

- Department of Neurosurgery, Tokyo Metropolitan Neurological Hospital, Fuchu, Tokyo, Japan.
DOI:10.25259/SNI_460_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Shintaro Arai, Keisuke Takai, Makoto Taniguchi. The algorithm for diagnosis and management of intracranial hypotension with coma: Report of two cases. 29-Aug-2020;11:267
How to cite this URL: Shintaro Arai, Keisuke Takai, Makoto Taniguchi. The algorithm for diagnosis and management of intracranial hypotension with coma: Report of two cases. 29-Aug-2020;11:267. Available from: https://surgicalneurologyint.com/surgicalint-articles/10227/
Date of Submission
22-Jul-2020
Date of Acceptance
07-Aug-2020
Date of Web Publication
29-Aug-2020
Abstract
Background: Spontaneous intracranial hypotension (SIH) is caused by spontaneous cerebrospinal fluid (CSF) leaks that can be treated in most cases with an epidural blood patch (EBP). However, some patients, who develop severe brain sagging, can neurologically deteriorate, and in occasional instances, which become comatose. Here, with the presentation of two cases, and a review of the literature, we have set guidelines for diagnosing SIH along with recommendations for its management.
Case Description: We reviewed two cases of SIH. Both patients became comatose due to a CSF leak associated with a tear in the spinal dura diagnosed on myelo-CT studies. As targeted EBP failed to achieve sustained improvement, direct operative repair of the dural tears was warranted (video presentation).
Conclusion: After reviewing two cases of SIH and the literature, we developed an algorithm for the diagnosis and management of SIH. To avoid deterioration to a comatose status, we recommend the early performance of myelo- CT studies to identify the location of the dural leak, followed by early dural repair.
