

- Department of Neurosurgery, Graduate School of Medicine, Yokohama City University, Yokohama, Japan.
- Department of Pathology, Graduate School of Medicine, Yokohama City University, Yokohama, Japan.
- Department of Neurosurgery, Iemasa Neurosurgical Clinic, Yokohama, Kanagawa, Japan.
Correspondence Address:
Hidetoshi Murata, Department of Neurosurgery, Graduate School of Medicine, Yokohama City University, Yokohama, Kanagawa, Japan.
DOI:10.25259/SNI_868_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Yuta Otomo1, Naoki Ikegaya1, Akito Oshima1, Shutaro Matsumoto1, Naoko Udaka2, Chia-Cheng Chang3, Kensuke Tateishi1, Hidetoshi Murata1, Tetsuya Yamamoto1. Superficial siderosis and nonobstructive hydrocephalus due to subependymoma in the ventricle: An illustrative case report. 30-Dec-2021;12:631
How to cite this URL: Yuta Otomo1, Naoki Ikegaya1, Akito Oshima1, Shutaro Matsumoto1, Naoko Udaka2, Chia-Cheng Chang3, Kensuke Tateishi1, Hidetoshi Murata1, Tetsuya Yamamoto1. Superficial siderosis and nonobstructive hydrocephalus due to subependymoma in the ventricle: An illustrative case report. 30-Dec-2021;12:631. Available from: https://surgicalneurologyint.com/surgicalint-articles/11308/
Date of Submission
28-Aug-2021
Date of Acceptance
14-Dec-2021
Date of Web Publication
30-Dec-2021
Abstract
Background: Intraventricular tumors can generally result in obstructive hydrocephalus as they grow. Rarely, however, some intraventricular tumors develop superficial siderosis (SS) and trigger hydrocephalus, even though the tumor has hardly grown. Here, we present an illustrative case of SS and nonocclusive hydrocephalus caused by subependymoma of the lateral ventricles.
Case Description: A 78-year-old man with an intraventricular tumor diagnosed 7 years ago had been suffering from gait disturbance for 2 years. He also developed cognitive impairment. Intraventricular tumors showed little growth on annual magnetic resonance imaging (MRI). MRI T2-star weighted images (T2*WI) captured small intratumoral hemorrhages from the beginning of the follow-up. Three years before, at the same time as the onset of ventricular enlargement, T2*WI revealed low intensity in the whole tumor and cerebral surface. Subsequent follow-up revealed that this hemosiderin deposition had spread to the brain stem and cerebellar surface, and the ventricles had expanded further. Cerebrospinal fluid (CSF) examination revealed xanthochromia. The tumor was completely removed en bloc. Histopathological findings were consistent with those of subependymoma. Although CSF findings improved, SS and hydrocephalus did not improve. Therefore, the patient underwent a lumboperitoneal shunt for CSF diversion after tumor resection.
Conclusion: Some intraventricular tumors cause SS and nonobstructive hydrocephalus due to microbleeding, even in the absence of tumor growth. T2*WI and, if necessary, timely CSF examination can allow identification of presymptomatic SS. This follow-up strategy may provide a favorable course by facilitating early intervention in patients with intraventricular lesions, not just subependymomas.
