

- Department of Neurosurgery, Kesennuma City Hospital, Kesennuma, Miyagi,
- Department of Radiological Technology, Sapporo City General Hospital, Sapporo, Hokkaido, Japan.
- Department of Neurosurgery, Tohoku University Graduate School of Medicine, Sendai, Miyagi,
Correspondence Address:
Norio Narita
Department of Neurosurgery, Tohoku University Graduate School of Medicine, Sendai, Miyagi,
DOI:10.25259/SNI_329_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Masahito Katsuki1, Norio Narita1, Dan Ozaki1, Yoshimichi Sato1, Saki Iwata2, Teiji Tominaga3. Three tesla magnetic resonance angiography with ultrashort echo time describes the arteries near the cerebral aneurysm with clip and the peripheral cerebral arteries. 01-Aug-2020;11:224
How to cite this URL: Masahito Katsuki1, Norio Narita1, Dan Ozaki1, Yoshimichi Sato1, Saki Iwata2, Teiji Tominaga3. Three tesla magnetic resonance angiography with ultrashort echo time describes the arteries near the cerebral aneurysm with clip and the peripheral cerebral arteries. 01-Aug-2020;11:224. Available from: https://surgicalneurologyint.com/surgicalint-articles/10178/
Date of Submission
02-Jun-2020
Date of Acceptance
01-Jul-2020
Date of Web Publication
01-Aug-2020
Abstract
Background: The assessment of the clipped cerebral aneurysm and the cerebral arteries after the treatment of subarachnoid hemorrhage (SAH) is important to find aneurysm regrowth or postoperative cerebral vasospasm. Usually, contrast-enhanced computed tomography angiography is performed for the evaluation of the arteries, but it has side effects of contrast medium. Time-of-flight magnetic resonance angiography (MRA) is a fast and non-invasive method, but clip-induced artifact limits assessment of the artery in the vicinity of the clip. 1.5T MRA with ultrashort echo time (UTE) reduces metal artifact, but the obtained image is too rough to evaluate the aneurysm remnant, and the description range is too narrow to assess the cerebral vasospasm. We routinely use SIGNA Pioneer 3.0T (GE Healthcare Life Sciences, Buckinghamshire, England) and perform SILENT SCAN with UTE-MRA for the postoperative assessment of the clipped aneurysm and cerebral arteries for SAH patients treated by clipping. It has better image quality and describes arteries with a wide description range, so it possesses the potential to overcome the disadvantages of 1.5T UTE-MRA.
