

- Department of Surgery, Section of Neurosurgery, The Aga Khan University Hospital, Karachi, Pakistan
Correspondence Address:
Syed Ather Enam
Department of Surgery, Section of Neurosurgery, The Aga Khan University Hospital, Karachi, Pakistan
DOI:10.4103/sni.sni_160_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Muhammad Waqas, Inamullah Khan, Reehana Khawaja, Ayesha Quddusi, Syed Ather Enam. Self-resolving prepontine cyst. 06-Sep-2017;8:215
How to cite this URL: Muhammad Waqas, Inamullah Khan, Reehana Khawaja, Ayesha Quddusi, Syed Ather Enam. Self-resolving prepontine cyst. 06-Sep-2017;8:215. Available from: http://surgicalneurologyint.com/surgicalint-articles/self%e2%80%91resolving-prepontine-cyst/
Date of Submission
24-Apr-2017
Date of Acceptance
06-Jul-2017
Date of Web Publication
06-Sep-2017
Abstract
Background:Intracranial prepontine cysts are rare and include epidermoid cysts, arachnoid cysts, and neurenteric cysts. Symptomatic prepontine cysts may require surgical intervention. Reports of spontaneous resolution of cysts are rare.
Case Description:We describe the case of a young gentleman who presented with headache and fever. Magnetic resonance imaging of the brain identified a prepontine lesion with features consistent with epidermoid cyst. During admission, the patient received symptomatic management in addition to empirical antibiotic therapy and dexamethasone. The patient improved symptomatically in the next 48 hours and was discharged. Follow-up imaging at 6 months and 1 year showed significant reduction in size of the lesion.
Conclusion:For asymptomatic prepontine cysts, a close radiological and clinical follow-up may prove useful.
Keywords: Adult brain cyst, MRI brain, prepotine cyst, self-resolution
INTRODUCTION
Prepontine cystic lesions are rare. Common types of cysts reported in this area include epidermoid cysts, arachnoid cysts, and neurenteric cysts.[
In this report, we describe the case of a young gentleman who presented with headache and fever. A large prepontine cyst was found on magnetic resonance imaging (MRI) with features consistent with epidermoid cyst. The possibility of neurenteric could not be excluded. Patient was treated symptomatically. Follow-up MRI at 1 year showed significant reduction in the size of the cyst.
CASE REPORT
A 41-year-old, right-handed gentleman presented to us in the emergency room with history of severe occipital headache for 4 days. It was constant and moderate to severe in intensity. There was no association with daytime or cough. Headache was associated with several episodes of vomiting. There were no mental status changes, seizure, or complain of motor weakness in any of his limbs.
On examination, he was well oriented to time, place, and person. Signs of meningeal irritation were absent. We also did not find any cranial nerve deficit, papilledema, or long tract signs. Systemic examination was also unremarkable. He had taken symptomatic treatment without much relief in his symptoms. Family history was unremarkable for any intracranial pathologies.
Considering the nature and severity of his symptoms, we obtained an MRI brain with and without contrast. MRI brain showed a midline prepontine cyst with signals identical to cerebrospinal fluid (CSF) on T1 and T2-weighted images [Figures
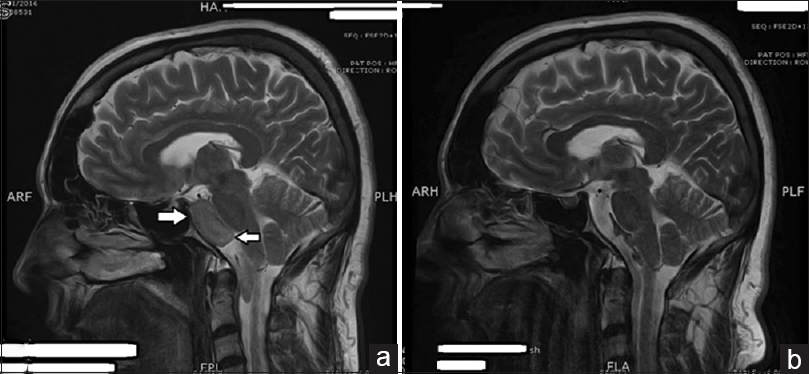
Figure 1
(a) A well-defined extra-axial lesion is identified anterior to the brainstem on this sagittal view, appearing hyper intense relative to brain parenchyma on the T2 weighted image (White arrows). (b) Similar section noted one year later with reduction in mass of the cystic lesion identified in the image a
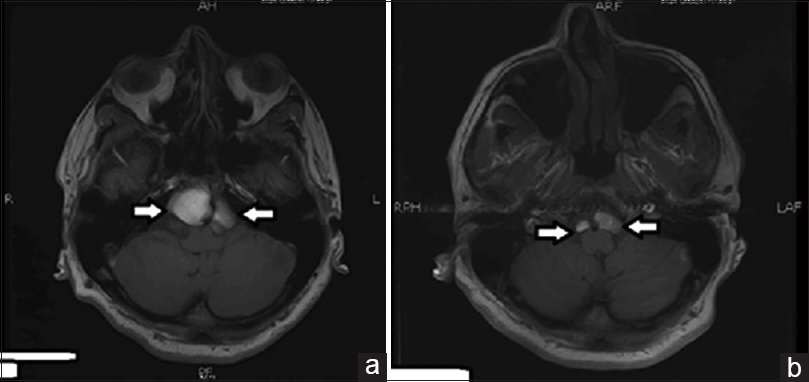
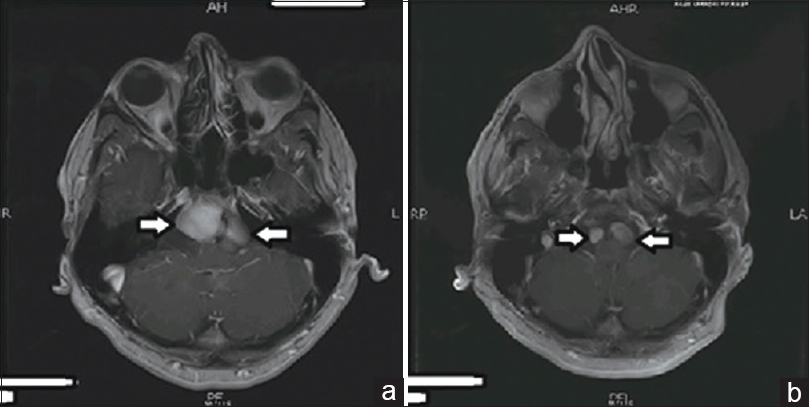
Figure 3