Keywords: Cerebrospinal fluid testing, Nonobstructive hydrocephalus, Subependymoma, Superficial siderosis, T2-star weighted image
INTRODUCTION
Intraventricular tumors can generally result in obstructive hydrocephalus as they grow. Subependymoma, which is a benign ventricular tumor, is generally followed up with imaging unless they grow or result in hydrocephalus.[
CASE DESCRIPTION
A 78-year-old man with an intraventricular tumor diagnosed 7 years before had been suffering from gait disturbance for 2 years [
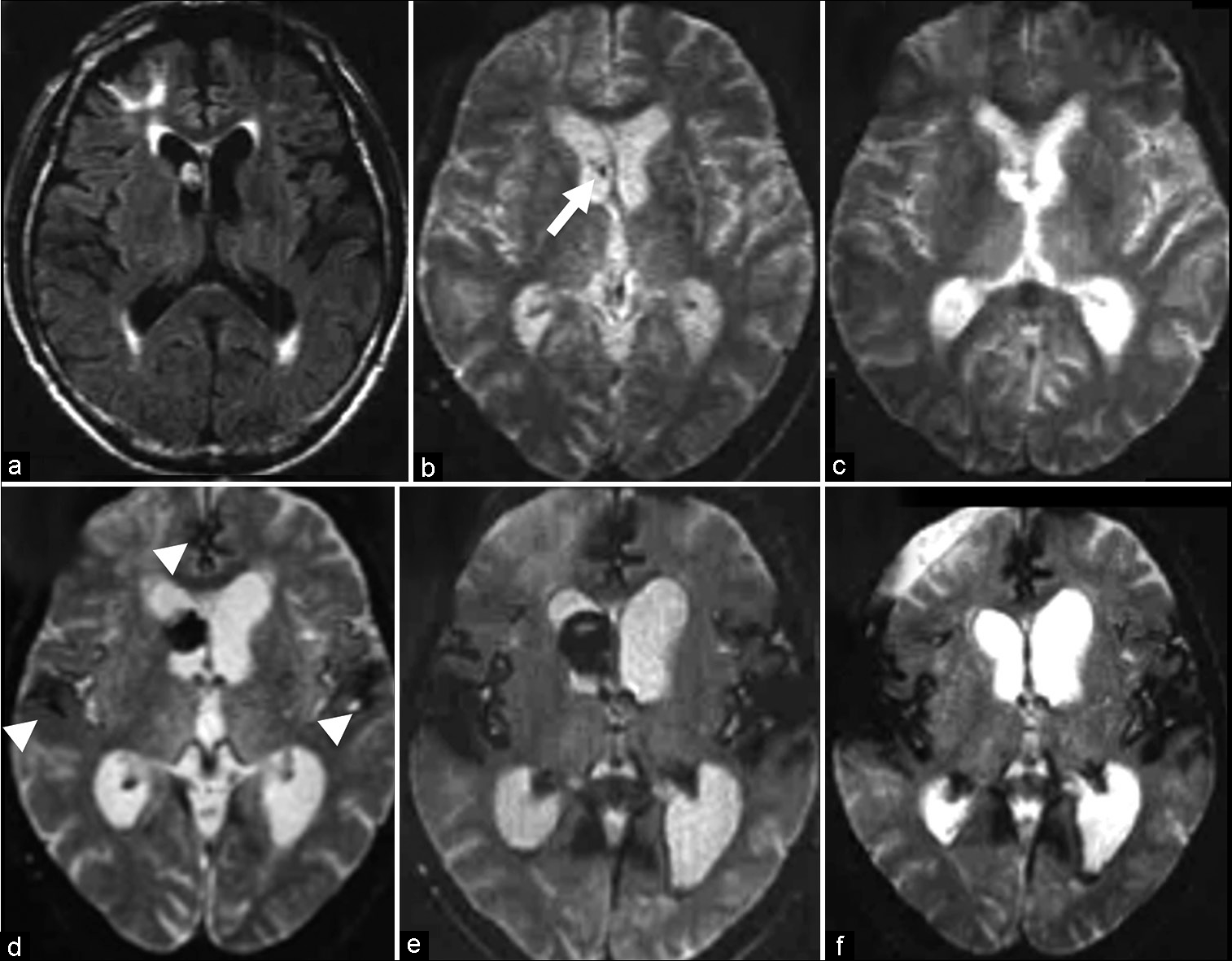
Figure 1:
Magnetic resonance imaging (MRI) findings. Initial fluid-attenuated inversion recovery MRI showing an intraventricular tumor (a). Initial T2-star weighted MRI (T2*WI) also revealed a tiny low-intensity spot (arrow), suggesting intratumoral hemorrhage 7 years before surgery (b). Note that 5 years before surgery, this signal change was localized within the tumor and not on the brain surface (c). Low intensity suggesting intratumoral hemorrhage and superficial siderosis on the brain surface (arrowhead) is demonstrated on T2*WI 3 years before surgery and ventricular enlargement progresses (d), and is exacerbated immediately before surgery (e). Hemosiderin deposition and hydrocephalus persisted even after tumor removal (f).