Case Description: We presented a representative SAH patient who postoperatively underwent 3.0T UTE- MRA after clipping. The artery near the clipped aneurysm was evaluated in detail, and the cerebral arteries were described from the main trunk to the peripheral parts with a wide description range, which enabled the assessment of cerebral vasospasm.
Conclusion: 3.0T UTE-MRA may be helpful for the usual assessment of the arteries after clipping and cerebral vasospasm in the future.
Keywords: 3 tesla, Cerebral aneurysm, Clipping, Magnetic resonance angiography, Ultrashort echo time
IMAGE REPORT
Background
The assessment of the clipped cerebral aneurysm and the cerebral arteries after the treatment of subarachnoid hemorrhage (SAH) is important to find aneurysm regrowth or postoperative cerebral vasospasm. Of course, non-invasive methods are better for the assessment of the arteries after clipping. Usually, contrast-enhanced computed tomography angiography (CTA) is performed for the evaluation of clipped cerebral aneurysm[
3.0T UTE-MRA has a potential to overcome the problem which 1.5T UTE-MRA has because its image is not so rough, and its description range is wider. However, only Takubo et al. reported the usefulness of 3.0T UTE-MRA for the assessment of clipped aneurysm,[
CASE DESCRIPTION
An 80-year-old woman developed SAH (Hunt and Konik Grade II) due to a ruptured aneurysm at the anterior communicating artery (ACoA). The preoperative CTA revealed the 4.0 mm aneurysm [arrowhead,
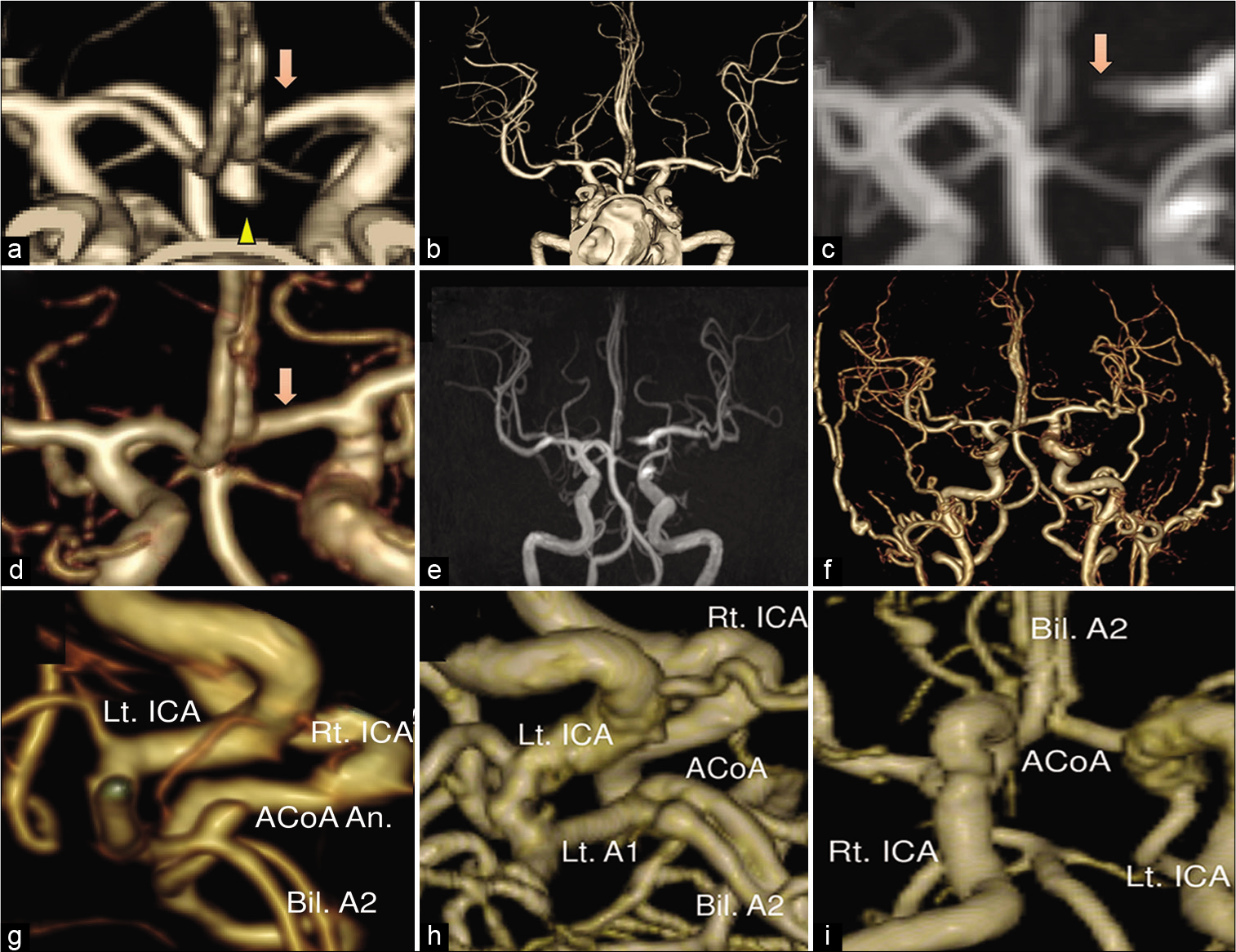
Figure 1:
The preoperative computed tomography angiography (CTA) revealed the 4.0 mm aneurysm at the anterior communicating artery (ACoA) (arrowhead, a) and the A1 portion of the anterior cerebral artery (arrow, a) with a wide description range from the main trunk to the peripheral parts (b). On the 5 postoperative day, 3.0T time of flight magnetic resonance angiography (TOF-MRA) did not describe the left A1 (arrow, c), but 3.0T ultrashort echo time MRA (UTE-MRA) described it (arrow, d). Both sequences described the cerebral arteries from the main trunk to the peripheral parts with a wide description range, which enabled the assessment of cerebral vasospasm (e and f). (g) is an operative image reconstructed using the preoperative CTA. (h) is that made by postoperative 3.0T UTE-MRA. (i) is a view from the bottom reconstructed using the postoperative 3.0T UTE-MRA, and it revealed the arteries in the vicinity of the clip, the bilateral A1, A2 portions, and the ACoA, in detail. ACoA: anterior communicating artery, Bil: bilateral, ICA: internal carotid artery.
