

- Seattle Science Foundation, Seattle, Washington,
- Department of Medicine, University of Illinois College of Medicine, Chicago, Illinois,
- Department of Medicine, Western University of Health Sciences College of Osteopathic Medicine of the Pacific-Northwest, Lebanon, Oregon,
- Swedish Medical Center, Swedish Neuroscience Institute, Washington,
- Department of Trauma Surgery, BG University Hospital Bergmannsheil, Ruhr University Bochum, Bochum, Germany.
- Hansjörg Wyss Hip and Pelvic Center, Swedish Hospital, Seattle, Washington,
- Riverside University Health System Medical Center, Moreno Valley, California, United States,
Correspondence Address:
Darius Ansari
Seattle Science Foundation, Seattle, Washington,
Swedish Medical Center, Swedish Neuroscience Institute, Washington,
DOI:10.25259/SNI_46_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Darius Ansari, Halle E. K. Burley, Alexander von Glinski, Christopher Elia, Jens R. Chapman, Rod J. Oskouian. The new onset of dysphagia four years after anterior cervical discectomy and fusion: Case report and literature review. 28-Feb-2020;11:32
How to cite this URL: Darius Ansari, Halle E. K. Burley, Alexander von Glinski, Christopher Elia, Jens R. Chapman, Rod J. Oskouian. The new onset of dysphagia four years after anterior cervical discectomy and fusion: Case report and literature review. 28-Feb-2020;11:32. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=9886
Date of Submission
02-Feb-2020
Date of Acceptance
13-Feb-2020
Date of Web Publication
28-Feb-2020
Abstract
Background:Dysphagia is a common complication immediately following anterior cervical spine surgery. However, its onset more than 1-year postoperatively is rare.
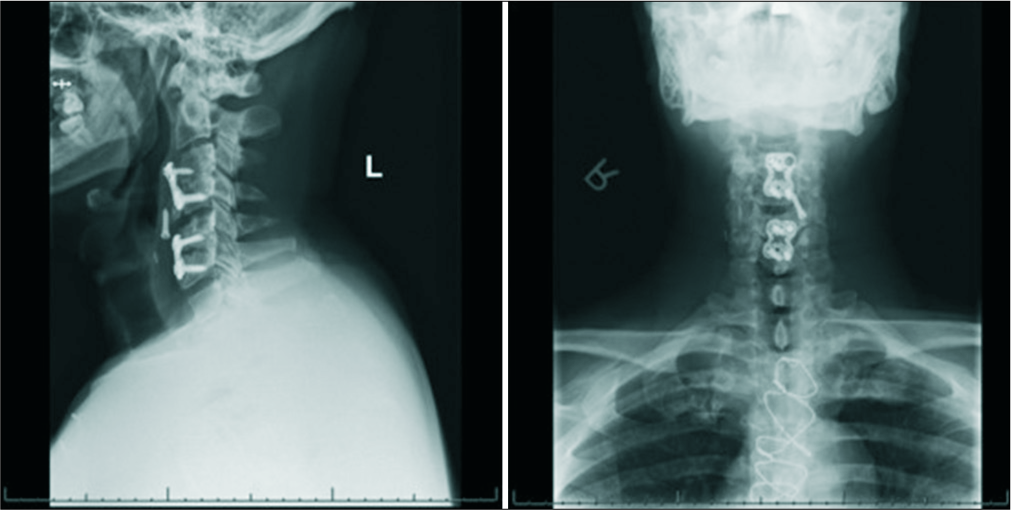
Case Description:A 45-year-old male initially underwent a C3-4 and C5-6 anterior cervical discectomy and fusion (ACDF). At age 49, 4 years later, he presented with worsening dysphagia accompanied by neck and right upper extremity pain. Radiographs demonstrated an extruded left C3 screw, which had migrated into the prevertebral soft tissues at the C4-C5 level; there was also loosening of the right C3 screw. The subsequent barium swallow study revealed that the screw was embedded in the pharyngeal wall. The patient required a two-stage operation; first, to remove the anterior instrumentation, and second, to perform a posterior instrumented C2-T2 fusion.
Conclusion:A barium swallow study and other dynamic imaging are a valuable component of the diagnostic workup and therapeutic intervention to evaluate the delayed onset dysphagia following an ACDF.
Keywords: Anterior cervical discectomy and fusion, Complications, Delayed onset dysphagia, Hardware failure
INTRODUCTION
Anterior cervical discectomy and fusions (ACDF) complications, include dysphagia (most common), followed by recurrent laryngeal nerve injury, Horner syndrome, esophageal perforation, infection, and graft extrusion. The prevalence of dysphagia 1–6 weeks postoperatively ranges from 28% to 57%.[
Here, we present the new-onset dysphagia in a 49-year-old male, 4 years following a 2-level C3-C4/C5-C6 ACDF. Symptoms were attributed to a left C3 screw extrusion into the posterior pharyngeal soft tissue with the loosening of the right C3 screw. The patient required anterior resection of instrumentation followed by a posterior C2T2 fusion. The point of this study was to highlight that the new-onset dysphagia occurring even years after an ACDF should be carefully evaluated for instrumentation failure (e.g., perforation of the pharyngeal wall).