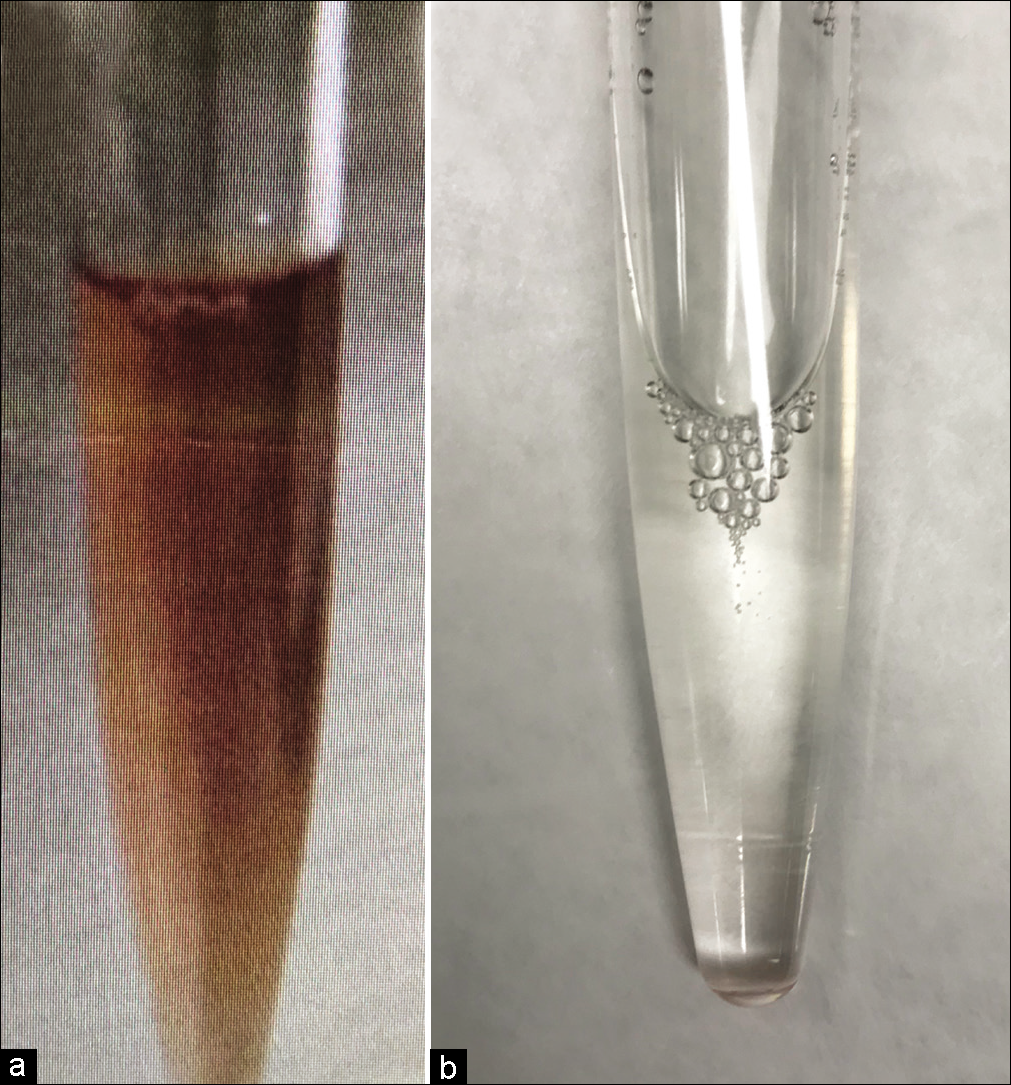
The timed up and go test before and after the cerebrospinal fluid (CSF) tap test in the presurgical evaluation showed improvement in gait disturbance, suggesting responsiveness to CSF diversion. On the other hand, CSF analysis demonstrated xanthochromia, a white blood cell (WBC) count of 154/μl (normal range 0–15/μL), and protein level of 596 mg/dL (normal range 10–40 mg/dL) [
Tumor resection was performed through a right frontal craniotomy. Visual inspection revealed that the ventricular wall turned yellowish-brown, suggesting deposition of hemosiderin on the ependyma [
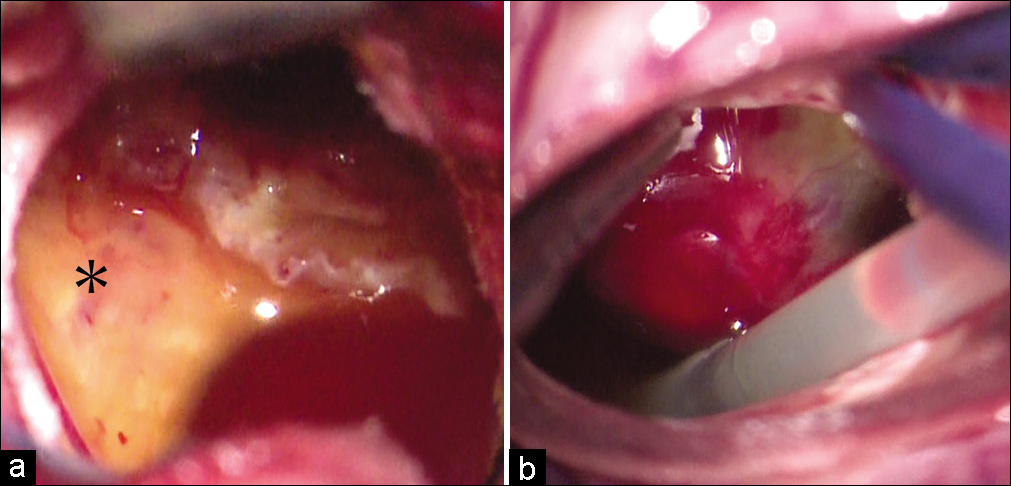
Figure 3:
Intraoperative photographs of the left lateral ventricle. (a) Black asterisk showing the ventricular wall is colored yellowish-brown, suggesting deposition of hemosiderin on the ependyma. (b) The tumor surface turns a mixture of yellow and red, suggesting the presence of hemorrhage at different times.
Histopathological findings were consistent with those of subependymomas. Although the tumor surface color suggested that multiple hemorrhages in different phases and slight microbleeding changes were observed in the tumor, Elastica van Gieson staining did not reveal any significant disruption of the tumor blood vessels [
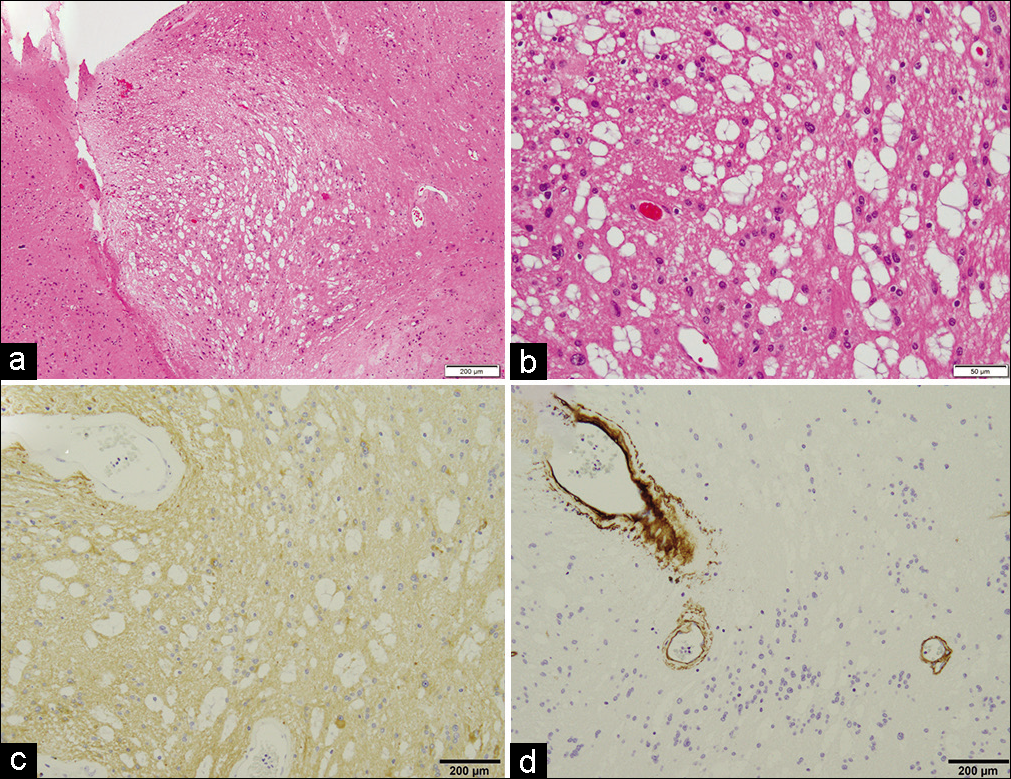
Figure 4:
(a) Low magnification and (b) high magnification: hematoxylin and eosin staining. Clusters of oval-shaped cells and isomorphic nuclei are embedded in a fine fibrillary back ground. Many microcystic formations and microbleeding changes were also seen in the tumor. (c) Immunohistochemical staining revealing a positive reaction for glial fibrillary acidic protein. The pathological findings of a-c are consistent with those of subependymoma. (d) Elastica van Gieson staining revealed a positive reaction for collagen type IV on the vessel walls, which suggests that the vessel walls in the tumor are normal.
