

- Department of Ortho-Spine Surgery, Sir Ganga Ram Hospital, New Delhi, Delhi, India.
DOI:10.25259/SNI_23_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nitin Maruti Adsul, Vishnu Panigrahi, Shankar Acharya, K. L. Kalra, R. S. Chahal. Stenotrophomonas maltophilia spondylodiscitis following lumbar microdiscectomy mimicking a cotton granuloma: A case report and literature review. 25-Feb-2020;11:28
How to cite this URL: Nitin Maruti Adsul, Vishnu Panigrahi, Shankar Acharya, K. L. Kalra, R. S. Chahal. Stenotrophomonas maltophilia spondylodiscitis following lumbar microdiscectomy mimicking a cotton granuloma: A case report and literature review. 25-Feb-2020;11:28. Available from: https://surgicalneurologyint.com/surgicalint-articles/9876/
Date of Submission
19-Jan-2020
Date of Acceptance
31-Jan-2020
Date of Web Publication
25-Feb-2020
Abstract
Background:Vertebral osteomyelitis caused by Stenotrophomonas maltophilia is very rare. There are only two cases reported in literature. Here, we present a 48-year-old immunocompetent male who, following a lumbar microdiscectomy, developed postoperative spondylodiscitis due to S. maltophilia that mimicked a cotton granuloma.
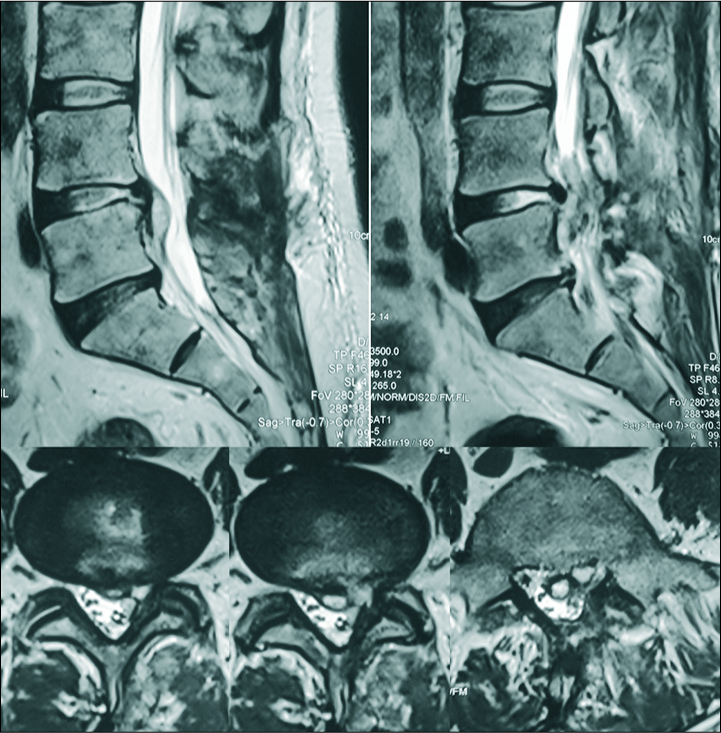
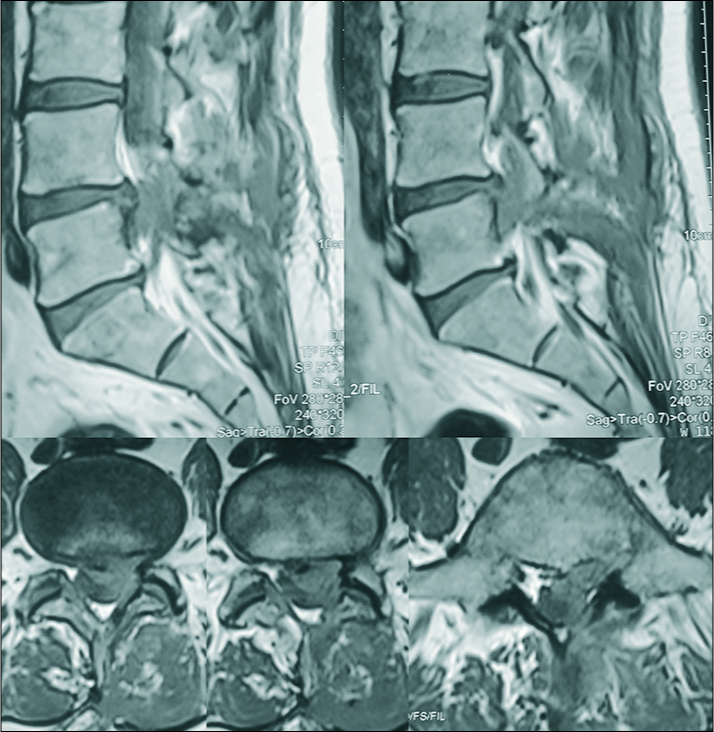
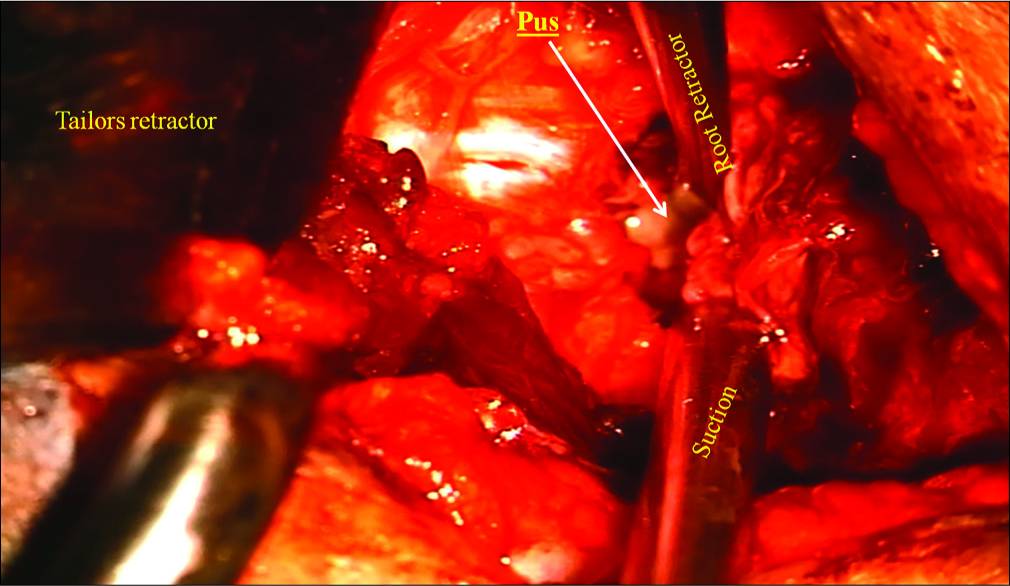
Case Report:Two months ago, a 48-year-old male underwent a lumbar L4-L5 microdiscectomy, he newly presented with the left thigh and leg pain of 4 weeks duration. Laboratory studies revealed a CRP of 26 mg/l, an ESR of 6 mm (1st h), and total leukocyte count of 7.85 thousand/ul. The MRI