vitro comparison of elution characteristics of vancomycin from calcium phosphate cement and polymethylmethacrylate. J Orthop Sci. 2009. 14: 784-93
46. Vander Salm TJ, Okike ON, Pasque MK, Pezzella AT, Lew R, Traina V. Reduction of sternal infection by application of topical vancomycin. J Thorac Cardiovasc Surg. 1989. 98: 618-22
47. Youssef JA, Orndorff DG, Scott MA, Ebner RE, Knewitz AP. Sterile seroma resulting from multilevel XLIF procedure as possible adverse effect of prophylactic vancomycin powder: A case report. Evid Based Spine Care J. 2014. 5: 127-33
Commentary
Alexander Ksendzovsky, I. Jonathan Pomeraniec, Justin S. Smith- label>1Surgical Neurology Branch, National Institute of Neurological Disorders and Stroke, National Institutes of Health, Bethesda, MD, USA
- label>2Department of Neurological Surgery, University of Virginia Health Sciences Center, Charlottesville, Virginia, USA E-mail:
ksendzovskya@ninds.nih.gov
TOPICAL VANCOMYCIN IN NEUROSURGERY
The authors present a review on the topical use of vancomycin. They discuss its pharmacology and pharmacokinetics along with associated toxicity. This report makes a special note of the historical underpinnings of vancomycin in the operating room and major trials in neurological surgery. Given a recent increased trend in topical vancomcyin use for surgical site infection (SSI) prophylaxis, this is an important topic to critically review.
As discussed in the current review, SSI remains a significant burden on patients, hospitals, and the broader healthcare system. In a recent prospective multicenter trial, the International Spine Study Group reviewed postoperative complications in adult deformity surgery over a two year period. In this cohort, 6% of 291 patients experienced deep wound SSIs.[
SSI reduction may not only produce cost savings but also has growing implications for reimbursement. Recently, the Center for Medicare and Medicaid Services introduced Hospital-Acquired Condition Reduction and Hospital Value-Based Purchasing Programs. These initiatives link reimbursement rates to quality measures in an attempt to improve patient outcomes. In both programs, infection reduction is a direct quality indicator, and hence directly dictates reimbursement.[
Despite this apparent need for reduction of infection rates, a consensus among neurosurgeons regarding vancomycin is still lacking. Topical vancomycin use has been examined in over 20 reported studies to date, most of which are in the spine literature.[
Similarly, there is a trend toward cost-reduction with vancomycin use. In 2014, Theologis et al. retrospectively reviewed the cost of SSI in adult deformity reconstruction surgery with and without the use of vancomycin. Out of 250 patients, there was significant reduction in 90-day hospital readmissions (2.6% vs. 10.9%) and an overall reduced cost of $244,402 per 100 spinal deformity cases.[
Even though the prospect of vancomycin use is encouraging, there are several barriers to widespread adoption. These barriers include lack of clarity regarding optimal dosage, lack of application guidelines, and the largely retrospective nature of the available data. More prospective data from appropriately designed clinical trials with consistent practice guidelines will help to further elucidate the role of vancomycin in neurosurgical practice.
References
1. Abdullah KG, Attiah MA, Olsen AS, Richardson A, Lucas TH. Reducing surgical site infections following craniotomy: Examination of the use of topical vancomycin. J Neurosurg. 2015. 123: 1600-4
2. Last accessed on 2016 Apr 11. https://www.cms.gov/medicare/medicare-fee-for-service-payment/physicianfeedbackprogram/valuebasedpaymentmodifier.html#Quality%20and%20Cost%20Measures%20Used%20in%20the%20Value%20Modifier.
3. Chiang HY, Kamath AS, Pottinger JM, Greenlee JD, Howard MA, Cavanaugh JE. Risk factors and outcomes associated with surgical site infections after craniotomy or craniectomy. Journal Neurosurg. 2014. 120: 509-21
4. Emohare O, Ledonio CG, Hill BW, Davis RA, Polly DW, Kangz MM. Cost savings analysis of intrawound vancomycin powder in posterior spinal surgery. Spine J. 2014. 14: 2710-5
5. Kang DG, Holekamp TF, Wagner SC, Lehman RA. Intrasite vancomycin powder for the prevention of surgical site infection in spine surgery: A systematic literature review. Spine J. 2015. 15: 762-70
6. Smith JS, Klineberg E, Lafage V, Shaffrey CI, Schwab F, Lafage R. Prospective multicenter assessment of perioperative and minimum 2-year postoperative complication rates associated with adult spinal deformity surgery. J Neurosurg Spine. 2016. p. 1-14
7. Theologis AA, Demirkiran G, Callahan M, Pekmezci M, Ames C, Deviren V. Local intrawound vancomycin powder decreases the risk of surgical site infections in complex adult deformity reconstruction: A cost analysis. Spine (Phila Pa 1976). 2014. 39: 1875-80
8. Tubaki VR, Rajasekaran S, Shetty AP. Effects of using intravenous antibiotic only versus local intrawound vancomycin antibiotic powder application in addition to intravenous antibiotics on postoperative infection in spine surgery in 907 patients. Spine (Phila Pa 1976). 2013. 38: 2149-55

