

- Department of Cerebrovascular Surgery, International Medical Center, Saitama Medical University,
- Department of Neuroendovascular Surgery, International Medical Center, Saitama Medical University, Hidaka, Saitama.
Correspondence Address:
Tomoya Kamide
Department of Cerebrovascular Surgery, International Medical Center, Saitama Medical University,
DOI:10.25259/SNI_493_2019
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Shinya Tabata, Tomoya Kamide, Toshiki Ikeda, Yuichiro Kikkawa, Shigen Kasakura, Shinya Kohyama, Hiroki Kurita. Trans-lamina terminalis approach assisted by endovascular temporary basilar artery occlusion for high-positioned, recurrent, basilar tip aneurysm: A technical case report. 24-Jan-2020;11:13
How to cite this URL: Shinya Tabata, Tomoya Kamide, Toshiki Ikeda, Yuichiro Kikkawa, Shigen Kasakura, Shinya Kohyama, Hiroki Kurita. Trans-lamina terminalis approach assisted by endovascular temporary basilar artery occlusion for high-positioned, recurrent, basilar tip aneurysm: A technical case report. 24-Jan-2020;11:13. Available from: https://surgicalneurologyint.com/surgicalint-articles/9856/
Date of Submission
22-Sep-2019
Date of Acceptance
07-Jan-2020
Date of Web Publication
24-Jan-2020
Abstract
Background: Coil embolization is increasingly becoming the surgical intervention of choice for cerebral aneurysms, particularly for those in the posterior circulation. However, in cases where it is difficult to perform coil embolization, microsurgical clipping is still required.
Case Description: We present a case of a high-positioned, ruptured, recurrent basilar tip aneurysm treated with a combination of microsurgical clipping through the trans-lamina terminalis approach and endovascular procedure. The technical considerations of this approach are discussed.
Conclusion: Microsurgical clipping through the trans-lamina terminalis approach combined with an endovascular technique can be effective for basilar tip aneurysms. This approach is particularly useful for high-positioned, small, anterior projective aneurysms and cases with dilation of the third ventricle due to hydrocephalus or clot.
Keywords: Basilar artery, Hybrid surgery, Intracranial aneurysm, Terminalis approach, Trans-lamina
INTRODUCTION