Keywords: Cerebrospinal fluid leak, Coma, Dural repair, Epidural blood patch
INTRODUCTION
Spontaneous intracranial hypotension (SIH) commonly causes orthostatic headaches. The standard treatment is initial conservative management utilizing an epidural blood patch (EBP).[
CASE REPORTS
Case 1
A 52-year-old woman presented with persistent orthostatic headaches and was diagnosed with SIH. She underwent an MRI that demonstrated deformation/severe sagging of the midbrain with bilateral subdural hematomas [
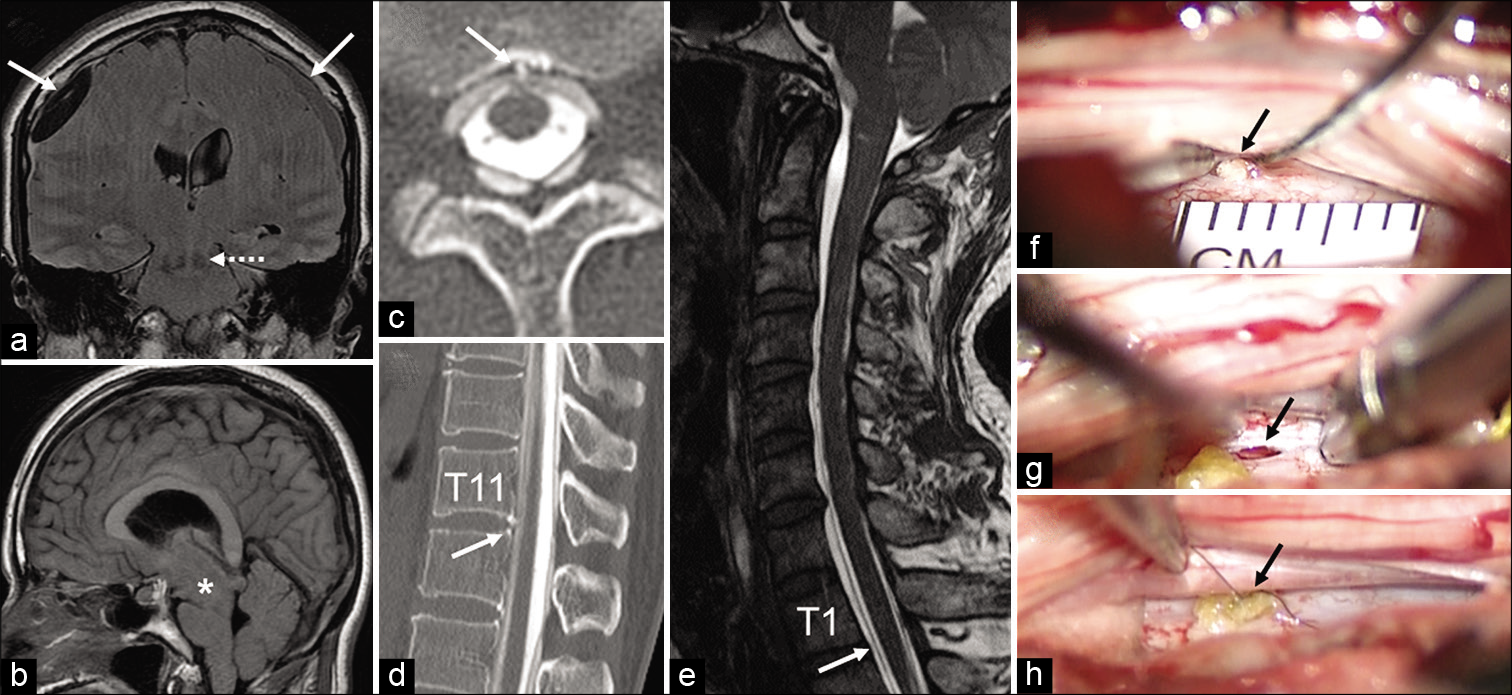
Figure 1:
Case 1: Brain MRI on admission showed bilateral subdural hematoma (a: arrows), downward shifting of the red nucleus (a: dotted arrow), and deformation of the diencephalon-midbrain due to severe brain sagging (b: asterisk). Myelographic CT showed microspurs on the ventral side of the dura at the Th11/12 level (c: arrow) and a leak of the contrast medium out of the dura (d: arrowhead). Case 2: A spinal CSF leak was suspected in spine MRI (e: arrow). A dural tear (2 × 1 mm) and a microspur were found in the ventral dura at the Th1/2 level (f: arrow). The microspur was removed (g: arrow) and the dural tear was sealed with subcutaneous fat tissue (h).
Myelo-CT study
The myelo-CT study revealed a very low opening pressure of just 4 cm H2O, while the myelo-CT itself revealed a micro ventral spur and dural tear at the Th11/12 level [
Case 2
A 61-year-old man with orthostatic headaches was transferred due to altered mental status. The brain MRI also showed deformation of the mesencephalon-midbrain due to severe brain sagging along with bilateral thick subdural hematomas. As a spinal CSF leak was suspected on the cervicothoracic MRI [

DISCUSSION