T2 images showed a focal hyperintense lesion in the left lateral recesses at the L4-L5 level; the accompanying hypointense-smooth margin resembled a cotton granuloma. At surgery, we found a localized epidural collection of pus; S. maltophilia was isolated from the culture. His symptoms gradually improved, and symptoms fully resolved with 3 months of subsequent antibiotic therapy.
Conclusion:S. maltophilia causing vertebral osteomyelitis is extremely rare and can sometimes mimic a cotton granuloma. MR diagnosis, surgical decompression, and obtaining cultures are requisite to direct appropriate antibiotic therapy.
Keywords: Cotton granuloma, Spondylodiscitis, Stenotrophomonas maltophilia
INTRODUCTION
Different spinal infections include spondylodiscitis, septic discitis, spondylitis, and/or vertebral osteomyelitis (e.g., including endplate and/or epidural abscess). However, vertebral osteomyelitis caused by S. maltophilia attributed to a lumbar microdiscectomy is very rare.[
CASE REPORT
Two months ago, a nonimmunocompromised hypertensive 48-year-old male underwent an L4-L5 microdiscectomy [
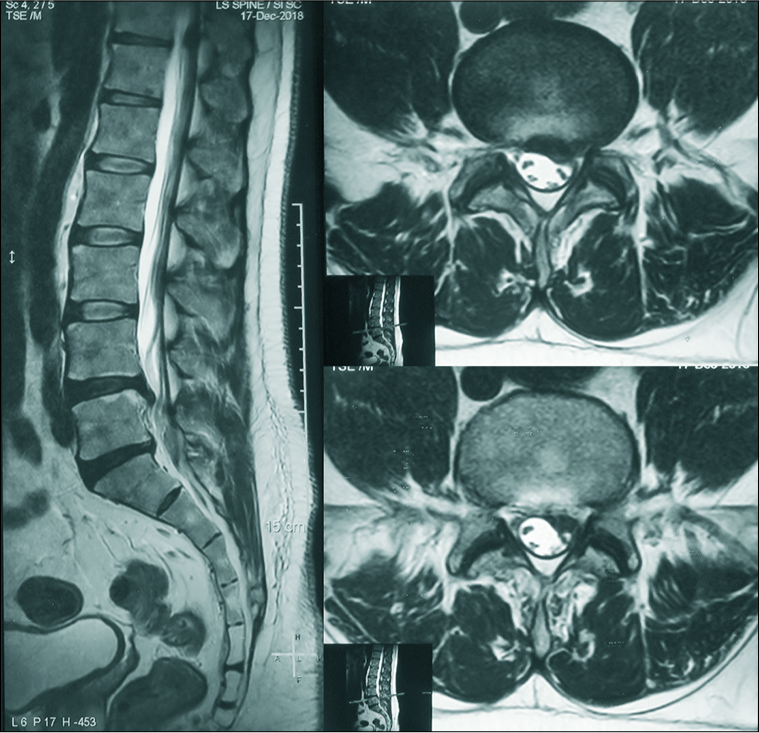
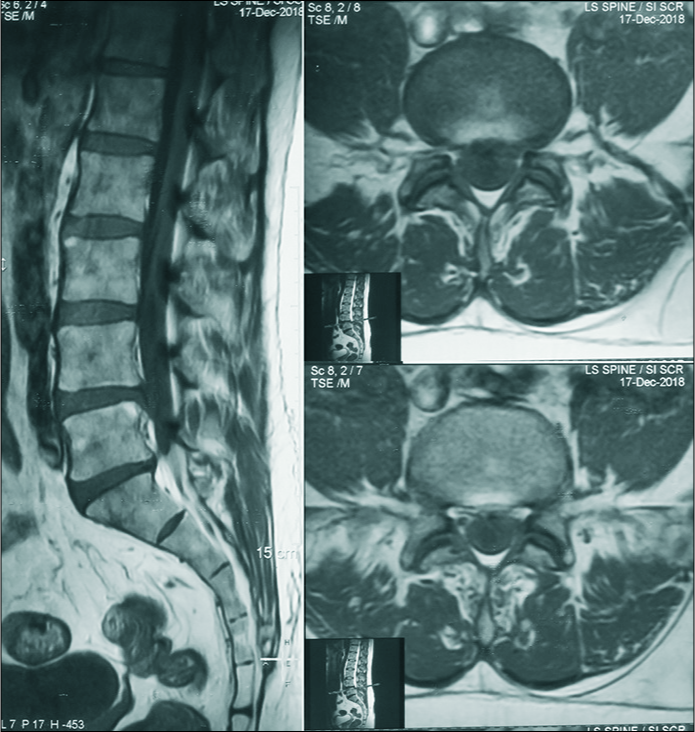
Laboratory studies showed a CRP of 26 mg/l, an ESR of 6 mm (1st h), and total leukocyte count of 7.85 thousand/ul. MRI T2 images showed a focal hyperintense lesion in the left lateral recesses at the L4-L5 level with an accompanying hypointense/smooth margin resembling a cotton granuloma [
DISCUSSION