(a) T1 weighted image with contrast Brain MRI, this axial section identifies the lesion anterior to the brain stem appearing hyper intense relative to brain parenchyma with no enhancement noticed on contrast (White arrows). (b) Similar section noted one year later with reduction in mass of the cystic lesion identified in the image a
We admitted the patient for further management. He received symptomatic management along with empirical antibiotics. Considering the possibility of chemical meningeal irritation, we also started dexamethasone for 1 week. The patient improved within the next 48 hours and was discharged with a plan for close clinical and radiological follow-up.
After discharge, the patient remained symptom free, and returned with a repeat MRI brain after 1 year. Repeat imaging showed a significant size reduction and decrease in mass effect [Figure
DISCUSSION
We have described the case of a patient with self-resolving prepontine cyst. Considering the location and radiological features, our top differentials were epidermoid and neurenteric cyst. Epidermoid cysts comprise 0.2–1.8% of primary intracranial tumors.[
Epidermoid cyst on a computed tomography (CT) scan is a round/lobulated mass with a density resembling CSF, calcification is seen in 10% of the cases.[
Neurenteric cysts are mostly found in the posterior fossa and are typically midline, anterior to the brainstem.[
CONCLUSION
Although spontaneous resolution of prepontine cysts is rare, in patients who are neurologically intact, symptomatic management with close clinical and radiological follow-up may prove useful.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Basheer N, Kasliwal MK, Suri A, Sharma MC, Arora A, Sharma BS. Lateral extradural, supratentorial neurenteric cyst. J Clin Neurosci. 2010. 17: 639-41
2. Bejjani GK, Wright DC, Schessel D, Sekhar LN. Endodermal cysts of the posterior fossa: Report of three cases and review of the literature. J Neurosurg. 1998. 89: 326-35
3. Chen CY, Wong JS, Hsieh SC, Chu JS, Chan WP. Intracranial epidermoid cyst with hemorrhage: MR imaging findings. Am J Neuroradiol. 2006. 27: 427-9
4. Chen CY, Wong JS, Hsieh SC, Chu JS, Chan WP. Intracranial epidermoid cyst with hemorrhage: MR imaging findings. AJNR Am J Neuroradiol. 2006. 27: 427-9
5. Chowdhury FH, Haque MR, Sarker MH. Intracranial epidermoid tumor; microneurosurgical management: An experience of 23 cases. Asian J Neurosurg. 2013. 8: 21-
6. Christov C, Chretien F, Brugieres P, Djindjian M. Giant supratentorial enterogenous cyst: Report of a case, literature review, and discussion of pathogenesis. Neurosurgery. 2004. 54: 759-63
7. deSouza CE, deSouza R, da Costa S, Sperling N, Yoon TH, Abdelhamid MM. Cerebellopontine angle epidermoid cysts: A report on 30 cases. J Neurol Neurosurg Psychiatry. 1989. 52: 986-90
8. Dodd RL, Barnes PD, Huhn SL. Spontaneous resolution of a prepontine arachnoid cyst. Case report and review of the literature. Pediatr Neurosurg. 2002. 37: 152-7
9. Kobata H, Kondo A, Iwasaki K. Cerebellopontine angle epidermoids presenting with cranial nerve hyperactive dysfunction. Skull Base. 2002. 12: 178-
10. Miyazaki S, Fukushima T, Takusagawa Y. Epidermoid presenting as trigeminal neuralgia. Neurol Med Chir. 1984. 24: 774-81
11. Osborn AG, Preece MT. Intracranial cysts: Radiologic-pathologic correlation and imaging approach. Radiology. 2006. 239: 650-64
12. Osborn AG, Preece MT. Intracranial cysts: Radiologic-pathologic correlation and imaging approach 1. Radiology. 2006. 239: 650-664
13. Preece M, Osborn A, Chin S, Smirniotopoulos J. Intracranial neurenteric cysts: Imaging and pathology spectrum. Am J Neuroradiol. 2006. 27: 1211-6
14. Sampath S, Yasha TC, Shetty S, Chandramouli BA. Parasellar neurenteric cyst: Unusual site and histology: Case report. Neurosurgery. 1999. 44: 1335-
15. Zhou LF. Intracranial epidermoid tumours: Thirty-seven years of diagnosis and treatment. Br J Neurosurg. 1990. 4: 211-6

