

- Department of Spine Surgery, University Hospital of Udine, Udine, Italy.
Correspondence Address:
Rossella Rispoli, Department of Spine Surgery, University Hospital of Udine, Udine, Italy.
DOI:10.25259/SNI_638_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Rossella Rispoli, Barbara Cappelletto. Telemedicine in practice: Patient selection and strategies adopted in spinal care during the COVID-19 era and beyond. 26-Aug-2022;13:383
How to cite this URL: Rossella Rispoli, Barbara Cappelletto. Telemedicine in practice: Patient selection and strategies adopted in spinal care during the COVID-19 era and beyond. 26-Aug-2022;13:383. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=11828
Date of Submission
16-Jul-2022
Date of Acceptance
04-Aug-2022
Date of Web Publication
26-Aug-2022
Abstract
Background: The SARS-CoV-2 (COVID-19) pandemic has had a substantial effect on health-care systems around the world. To deal with this challenge, we developed a prospectus design and test a teleconsultation procedure suitable for both diagnostic and therapeutic needs of outpatients in our Spine and Spinal Cord Surgery Units.
Methods: (1) The first 15 patients received in-person and telemedicine visits: Our pilot began with screening protocol that involved 15 patients who received an in-person assessment and a telemedicine consult. The 15 patients who were selected were already known to our unit after having had at least one previous in-person visit. Further, they had to be neurologically intact or have a stable neurological examination. The secondary teleconsultation took place as a synchronous face-to-face communication between the doctor and the patient through a video interface (Lifesize Video Conferencing, Austin, Texas). If the patient demonstrated worsening of symptoms or of their condition, they were rescheduled for an immediate/timely in-person revisit with a spinal physician. (2) Fifty patients were offered telemedicine visits alone: 35 accepted: Next, from 2020 to 2021, we provided a questionnaire to 50 patients, we deemed eligible for teleconsultations: 35 agreed to the teleconsultations, while 15 refused (i.e., selecting direct in-person assessments).
Results: We found a comparable quality for the clinical consultations/assessments provided in-person versus through telemedicine. Further, the additional 35 patients who were positively impressed with the quality of the medical care provided utilizing the telemedicine/remote visits alone.
Conclusion: When pandemic conditions worsen, telemedicine appears to be a viable and important tool/ alternative for spinal surgeons to screen potential patients for treatment/surgery. This preliminary study suggests that a remote examination may be effective, particularly in patients who have previously undergone prior in-person evaluations.
Keywords: COVID-19, Neurological examination, Outpatients, SARS-CoV-2, Spine surgery, Teleconsultation
INTRODUCTION
The COVID-19 pandemic has given rise to a major reorganization of health-care systems throughout the world. As COVID-19 has spread, many countries have experienced human resource constraints and shortages of adequate equipment, and medical personnel, including spine surgeons.[
MATERIALS AND METHODS
First study involving 15 patients undergoing both in-person and telemedicine visits
This study was conducted between November 2020 and January 2021, and involved a comparison of the efficacy of in-person versus telemedicine evaluations of 15 spine patients. To be included in the study, all 15 patients had to have prior in-person evaluations. Further, they had to exhibit no neurological deficits and/or showed no evidence of neurological deterioration. To perform the telemedicine visits, patients typically with their companions were placed in a room with a telephone. They were then connected to the spinal surgeon who was in a separate room. Once the televisit was completed, the quality of generated reports was compared.
Second study involving 35 telemedicine visits alone
We then performed a larger survey of 50 spine patients from 2020 to 2021. All 50 patients received a questionnaire asking if they would participate in a telemedicine consultation with a spinal surgeon (i.e., without an in-person evaluation): 35 agreed to the teleconsultation. They averaged 51 years of age (range 18–96), and notably, 2/3 were under 60 years old [

Eligibility criteria for participants in both studies
Patients eligible for teleconsultation were already known to our unit and had undergone at least one previous in-hospital visit. They also had to exhibit either no neurological deficit or a stable deficit. We identified two groups of patients: (1) postoperative patients or (2) follow-up patients (i.e., whose surgery had been canceled/postponed due to COVID-19 restrictions and who needed to discuss therapies alternative to surgery). All new patients were excluded from the study.