During the postoperative course, MRI revealed total tumor removal and no postoperative complications [
DISCUSSION
We describe a case of SS and hydrocephalus caused by subependymoma of the lateral ventricles. It is very important to recognize that some intraventricular tumors can cause SS and nonobstructive hydrocephalus without tumor growth due to microbleeding. The clinical course of the patient has two important clinical issues. First, subependymoma of the lateral ventricles can be a source of bleeding, leading to SS and nonobstructive hydrocephalus. Second, MRI T2*WI and a final CSF examination might allow the identification of presymptomatic SS and prevent irreversible SS through intraventricular tumor resection.
This case macroscopically showed bleeding on both the surface and the inside of the tumor, but histopathological examination failed to reveal evidence of significant disruption of the tumor vessel walls. This finding may indicate that intratumoral bleeding was limited to very minor bleeding. In fact, MRI showed SS but no apparent intraventricular hemorrhage. Vascular degeneration and coexisting cavernous-like malformations may contribute to subependymoma hemorrhage, but the cause of bleeding is not always clear, as in our case.[
Second, MRI T2*WI can identify hemorrhagic changes with high sensitivity and is useful for the detection of bleeding that remains in the lesion, as in this case.[
Our follow-up strategy with MRI T2*WI and timely CSF examination can also be applied to other lesions in the CSF space. Ependymoma is the major tumor of the central nervous system that causes SS, and is occasionally associated with intratumoral hemorrhage in imaging studies.[
CONCLUSION
