

- Department of Neurosurgery, National Institute of Neurology and Neurosurgery Manuel Velasco Suarez, Tlalpan, Mexico City, Mexico
- American British Cowdray Medical Center, Álvaro Obregón, Mexico City, Mexico
- National Institute of Medical Sciences and Nutrition, Mexico.
Correspondence Address:
Luis Alberto Rodriguez-Hernandez, Department of Neurosurgery, National Institute of Neurology and Neurosurgery Manuel Velasco Suarez, Tlalpan, Mexico City, Mexico.
DOI:10.25259/SNI_698_2023
Copyright: © 2024 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: José Guillermo Flores-Vázquez1, Luis Alberto Rodriguez-Hernandez1, Gustavo Becerril-Vega2, Ivan Abdiel Rodríguez-Hernández3, Aldo G. Eguiluz-Melendez3, Oscar Suarez-Rivera1. Technetium-99m-ubiquicidin 29–41 SPECT-CT to detect postsurgical spinal infection: A case report. 26-Jan-2024;15:24
How to cite this URL: José Guillermo Flores-Vázquez1, Luis Alberto Rodriguez-Hernandez1, Gustavo Becerril-Vega2, Ivan Abdiel Rodríguez-Hernández3, Aldo G. Eguiluz-Melendez3, Oscar Suarez-Rivera1. Technetium-99m-ubiquicidin 29–41 SPECT-CT to detect postsurgical spinal infection: A case report. 26-Jan-2024;15:24. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=12726
Date of Submission
21-Aug-2023
Date of Acceptance
23-Dec-2023
Date of Web Publication
26-Jan-2024
Abstract
Background: Postsurgical spinal infections are a severe complication and a challenge to the neurosurgeon due to their complex management. Revision surgeries and the removal of hardware are usually necessary. Recently, advances in nuclear medicine have made it possible to employ radiotracers to identify infections. The radiolabeled antimicrobial peptide technetium-99m-ubiquicidin (99mTc-UBI) (29–41) has been demonstrated to detect bacterial infections. UBI 29–41 is a peptide sequence with selective binding to the anionic cell membrane of bacteria, which has recently been used to differentiate between infection and inflammation. Here, we describe the clinical utility of 99mTc-UBI 29–41 single-photon emission computed tomography-computed tomography (SPECT-CT) in a patient suspected of a postoperative infection.
Case description: A 54-year-old male who presented with conus medullaris syndrome secondary to T12 spondylodiscitis and multiple abscess collections was initially managed with debridement, corpectomy, and minimally invasive lateral instrumentation. The patient developed postsurgical empyema near the surgical site. The image study avoided the need for a second surgery and hardware removal.
Conclusion: The use of 99mTc-UBI 29–41 SPECT-CT served as a tool to avoid a second invasive procedure; instead, conservative management with antibiotics was performed with an effective outcome after two weeks. This radiotracer has utility in cases in which infection is suspected, but the location is not entirely clear, and information is needed to guide the therapeutic approach.
Keywords: Nuclear medicine, Postsurgical infection, Single-photon emission computed tomography, Spinal infection, Ubiquicidin
INTRODUCTION
Postoperative infection constitutes an important complication of spinal surgery due to the need for reoperation and prolonged hospitalization in most cases, increasing health-care costs, morbidity, and morbimortality. When postsurgical spinal infection is suspected, it can be challenging to differentiate between active infection and sterile inflammation. It is also challenging to determine if the infective process has compromised the instrumentation hardware and if it needs to be removed.[
Recently, the radiolabeled antimicrobial peptide technetium-99m-ubiquicidin (99mTc-UBI) (29–41) has been shown to detect bacterial and fungal infections. UBI is a 59-amino acid peptide of human origin, part of our innate immunity against infection. It has minimal cytotoxic and immunogenic properties when radiolabeled with technetium-99m for single-photon emission computed tomography (SPECT) imaging. Its cationic 29–41 amino acid fragment is a specific bacterial-binding domain sequence that links directly to the bacterial anionic cell membrane, allowing it to differentiate between bacterial and sterile inflammation in a suspected infection site.[
Some studies have demonstrated the promising role of 99mTc-UBI (29–41) as a diagnostic tool of high value to differentiate bacterial infection from sterile inflammation in suspected orthopedic implant infections.[
CASE DESCRIPTION
A 54-year-old male presented with intense lumbar pain, erectile dysfunction, urinary and fecal incontinence, hypoesthesia of the genital and perianal regions, and decreased muscle strength and sensitivity in the lower extremities. The patient had a clinical history of hypertensive cardiac disease, chronic kidney disease (KDIGO G3b), proliferative retinopathy, right transmetatarsal amputation due to diabetes mellitus type 2, left radical nephrectomy due to stage III clear cell renal adenocarcinoma (T2bN1M0), and a right renal abscess. On physical examination, he presented with bilateral lower limb strength of 4/5, bilateral decreased patellar and Achilles reflexes, hypoesthesia in S3–S5 dermatomes, abolished cremasteric reflex, urinary retention, and decreased anal sphincter tone on digital rectal examination.
