

- Department of Neurosurgery, University of Washington, Seattle, Washington, United States,
- Department of Medicine, Firat University, Elazig, Turkey,
- Department of Medicine, University of Paris, Paris, France,
- Department of Radiology, Univ of Washington, Seattle, Washington, United States.
Correspondence Address:
Zaid Aljuboori, Department of Neurosurgery, University of Washington, Seattle, Washington, United States.
DOI:10.25259/SNI_878_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Zaid Aljuboori1, Margaret McGrath1, Muhammed Amir Essibayi2, Saif Zaidi3, Danial Hallam4, Basavaraj Ghodke4. Spontaneous spinal cerebrospinal fluid venous-fistula treated with transvenous embolization: A case report. 30-Sep-2021;12:492
How to cite this URL: Zaid Aljuboori1, Margaret McGrath1, Muhammed Amir Essibayi2, Saif Zaidi3, Danial Hallam4, Basavaraj Ghodke4. Spontaneous spinal cerebrospinal fluid venous-fistula treated with transvenous embolization: A case report. 30-Sep-2021;12:492. Available from: https://surgicalneurologyint.com/surgicalint-articles/11135/
Date of Submission
31-Aug-2021
Date of Acceptance
04-Sep-2021
Date of Web Publication
30-Sep-2021
Abstract
Background: Spinal cerebrospinal fluid venous fistula (CVF) is a recognized cause of chronic positional headache and spontaneous intracranial hypotension (SIH). It occurs due to an aberrant connection formed between the spinal subarachnoid space and an adjacent spinal epidural vein. The diagnosis of CVF can be difficult to establish but can be documented utilizing advanced imaging techniques (e.g., enhanced MR myelography/digital subtraction myelography). Their treatment involves surgical ligation of the involved nerve root, imaging-guided epidural blood patching, and/or endovascular embolization. Here, we report a 40-year-old male who presented with a symptomatic lumbar CVF successfully treated with transvenous embolization.
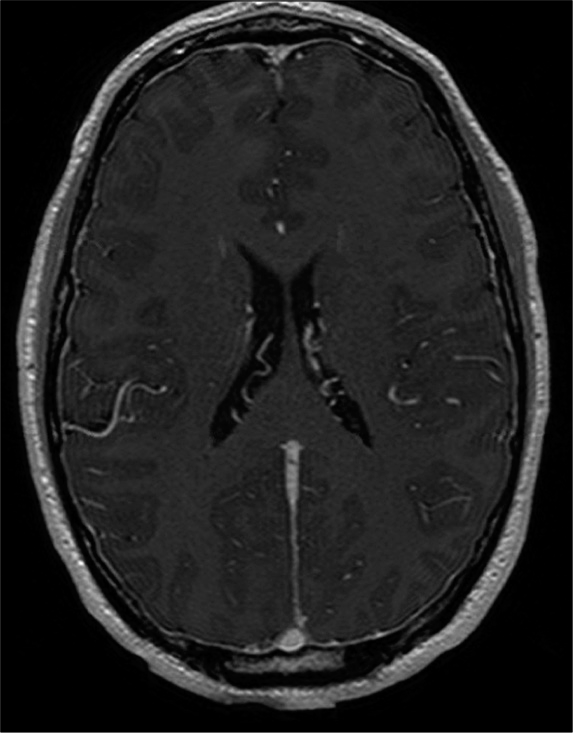
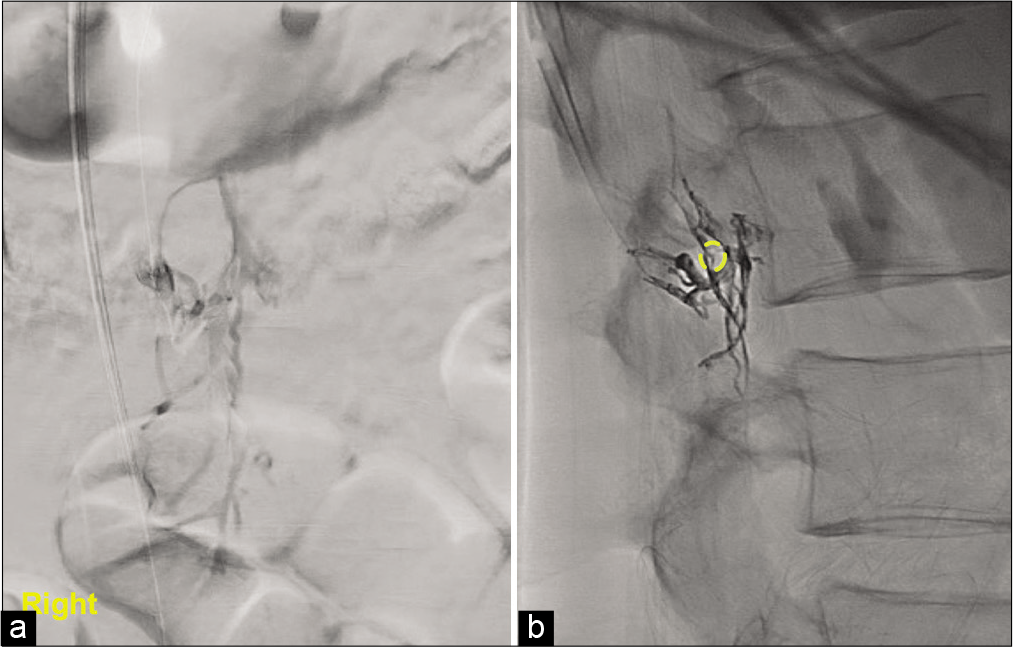
Case Description: A 40-year-old male presented with several months of positional headaches. The MRI of the brain showed diffuse pachymeningeal enhancement consistent with the diagnosis of SIH. Although the MR of the lumbar spine was unremarkable, the MR myelogram with digital subtraction imaging showed a CVF at the L2 level. Following transvenous embolization (i.e., through the Azygous vein), the patient’s symptoms fully resolved.
