

- Department of Neurosurgery, Kyoto University, Kyoto, Japan
- Department of Neurosurgery, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan
Correspondence Address:
Taichi Ikedo, Department of Neurosurgery, Kyoto University, Kyoto, Japan.
DOI:10.25259/SNI_195_2025
Copyright: © 2025 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Taichi Ikedo1,2, Takaaki Itazu2, Hirotoshi Imamura2, Yuto Inoue2, Shinya Tabata2, Koji Shimonaga2, Eika Hamano2, Kiyofumi Yamada2, Hisae Mori2, Koji Iihara2, Hiroharu Kataoka2. Successful endovascular occlusion of multiple fusiform aneurysms on the persistent primitive lateral basilovertebral anastomosis. 16-May-2025;16:185
How to cite this URL: Taichi Ikedo1,2, Takaaki Itazu2, Hirotoshi Imamura2, Yuto Inoue2, Shinya Tabata2, Koji Shimonaga2, Eika Hamano2, Kiyofumi Yamada2, Hisae Mori2, Koji Iihara2, Hiroharu Kataoka2. Successful endovascular occlusion of multiple fusiform aneurysms on the persistent primitive lateral basilovertebral anastomosis. 16-May-2025;16:185. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=13555
Date of Submission
22-Feb-2025
Date of Acceptance
14-Apr-2025
Date of Web Publication
16-May-2025
Abstract
Background: The primitive lateral basilovertebral anastomosis (PLBA) is a transient embryonic vessel in the vertebrobasilar system that typically regresses during cerebellar artery development. Persistent PLBA (PPLBA), which forms a vertebrobasilar duplication, is a rare vascular anomaly. This is the first reported case of multiple fusiform aneurysms associated with a PPLBA.
Case Description: A 14-year-old girl was diagnosed with intracranial aneurysms before undergoing coronary artery bypass grafting surgery for myocardial infarction. Digital subtraction angiography showed two fusiform aneurysms on a PPLBA, connecting the left vertebral artery (VA) and the left anterior inferior cerebellar artery (AICA). After 3 years of follow-up, a new aneurysm developed at the origin of the PPLBA, proximal to the existing two aneurysms. Due to the AICA blood flow originating mainly from the basilar artery (BA) rather than the PPLBA, endovascular parent artery occlusion of the PPLBA was planned to prevent aneurysmal rupture and subarachnoid hemorrhage. Complete occlusion of all three aneurysms was achieved without complications.
Conclusion: Understanding the embryological anatomy of this rare vertebrobasilar duplication involving the PPLBA, AICA, BA, and VA facilitated the successful development of a therapeutic strategy. Aneurysms associated with PPLBA exhibit various vascular structures and can be treated effectively with tailored endovascular approaches.
Keywords: Endovascular parent artery occlusion, Fusiform aneurysms, Persistent primitive lateral basilovertebral anastomosis, Vertebrobasilar duplication
INTRODUCTION
The primitive lateral basilovertebral anastomosis (PLBA) is a transient embryonic vessel of the vertebrobasilar artery system, first described by Padget in 1948.[
We report the first case of multiple fusiform aneurysms associated with a PPLBA. In this case, because the PPLBA formed a vertebrobasilar duplication, endovascular occlusion of the PPLBA with fusiform aneurysms was successfully performed.
CASE PRESENTATION
A 14-year-old girl was admitted with intracranial aneurysms detected on magnetic resonance angiography during preoperative assessment before coronary artery bypass grafting surgery for myocardial infarction. Digital subtraction angiography (DSA) revealed two fusiform aneurysms on the PPLBA, connecting the left vertebral artery (VA) and left anterior inferior cerebellar artery (AICA) [
After 3 years of follow-up, a new aneurysm developed at the origin of the PPLBA, proximal to the previous two aneurysms on DSA images [

Figure 1:
DSA images at the time of diagnosis. (a) Two fusiform aneurysms on a PPLBA connecting the left VA and left anterior inferior cerebellar artery at the first diagnosis. A black arrow indicates the fusiform aneurysms. (b) An additional de novo aneurysm appeared at the origin of the PPLBA just proximal to the previous two aneurysms after 3 years of follow-up (a white arrow). (c) A 3D-DSA image of the multiple aneurysms. The PPLBA, AICA, BA, and VA form a loop structure of the vertebrobasilar duplication. A white arrow indicates the connection between the PPLBA and AICA. (d and e) Blood flow of left AICA was observed in the earlier phase through the BA than the PPLBA. Early (d) and late phase (e). Black arrowheads indicate the blood flow of the AICA from the BA. (f) High-resolution CBCT showed no obvious perforators on the aneurysms and PPLBA. DSA: Digital subtraction angiography, PPLBA: Persistent primitive lateral basilovertebral anastomosis, VA: Vertebral artery, AICA: Anterior inferior cerebellar artery, BA: Basilar artery, CBCT: Cone-beam computed tomography.
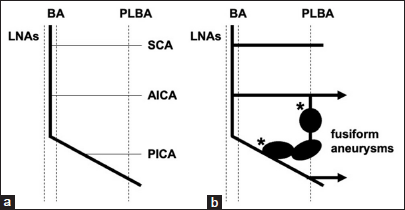
Figure 2:
Normal embryonic development of the arteries in the posterior circulation and schema of the present case. (a) Normal development. (b) The schema of the present case. The three aneurysms were on the PPLBA, forming the loop structure of the vertebrobasilar duplication. Two asterisks indicate the distance of the coil embolization. LNAs: Longitudinal neural arteries, PLBA: Primitive lateral basilovertebral anastomosis, SCA: Superior cerebellar artery, PICA: Posterior inferior cerebellar artery