Some intraventricular tumors can cause SS and nonobstructive hydrocephalus, even if the tumor has not grown. We describe a case of SS and hydrocephalus caused by subependymoma of the lateral ventricles. T2*WI-based radiographic screening and, if necessary, CSF examination might allow the identification of presymptomatic SS and prevent irreversible SS through intraventricular tumor resection. Early detection of SS would be helpful in timely early intervention, contributing to a favorable course in patients with intraventricular lesions.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Abu Rumeileh S, Favoni V, Toni F, Pierangeli G, Oppi F, Calandra-Buonaura G. Superficial siderosis associated with peripheral autonomic failure and tetraventricular hydrocephalus: A case report. Clin Auton Res. 2017. 27: 63-6
2. Akamatsu Y, Utsunomiya A, Suzuki S, Endo T, Suzuki I, Nishimura S. Subependymoma in the lateral ventricle manifesting as intraventricular hemorrhage. Neurol Med Chirurg. 2010. 50: 1020-3
3. Alsereihi M, Turkistani F, Alghamdi F, Baeesa S. Apoplexy of a collision tumour composed of subependymoma and cavernous-like malformation in the lateral ventricle: A case report. Br J Neurosurg. 2019. 33: 581-3
4. Atlas SW, Mark AS, Grossman RI, Gomori JM. Intracranial hemorrhage: Gradient-echo MR imaging at 1.5 T Comparison with spin-echo imaging and clinical applications. Radiology. 1988. 168: 803-7
5. Bi Z, Ren X, Zhang J, Jia W. Clinical, radiological, and pathological features in 43 cases of intracranial subependymoma. J Neurosurg. 2015. 122: 49-60
6. Chen H, Raza HK, Jing J, Ye X, Zhang Z, Hua F. Superficial siderosis of central nervous system with unknown cause: Report of 2 cases and review of the literature. Br J Neurosurg. 2019. 33: 305-8
7. Das A, Ratnagopal P, Puvanendran K, Teo JG. Spinal meningeal melanocytoma with hydrocephalus and intracranial superficial siderosis. Intern Med J. 2001. 31: 562-4
8. Fearnley JM, Stevens JM, Rudge P. Superficial siderosis of the central nervous system. Brain. 1995. 118: 1051-66