Acceptance questionnaire
We developed a preliminary questionnaire [
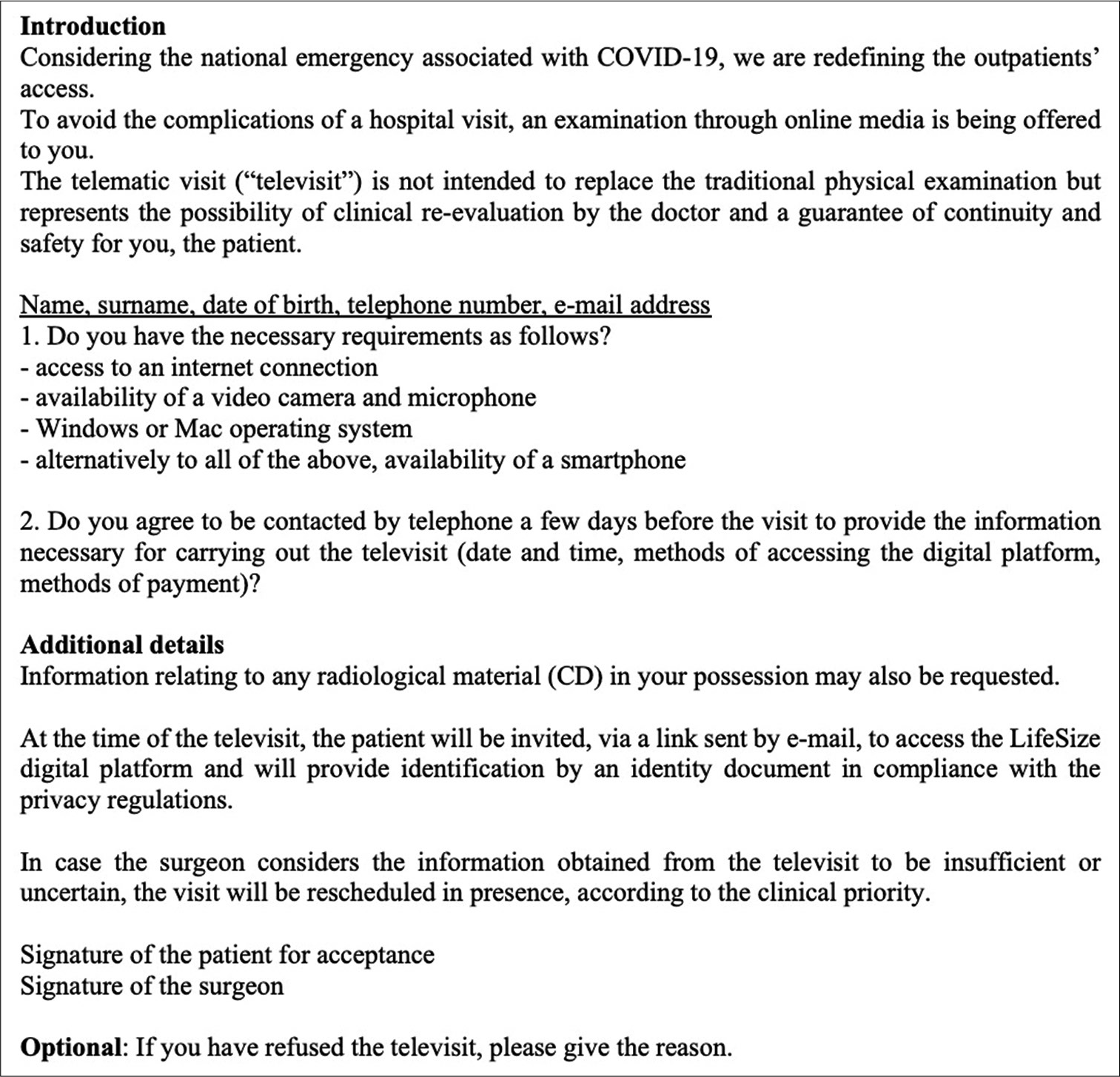
Teleconsultations
Teleconsultation included a synchronous face-to-face communication through audio-video channels between the doctor and the patient in different locations (i.e., using Lifesize Video Conferencing: Austin, Texas). About 1 week before the teleconsultation, the patient was contacted to find out where the radiological examinations had been performed; if performed in a facility outside our access network, the patient was asked to send us the copies of the examination CDs. During and after these visits, we assessed the quality/ efficacy of the telecommunication technology itself.