Conclusion: Spinal CVF are rare and may cause chronic headaches and symptoms/signs of SIH. In this case, an MR myelogram with digital subtraction images demonstrated the anomalous connection between the spinal subarachnoid space and an adjacent spinal epidural vein at the L2 level. Although open surgical ablation of this connection may be feasible, less invasive techniques such as endovascular embolization should become the treatment of choice for the future management of CVF.
Keywords: Cerebrospinal fluid, Embolization, Fistula, Venous
INTRODUCTION
Cerebrospinal fluid venous fistula (CVF) is defined as an aberrant connection formed between the spinal subarachnoid space and an adjacent spinal epidural veins allowing for the unregulated loss of cerebrospinal fluid into the circulatory system.[
CASE DESCRIPTION
A 40-year-old male presented with spontaneous onset of SIH characterized by positional headaches for several months. His neurological exam was normal. The enhanced MRI of the brain showed diffuse pachymeningeal enhancement consistent with SIH [

DISCUSSION
SIH
SIH patients are typically females in their 5th/6th decades.[
Levels of CVF
Most CVF are found in the thoracic spine; only a few cases are found in the cervical and lumbar regions.[
CONCLUSION
CVF, responsible for SIH, is best diagnosed utilizing MRmyelography/digital subtraction myelograms. Although direct surgical treatment may be successful, endovascular procedures are increasingly and less invasively effectively managing CVF Lesions.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Amrhein TJ, Kranz PG. Spontaneous intracranial hypotension: Imaging in diagnosis and treatment. Radiol Clin North Am. 2019. 57: 439-51
2. Brinjikji W, Savastano LE, Atkinson JL, Garza I, Farb R, Cutsforth-Gregory JK. A novel endovascular therapy for CSF hypotension secondary to CSF-venous fistulas. AJNR Am J Neuroradiol. 2021. 42: 882-7
3. Chazen JL, Robbins MS, Strauss SB, Schweitzer AD, Greenfield JP. MR myelography for the detection of CSF-venous fistulas. AJNR Am J Neuroradiol. 2020. 41: 938-40
4. Chiapparini L, Farina L, D’Incerti L, Erbetta A, Pareyson D, Carriero MR. Spinal radiological findings in nine patients with spontaneous intracranial hypotension. Neuroradiology. 2002. 44: 143-50
5. Clark MS, Diehn FE, Verdoorn JT, Lehman VT, Liebo GB, Morris JM. Prevalence of hyperdense paraspinal vein sign in patients with spontaneous intracranial hypotension without dural CSF leak on standard CT myelography. Diagn Interv Radiol. 2018. 24: 54-9
6. Duvall JR, Robertson CE, Cutsforth-Gregory JK, Carr CM, Atkinson JL, Garza I. Headache due to spontaneous spinal cerebrospinal fluid leak secondary to cerebrospinal fluid-venous fistula: Case series. Cephalalgia. 2019. 39: 1847-54
7. Kranz PG, Amrhein TJ, Gray L. CSF Venous fistulas in spontaneous intracranial hypotension: Imaging characteristics on dynamic and CT myelography. AJR Am J Roentgenol. 2017. 209: 1360-6
8. Kranz PG, Amrhein TJ, Schievink WI, Karikari IO, Gray L The. “Hyperdense Paraspinal Vein” sign: A marker of CSF-venous fistula. AJNR Am J Neuroradiol. 2016. 37: 1379-81
9. Kranz PG, Gray L, Malinzak MD, Amrhein TJ. Spontaneous intracranial hypotension: Pathogenesis, diagnosis, and treatment. Neuroimaging Clin N Am. 2019. 29: 581-94
10. Kumar N, Diehn FE, Carr CM, Verdoorn JT, Garza I, Luetmer PH. Spinal CSF venous fistula: A treatable etiology for CSF leaks in craniospinal hypovolemia. Neurology. 2016. 86: 2310-2
11. Roytman M, Salama G, Robbins MS, Chazen JL. CSF-venous fistula. Curr Pain Headache Rep. 2021. 25: 5
12. Schievink WI, Moser FG, Maya MM. CSF-venous fistula in spontaneous intracranial hypotension. Neurology. 2014. 83: 472-3
13. Shlobin NA, Shah VN, Chin CT, Dillon WP, Tan LA. Cerebrospinal fluid-venous fistulas: A systematic review and examination of individual patient data. Neurosurgery. 2021. 88: 931-41