CASE REPORT
At age 45, the patient with a history of renal insufficiency, had a C3-4 and C5-6 ACDF. Four years later, he prior presented with neck/right upper extremity pain, and worsening dysphagia. The physical exam revealed 3/5 deltoid strength on the right side, but was otherwise unremarkable.
Diagnostic studies
Lateral radiographs of the cervical spine revealed an extruded left C3 screw, which had migrated into the prevertebral soft tissues at the C4-5 level, as well as loosening of the right C3 screw [
Surgery
With the help of an otolaryngologist ear, nose, and throat specialist, the left C3 screw was removed from within the left lateral pharyngeal wall; scar tissue on the posterior aspect of the screw pocket was opened, and the inflammatory capsule surrounding it was excised without evidence of esophageal perforation. Next, the spine surgeons removed the anterior instrumentation (e.g., plate C3-C4/C5-C6), followed by placement of a new interbody structural allograft at C4-5 with a new plate, and posteriorly, and instrumented fusion from C2-T2. The patient was discharged without complaints.
DISCUSSION
Following anterior-approach cervical operations, many patients experience some degree of dysphagia, which is almost always self-limiting and may take up to 2 years to resolve.[
To assess dysphagia, dynamic imaging studies include modified barium swallow study and fiberoptic endoscopic evaluation of swallowing.
Delayed-onset dysphagia may be variously attributed to: mass effect exerted on the posterior laryngeal wall by an abscess, delayed instrumentation failure with pharyngeal versus esophageal defect,[
Radiographic recommendations to evaluate delayed onset dysphagia
We recommend preoperative dynamic imaging and intraoperative fluoroscopy for all cases of delayed postoperative dysphagia, especially those with potential for or known screw migration/instrumentation failure. A multidisciplinary approach with an otolaryngologist may be valuable to ensure safe instrumentation mobilization and removal, as well as to prepare for a possible esophageal repair.[
CONCLUSION
Anterior cervical instrumentation failure should be considered when patients who previously underwent an ACDF newly present with dysphagia months to years later; the preoperative workup should include X-rays, magnetic resonance imaging, computed tomography, and videofluoroscopic swallowing studies.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos available on:
www.surgicalneurologyint.com
References
1. Anderson KK, Arnold PM. Oropharyngeal dysphagia after anterior cervical spine surgery: A review. Global Spine J. 2013. 3: 273-86
2. Christiano LD, Goldstein IM. Late prevertebral abscess after anterior cervical fusion. Spine (Phila Pa 1976). 2011. 36: E798-802
3. Fryer C, Tan HE, Bakmeedeniya R, Friedland PL. Late-onset dysphagia from hardware migration after anterior cervical discectomy and fusion: An unusual cause and review of literature. Clin Med Insights Ear Nose Throat. 2019. 12: 1179550619881131-
4. Lee MJ, Bazaz R, Furey CG, Yoo J. Risk factors for dysphagia after anterior cervical spine surgery: A two-year prospective cohort study. Spine J. 2007. 7: 141-7
5. Min Y, Kim WS, Kang SS, Choi JM, Yeom JS, Paik NJ. Incidence of dysphagia and serial videofluoroscopic swallow study findings after anterior cervical discectomy and fusion: A prospective study. Clin Spine Surg. 2016. 29: E177-81
6. Smith-Hammond CA, New KC, Pietrobon R, Curtis DJ, Scharver CH, Turner DA. Prospective analysis of incidence and risk factors of dysphagia in spine surgery patients: Comparison of anterior cervical, posterior cervical, and lumbar procedures. Spine (Phila Pa 1976). 2004. 29: 1441-6
7. Vanderveldt HS, Young MF. The evaluation of dysphagia after anterior cervical spine surgery: A case report. Dysphagia. 2003. 18: 301-4
8. Winslow CP, Winslow TJ, Wax MK. Dysphonia and dysphagia following the anterior approach to the cervical spine. Arch Otolaryngol Head Neck Surg. 2001. 127: 51-5


Denise Purcell
Posted January 10, 2023, 10:10 am
I am a patient who had anterior and posterior neck laminectomy and hardware placed from beginning to c7.
I had this done 2010. Since then I have had trouble slowing and coughing to the point my throat feels like it’s closing and I can’t catch my breath.this has only gotten worse.i stumbled on a few articles including this one referring to this problem after surgery and years later.i was never informed. I td my Dr and wa dismissed. Now I know there is a real problem and possibly why. Any suggestion?