In general, SIH often resolves with conservative treatment, particularly with the performance of EBP.[
Treatment alternatives for SIH
There are a variety of methods for treating SIH. Nonsurgical treatment, includes nontargeted lumbar EBP,[
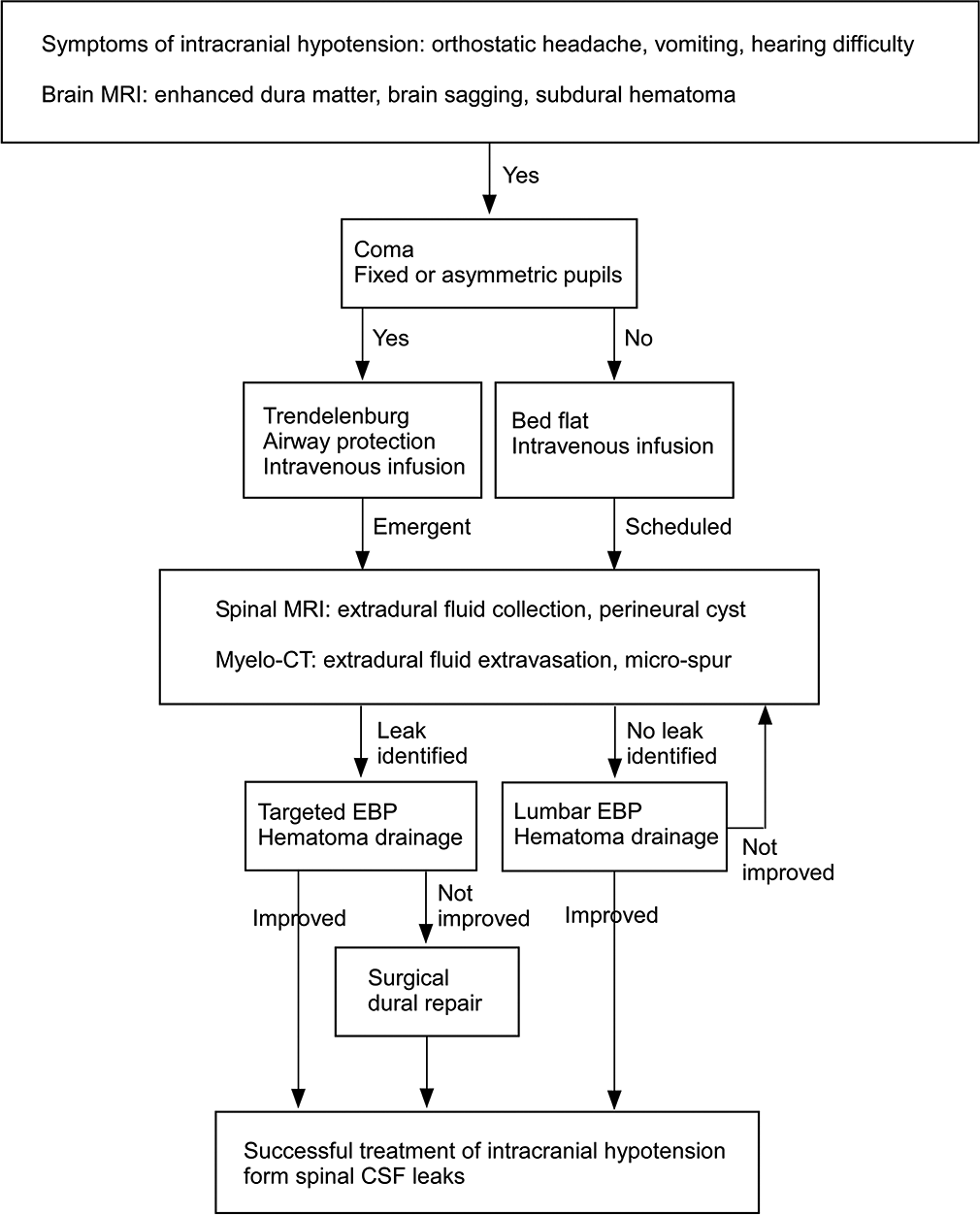
Algorithm for the diagnosis and management of SIH
Here, we propose an algorithm for the diagnosis and management of SIH [
CONCLUSION
The clinical decision-making algorithm presented here may help neurologists/neurosurgeons who diagnose and treat this rare condition.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
Dr. Shintaro Arai and Dr. Keisuke Takai contributed equally to this work and share first authorship.
References
1. Collange O, Wolff V, Cebula H, Pradignac A, Meyer A, Kindo M. Spontaneous intracranial hypotension: An etiology for consciousness disorder and coma. A A Case Rep 2016. ;. 7: 207-11
2. Davidson B, Nassiri F, Mansouri A, Badhiwala JH, Witiw CD, Shamji MF. Spontaneous intracranial hypotension: A review and introduction of an algorithm for management. World Neurosurg. 2017. 101: 343-9
3. Ghavanini AA, Scott CA, Chan DK, Tang-Wai DF. Management of patients with spontaneous intracranial hypotension causing altered level of consciousness: Report of two cases and review of literature. Cephalalgia. 2013. 33: 43-51
4. Takai K, Taniguchi M. Intracranial hypotension with coma: Microsurgical repair of a spinal ventral dural tear and drainage of subdural hematoma with intracranial pressure monitoring. World Neurosurg. 2018. 118: 269-73
5. Yoshida H, Takai K, Taniguchi M. Leakage detection on CT myelography for targeted epidural blood patch in spontaneous cerebrospinal fluid leaks: Calcified or ossified spinal lesions ventral to the thecal sac. J Neurosurg Spine. 2014. 21: 432-41