DISCUSSION
This is the first report on the clinical usefulness of 3.0T UTE-MRA for postclipping assessment on the cerebral arteries. Compared to CTA, UTE-MRA is less invasive and fast, but its image quality is not up to the CTA. Compared to TOF-MRA, only UTE-MRA reveals the artery in the vicinity of a clip, but both sequences describe cerebral arteries from the main trunk to the peripheral parts. However, the total required time is longer in UTE-MRA than that in TOF-MRA because UTE-MRA needs arterial spin labeling (ASL) preparation,[
CONCLUSION
3.0T UTE-MRA may be helpful for the usual assessment of the arteries after clipping and cerebral vasospasm.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Becker RL, Norfray JF, Teitelbaum GP, Bradley WG, Jacobs JB, Wacaser L. MR imaging in patients with intracranial aneurysm clips. AJNR Am J Neuroradiol. 1988. 9: 885-9
2. Healthcare GE. Available from: http://www3.gehealthcare.co.jp/ja-jp/products_and_service/imaging/magnetic_resonance_imaging/signa_pioneer [Last accessed on 2020 May 22].
3. Gönner F, Lövblad KO, Heid O, Remonda L, Guzman R, Barth A. Magnetic resonance angiography with ultrashort echo times reduces the artefact of aneurysm clips. Neuroradiology. 2002. 44: 755-8
4. Irie R, Suzuki M, Yamamoto M, Takano N, Suga Y, Hori M. Assessing blood flow in an intracranial stent: A feasibility study of MR angiography using a silent scan after stent-assisted coil embolization for anterior circulation aneurysms. AJNR Am J Neuroradiol. 2015. 36: 967-70
5. Katsuki M, Kakizawa Y, Yamamoto Y, Nishikawa A, Wada N, Uchiyama T. Magnetic resonance angiography with ultrashort echo time evaluates cerebral aneurysm with clip. Surg Neurol Int. 2020. 11: 65
6. Kiriki M, Jomoto W, Ikeda T, Kotoura N. Imaging parameter optimization of 3D phase contrast-MRA to reduce susceptibility-artifact and radiofrequency-shielding around the intracranial stent. Nihon Hoshasen Gijutsu Gakkai Zasshi. 2018. 74: 1293-301
7. Koch KM, Hargreaves BA, Pauly KB, Chen W, Gold GE, King KF. Magnetic resonance imaging near metal implants. J Magn Reson Imaging. 2010. 32: 773-87
8. Robson MD, Gatehouse PD, Bydder M, Bydder GM. Magnetic resonance: An introduction to ultrashort TE (UTE) imaging. J Comput Assist Tomogr. 2003. 27: 825-46
9. Schmalbrock P, Yuan C, Chakeres DW, Kohli J, Pelc NJ. Volume MR angiography: Methods to achieve very short echo times. Radiology. 1990. 175: 861-65
10. Takano N, Suzuki M, Irie R, Yamamoto M, Hamasaki N, Kamagata K. Usefulness of non-contrast-enhanced MR angiography using a silent scan for follow-up after Y-configuration stentassisted coil embolization for basilar tip aneurysms. Am J Neuroradiol. 2017. 38: 577-81
11. Takubo S, Kawasaki K, Nagatari T, Matsumoto M, Kageyama T. Clinical usefulness of ultra-short TE MRA for follow-up imaging after cerebral aneurysm clipping. Nihon Hoshasen Gijutsu Gakkai Zasshi. 2020. 76: 177-84
12. Tomura N, Kokubun M, Horiuchi K, Watanabe Z. Comparison of TOF-MRA and silent scan-MRA in depicting cerebral arteries in patients with moyamoya disease. Acta Radiol. 2019. 60: 1321-8
13. Tomura N, Saginoya T, Kokubun M, Horiuchi K, Watanabe Z. Comparison of time-of-flight-magnetic resonance angiography from silent scan magnetic resonance angiography in depiction of arteriovenous malformation of the Brain. J Comput Assist Tomogr. 2019. 43: 943-7
14. Van Loon JJ, Yousry TA, Fink U, Seelos KC, Reulen HJ, Steiger HJ. Postoperative spiral computed tomography and magnetic resonance angiography after aneurysm clipping with titanium clips. Neurosurgery. 1997. 41: 851-6