Figure 3:
DSA and MRI images of perioperative periods. (a) The tip of the microcatheter was inserted into the distal fusiform aneurysm. A white arrow indicates the tip of the microcatheter. (b) Coil mass after complete occlusion of the multiple aneurysms. (c) DSA showed complete occlusion of the multiple aneurysms. (d) A DWI image after endovascular therapy. DSA: Digital subtraction angiography, MRI: Magnetic resonance imaging, DWI: Diffusion-weighted imaging.
DISCUSSION
We report the first successful treatment of multiple fusiform aneurysms of the PPLBA through parental artery occlusion. The duplicated vertebrobasilar system, comprising the BA and PPLBA, facilitated endovascular parent artery occlusion of the PPLBA.
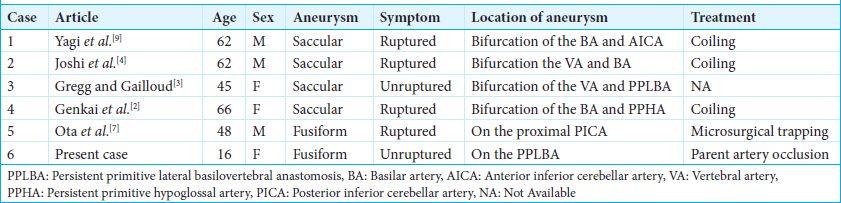
Aneurysm formation has rarely been observed in the PPLBA system. Six reports, including the present case, of intracranial aneurysms associated with the PPLBA are listed in
The other two aneurysms (33%), including this case, were fusiform. Ota et al.[
In the case of the BA fenestration, perforating arteries are usually involved because it is consisted of the LNAs.[
The etiology of fusiform and bifurcated aneurysms may differ, potentially involving factors such as hemodynamic conditions, genetic predisposition, or systemic vascular fragility factors. Given the patient’s history of multiple coronary aneurysms of unknown etiology, both hemodynamic stress and systemic vascular fragility may have contributed to aneurysm formation in the intracranial PPLBA.
CONCLUSION
In this case, the rare looped vertebrobasilar duplication, encompassing the PPLBA, AICA, BA, and VA, facilitated endovascular occlusion of the PPLBA and associated fusiform aneurysms. Aneurysms associated with PPLBA exhibit diverse vascular morphologies and can be effectively treated by understanding their embryological development.
Ethical approval:
The Institutional Review Board approval is not required.
Declaration of patient consent:
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship:
Nil.
Conflicts of interest:
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation:
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. De Caro R, Serafini MT, Galli S, Parenti A, Guidolin D, Munari PF. Anatomy of segmental duplication in the human basilar artery. Possible site of aneurysm formation. Clin Neuropathol. 1995. 14: 303-9
2. Genkai N, Okamoto K, Nomura T, Abe H. Endovascular treatment of a ruptured aneurysm arising from the proximal end of a partial vertebrobasilar duplication with a contralateral prominent persistent primitive hypoglossal artery: Illustrative case. J Neurosurg Case Lessons. 2021. 1: CASE20108
3. Gregg L, Gailloud P. The role of the primitive lateral basilovertebral anastomosis of padget in variations of the vertebrobasilar arterial system. Anat Rec (Hoboken). 2017. 300: 2025-38
4. Joshi KC, Thomas A, Jagannatha AT, Garg D. Stent-assisted coiling of aneurysm in a persistent primitive lateral vertebrobasilar system. World Neurosurg. 2016. 86: 513 e9-14
5. Moffat DB. The embryology of the arteries of the brain. Ann R Coll Surg Engl. 1962. 30: 368-82
6. Ota T, Dofuku S, Sato M. Persistence of primitive lateral basilovertebral anastomosis with a ruptured posterior inferior cerebellar artery aneurysm: A case report. NMC Case Rep J. 2022. 9: 69-72
7. Ota T, Komiyama M. Vascular supply of the hindbrain: Basic longitudinal and axial angioarchitecture. Interv Neuroradiol. 2022. 28: 756-64
8. Padget DH. The development of the cranial arteries in the human embryo. Contrib Embryol. 1948. 32: 205-261
9. Yagi K, Satoh K, Satomi J, Nagahiro S. Primitive vertebrobasilar system associated with a ruptured aneurysm. AJNR Am J Neuroradiol. 2004. 25: 781-3