Instructions to the patient
The patient was instructed to be seated in a room with good lighting, and with no light source (e.g., window) behind their back (i.e., to avoid underexposure/silhouette effect). A frontally positioned light was preferable to enhance visualization during the physical examination. Patients were encouraged to have a family member or friend present during the consultation to assist in the history and physical examination.
Evaluations
Surgeons took routine histories and estimated pain using a numerical rating scale from 0 to 10. Surgeons could inspect the patient by asking them to slowly turn around (i.e., 360°). This allowed for the assessment of deformity, muscle atrophy, kyphosis, etc. Asking the patient to flex, extend and rotate facilitated determination of the range of motion at different spinal levels.
Motor function assessment
Patients were routinely asked to walk to determine motor function in the lower extremities (i.e., walking on heels looking for a foot drop, ability to walk on toes, looking for plantar flexor (PF) weakness) and to walk in a tandem fashion to test balance/gait (i.e., holding or being guarded by a person present or near a wall or furniture). With the patient seated, the deltoid, biceps, brachioradialis, triceps, extensor of the wrist, apposition thumb/index, apposition thumb/pinky, extensor phalanges, and triceps functions in the upper extremities were tested/ observed. This was then followed by testing of the iliopsoas, quadriceps, extensor hallucis longus, dorsiflexors, and PFs. The patients could actually use their opposite hand/leg to evaluate the motor function on the opposite side, or the relative/friend present could perform this, while receiving instructions from the telemedicine spinal surgeon. Thus, the examining spine surgeon could directly observe the motor results.
Sensory function assessment
The spine surgeon could then ask patient or assistant to touch the different dermatomes to determine whether there was any notable change to light touch. They could also be asked about position sensation.
Accuracy of telemedicine evaluations
All these examination maneuvers may be easily accomplished with a relatively adequate degree of accuracy. At the end of our teleconsultation, the examiners assessed the adequacy of the telemedicine appointment. appointment, along with technical problems. In cases where the televisit revealed that the patient’s condition failed to improve or worsened versus a prior in-person examination, the patients were rescheduled for timely in-person visits.
Satisfaction questionnaire after telemedicine visit
At the conclusion of the telemedicine visits, we asked two simple questions: “(1) were you satisfied with this examination procedure? (2) If given the opportunity, would you agree to a future teleconsultation examination?” Following the consultation, the digitally signed report and prescriptions were sent by certified e-mail or by mail.
RESULTS
For the 15 patients, we found that in-person and telemedicine visits offered comparable quality of clinical assessments and treatment. The next 35 patients who agree to televisits, alone were also satisfied (i.e., they answered Yes to both final questions: they were satisfied and, if given the opportunity, they would agree to a future teleconsultation examination).