S. maltophilia is a Gram-negative aerobic bacillus that is commonly found in the environment causing hospital- acquired infections in immunocompromised hosts. It is typically resistant to most broad-spectrum antibiotics.[
Laboratory studies
Laboratory evaluations for S. maltophilia infections typically show elevated WBC counts (60%), elevated ESR and CRP levels (90%), and positive blood cultures (65%).[
CONCLUSION
A high degree of suspicion was required in this case to diagnose S. maltophilia as causing postoperative spondylodiscitis and must be differentiated from cotton granulomas. Here, after obtaining definitive cultures utilizing open surgical approach, prolonged antibiotics treatment was warranted.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chen WH, Jiang LS, Dai LY. Surgical treatment of pyogenic vertebral osteomyelitis with spinal instrumentation. Eur Spine J. 2007. 16: 1307-16
2. Denton M, Kerr KG. Microbiological and clinical aspects of infection associated with Stenotrophomonas maltophilia. Clin Microbiol Rev. 1998. 11: 57-80
3. Friedman ND, Korman TM, Fairley CK, Franklin JC, Spelman DW. Bacteraemia due to Stenotrophomonas maltophilia An analysis of 45 episodes. J Infect. 2002. 45: 47-53
4. Gasbarrini A, Boriani L, Salvadori C, Mobarec S, Kreshak J, Nanni C. Biopsy for suspected spondylodiscitis. Eur Rev Med Pharmacol Sci. 2012. 16: 26-34
5. Kang BU, Lee SH, Ahn Y, Choi WC, Choi YG. Surgical site infection in spinal surgery: Detection and management based on serial C-reactive protein measurements. J Neurosurg Spine. 2010. 13: 158-64
6. Okten AI, Adam M, Gezercan Y. Textiloma: A case of foreign body mimicking a spinal mass. Eur Spine J. 2006. 15: 626-9