9. Hou Z, Wu Z, Zhang J, Zhang L, Tian R, Liu B. Lateral ventricular subependymomas: An analysis of the clinical features of 27 adult cases at a single institute. Neurol India. 2012. 60: 379-84
10. Kandenwein JA, Bostroem A, Feuss M, Pietsch T, Simon M. Surgical management of intracranial subependymomas. Acta Neurochirurg. 2011. 153: 1469-75
11. Katoh N, Yoshida T, Uehara T, Ito K, Hongo K, Ikeda S. Spinal intradural extramedullary cavernous angioma presenting with superficial siderosis and hydrocephalus: A case report and review of the literature. Intern Med (Tokyo Japan). 2014. 53: 1863-7
12. Kumar N, Cohen-Gadol AA, Wright RA, Miller GM, Piepgras DG, Ahlskog JE. Superficial siderosis. Neurology. 2006. 66: 1144-52
13. Kumar N. Superficial siderosis: A clinical review. Ann Neurol. 2021. 89: 1068-79
14. Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK. The 2016 World Health Organization histological classification of tumours of the central nervous system: A summary. Acta Neuropathol. 2016. 131: 803-20
15. Mbadugha T, Ogiwara T, Nagm A, Hasegawa T, Kamiya K, Ohaegbulam S. Superficial siderosis associated with craniopharyngioma. World Neurosurg. 2019. 123: 108-12
16. Rushing EJ, Cooper PB, Quezado M, Begnami M, Crespo A, Smirniotopoulos JG. Subependymoma revisited: Clinicopathological evaluation of 83 cases. J Neurooncol. 2007. 85: 297-305
17. Varma A, Giraldi D, Mills S, Brodbelt AR, Jenkinson MD. Surgical management and long-term outcome of intracranial subependymoma. Acta Neurochirurg. 2018. 160: 1793-9
18. Yoshiki K, Sasagawa Y, Kinoshita M, Furuta T, Tamai S, Sabit H. Superficial siderosis associated with long-term recurrence of pilocytic astrocytoma in an elderly person. World Neurosurg. 2020. 138: 541-4.e541
19. Zhang Q, Xie SN, Wang K, Wang L, Du J, Guo TX. Intratumoral hemorrhage as an unusual manifestation of intracranial subependymoma. World Neurosurg. 2018. 114: e647-53