DISCUSSION
Definition of telemedicine
The COVID-19 pandemic determined radical changes in the organization of the health-care system all over the world. The World Health Organization broadly defines mobile health, or “mHealth,” as “medical and public health practice supported by mobile devices.” The United States government has played an active role in facilitating the rapid roll-out of telehealth programs across the country. Telemedicine use was lower in counties with lower median income, lower population density, less broadband availability, less prepandemic telemedicine use, and fewer COVID-19 cases per capita in the first 30 days of pandemic.[
Difficulty performing a neurological examination
Few studies compared the equivalence of telemedicine versus face-to-face visits. As early as 2016, the American Medical Association initiated a policy requiring medical schools to incorporate telemedicine training into their curriculum. For spine surgeons, the main concern remains the difficulty in performing a detailed neurological examination.[
Telemedicine engagement with remote patients
Telemedicine visits for neurosurgical patients appear promising in the prehospital, inpatient, outpatient, and transfer triage settings, at least in resource-constrained situations.[
Patient preference for in-person assessment
Some patients prefer in-person appointments to virtual appointments. From a patient safety and medicolegal perspective, examiners must be cautious when asking patients to maneuver and the presence of a patient companion is recommended to enhance safety. The video/telemedicine examination has to be accurate and comprehensive to detect potentially significant acute neurological deficits warranting acute hospitalization and/or surgery. Further elderly patients with debilitating spinal pathology may not be able to complete various portions of the physical examination secondary to deconditioning or instability.
CONCLUSION
Telemedicine is an invaluable tool for facilitating safe and timely evaluation and treatment of spinal patients during the COVID pandemic. In the future, telemedicine may continue to be utilized for bringing spine care to patients with less access to spine care.
Declaration of patient consent
Patients’ consent not required as patients’ identities were not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Eichberg DG, Basil GW, Shah AH, Luther EM, Lu VM, Perez-Dickens M. Telemedicine in neurosurgerye. Lessons learned from a systematic review of the literature for the COVID-19 era and beyond. Neurosurgery. 2020. 88: E1-12
2. Franco D, Montenegro T, Gonzalez GA, Hines K, Mahtabfar A, Helgeson MD. Telemedicine for the spine surgeon in the age of COVID-19: Multicenter experiences of feasibility and implementation strategies. Global Spine J. 2021. 11: 608-13
3. Goyal DK, Divi SN, Schroeder GD, Pfeifer R, Canseco JA, Bowles DR. Development of a telemedicine neurological examination for spine surgery: A pilot trial. Clin Spine Surg. 2020. 33: 355-69
4. Greven AC, Rich CW, Malcolm JG, Bray DP, Rodts GE, Refai D. Letter: Neurosurgical management of spinal pathology via telemedicine during the COVID-19 pandemic: Early experience and unique challenges. Neurosurgery. 2020. 87: E192-6
5. Iyer S, Shafi K, Lovecchio F, Turner R, Albert TJ, Kim HJ. The spine physical examination using telemedicine: Strategies and best practices. Global Spine J. 2020. 12: 2192568220944129
6. Kahn EN, La Marca F, Mazzola CA. Neurosurgery and telemedicine in the United States: Assessment of the risks and opportunities. World Neurosurg. 2016. 89: 133-8
7. Lovecchio F, Riew GJ, Samartzis D. Louie PK, Germscheid N, An HS. Provider confidence in the telemedicine spine evaluation: Results from a global study. Eur Spine J. 2021. 30: 2109-23
8. Patel SY, Rose S, Barnett ML, Huskamp HA, Uscher-Pines L, Mehrotra A. Community factors associated with telemedicine use during the COVID-19 pandemic. JAMA Netw Open. 2021. 4: e2110330
9. Piche J, Butt BB, Ahmady A, Patel R, Aleem I. Physical examination of the spine using telemedicine: A systematic review. Global Spine J. 2021. 11: 1142-7
10. Rispoli R, Diamond ME, Balsano M, Cappelletto B. Spine surgery in Italy in the COVID-19 era: Proposal for assessing and responding to the regional state of emergency. World Neurosurg. 2021. 145: e1-6