A spine magnetic resonance imaging (MRI) reported T12 spondylodiscitis with decreased height and posterior wall retropulsion, an epidural collection with severe canal narrowing and conus medullaris compression, as well as left parasagittal epidural and retrocrural collections. The patient was admitted for percutaneous drainage of the left paravertebral abscess, which isolated pan-sensitive Staphylococcus aureus. Despite receiving a complete intravenous antibiotic scheme, clinical deterioration, fever, and elevated C-reactive protein occurred. A new MRI and positron emission tomography-computed tomography (CT) reported the persistence of T12 spondylodiscitis with dissemination to soft tissues and T11-L1 vertebral bodies, destruction of both pedicles, intracanalicular extension of prevertebral collections with spinal stenosis, and displacement of the spinal canal. Collections were identified in both psoas muscles and the left diaphragmatic crura.
Surgical treatment was decided; a T12 corpectomy and instrumentation with an expandable cage supplemented by lateral plate and bicortical screws through a minimally invasive lateral approach was performed. Clinical and radiological improvement was observed during the next two weeks. Nevertheless, at the control MRI, after two weeks, a right postero-basal pleural empyema was observed. A enhanced chest CT scan showed right pleural effusion with gas content. Due to the proximity of the empyema to the neurosurgical site, a 99mTc-UBI 29–41 SPECT/CT was performed [
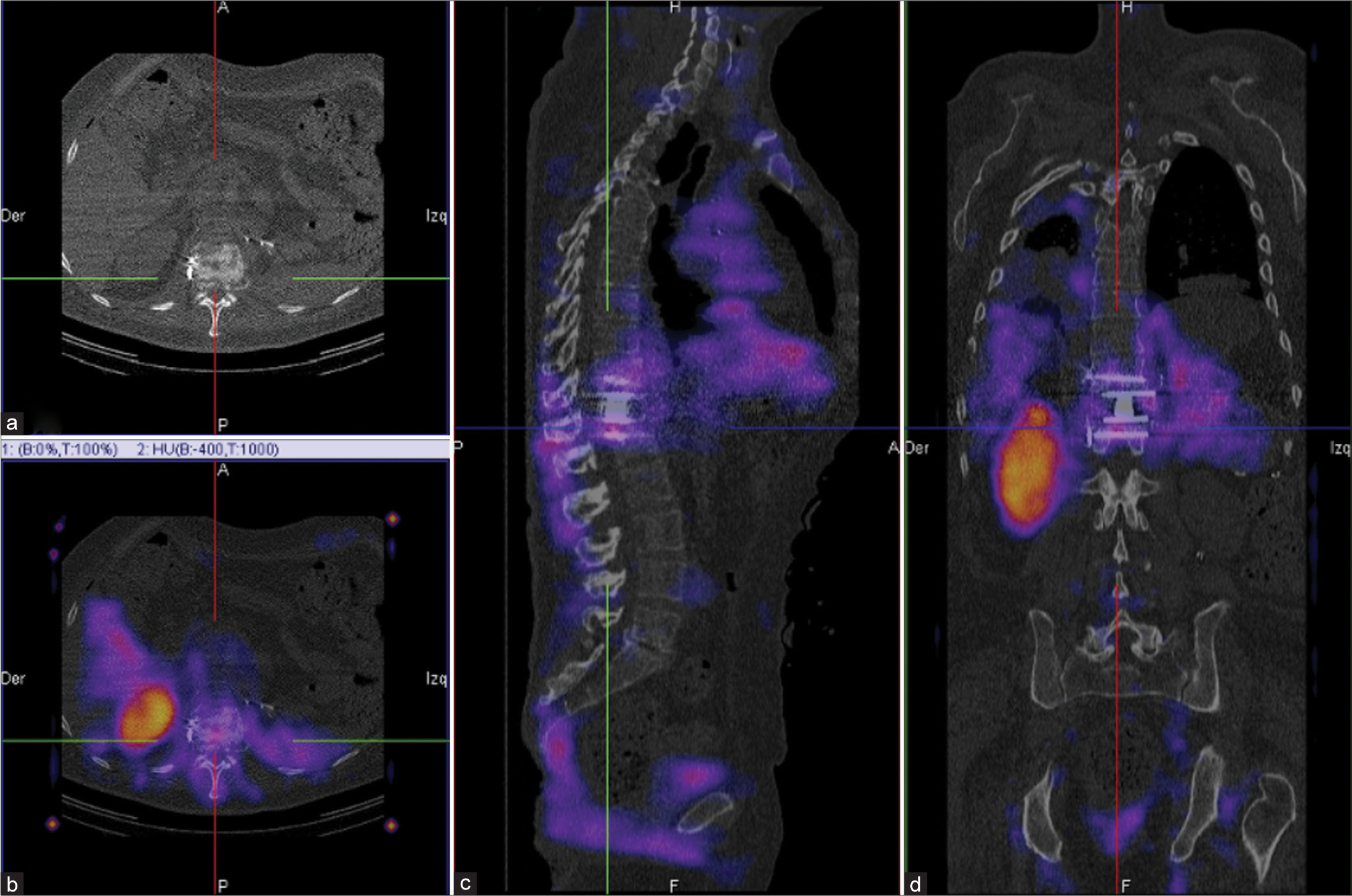
Figure 1:
Due to the proximity of the empyema to the neurosurgical site, a technetium-99m-ubiquicidin (99mTc-UBI) 29–41 single-photon emission computed tomography-computed tomography (SPECT-CT) was performed to rule out infection of the hardware. As suggested by the 4-point scale for uptake of 99mTc-UBI 29–41 at the site of suspected infection (0 = no uptake; 1 = uptake < liver; 2 = uptake > liver; 3 = uptake > kidneys), uptake was classified as 1 point in the hardware area and 2 points in the suspected infection zone. The study reported an infection in the spinal column at T11-L1 that did not compromise the neurosurgical instrumentation. (a) T11 axial CT (b) with uptake of 99mTc-UBI 29–41. (c and d) Uptake of the suspected site of infection compared with kidney uptake in a coronal and sagittal spine 99mTcUBI 29–41 SPECT-CT.
Video 1
CONCLUSION
The use of 99mTc-UBI 29–41 SPECT-CT served as a tool to avoid a second invasive procedure; instead, conservative management with antibiotics was performed with an effective outcome after two weeks. This radiotracer has utility in cases in which infection is suspected, but the location is not entirely clear, and information is needed to guide the therapeutic approach.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Videos available on:
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Beiki D, Yousefi G, Fallahi B, Tahmasebi MN, Gholamrezanezhad A, Fard-Esfahani A. 99mtcubiquicidin [29–41], a promising radiopharmaceutical to differentiate orthopedic implant infections from sterile inflammation. Iran J Pharm Res. 2013. 12: 347
2. Marjanovic-Painter B, Kleynhans J, Zeevaart JR, Rohwer E, Ebenhan T. A decade of ubiquicidin development for PET imaging of infection: A systematic review. Nucl Med Biol. 2023. 116-7: 108307
3. Paez D, Sathekge MM, Douis H, Giammarile F, Fatima S, Dhal A. Comparison of MRI, [18F] FDG PET/CT, and 99mTc-UBI 29-41 scintigraphy for postoperative spondylodiscitis-a prospective multicenter study. Eur J Nucl Med Mol Imaging. 2021. 48: 1864-75
4. Shinto AS, Mukherjee A, Karuppusamy KK, Joseph J, Bhatt J, Korde A. Clinical utility of 99mTc-ubiquicidin (29-41) as an adjunct to bone scan in differentiating infected versus noninfected loosening of prosthesis before revision surgery. Nucl Med Commun. 2017. 38: 285-90