Executing a microsurgical approach to resolve a high-positioned basilar tip aneurysm is one of the most difficult operations in the field of neurosurgery. Coil embolization has facilitated the procedure and has thus become an increasingly widespread treatment option; however, in cases where endovascular treatment is not suitable, microsurgical clipping of the aneurysm is necessary. Herein, we describe a case of a high-positioned, recurrent basilar tip aneurysm treated through the trans-lamina terminalis approach assisted by endovascular temporary basilar artery occlusion.
CASE REPORT
An 80-year-old man presented with a severe headache of sudden onset and nausea. His medical history included the surgical clipping of a ruptured basilar tip aneurysm and unruptured right internal carotid-posterior communicating aneurysm through the right orbitozygomatic approach 14 years ago. On admission, he exhibited a mild disturbance of consciousness, with a Glasgow Coma Scale score of 14. Computed tomography (CT) revealed clots in all ventricles [
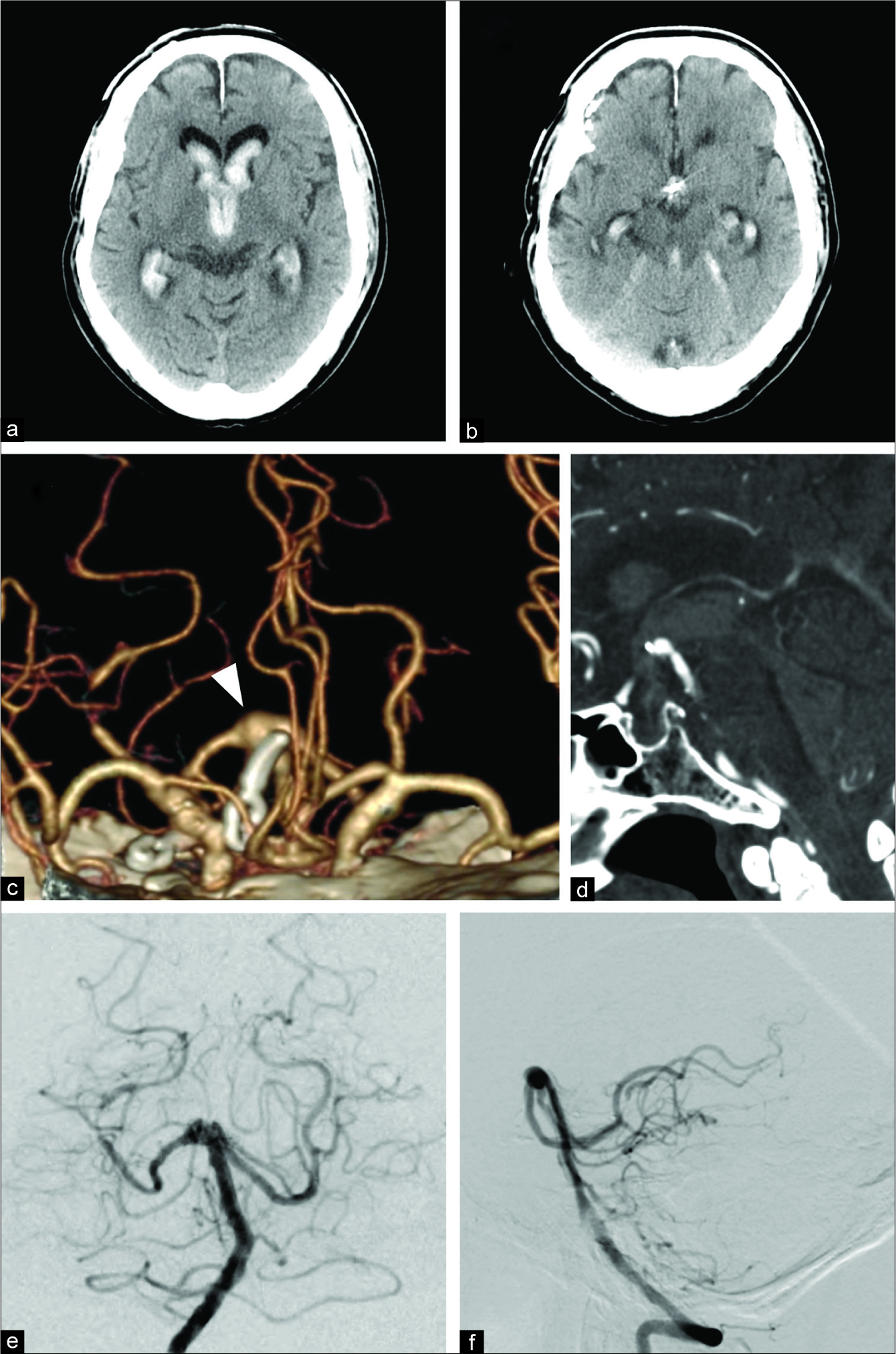
Figure 1:
Preoperative images. (a and b) Computed tomography (CT) showing a clot in the third ventricle surrounding the previously applied clip; (c) three-dimensional (3D) CT angiogram showing a tiny bulge on the right side of the previously applied clip (arrow); (d) sagittal view of the 3D CT angiogram showing the distance between the basilar tip and the posterior clinoid process: 15 mm; (e and f) preoperative digital subtraction angiogram showing a tiny bulge on the right side of the previously applied clip and no other bleeding source.
Considering the shape of the small bulge and the lack of space into which the coil could be inserted, the use of coil embolization, even in conjunction with the stent-assisted technique, was precluded. Several microsurgical approaches including the pterional, subtemporal, temporopolar, and orbitozygomatic approaches were thought to be impractical due to the topography of the aneurysm and the previously applied clip. We selected the trans-lamina terminalis approach. To prepare for a premature rupture, we decided to incorporate the endovascular technique in the hybrid operation room (OR). Through bifrontal craniotomy, the interhemispheric fissure was widely dissected. Subsequently, a 4-Fr guiding sheath was inserted through the right femoral artery and was advanced to the left vertebral artery. A balloon microcatheter (HyperForm®, 7 mm × 7 mm) was placed at the basilar artery for proximal flow control. Opening of the third ventricle was performed through the trans-lamina terminalis approach [

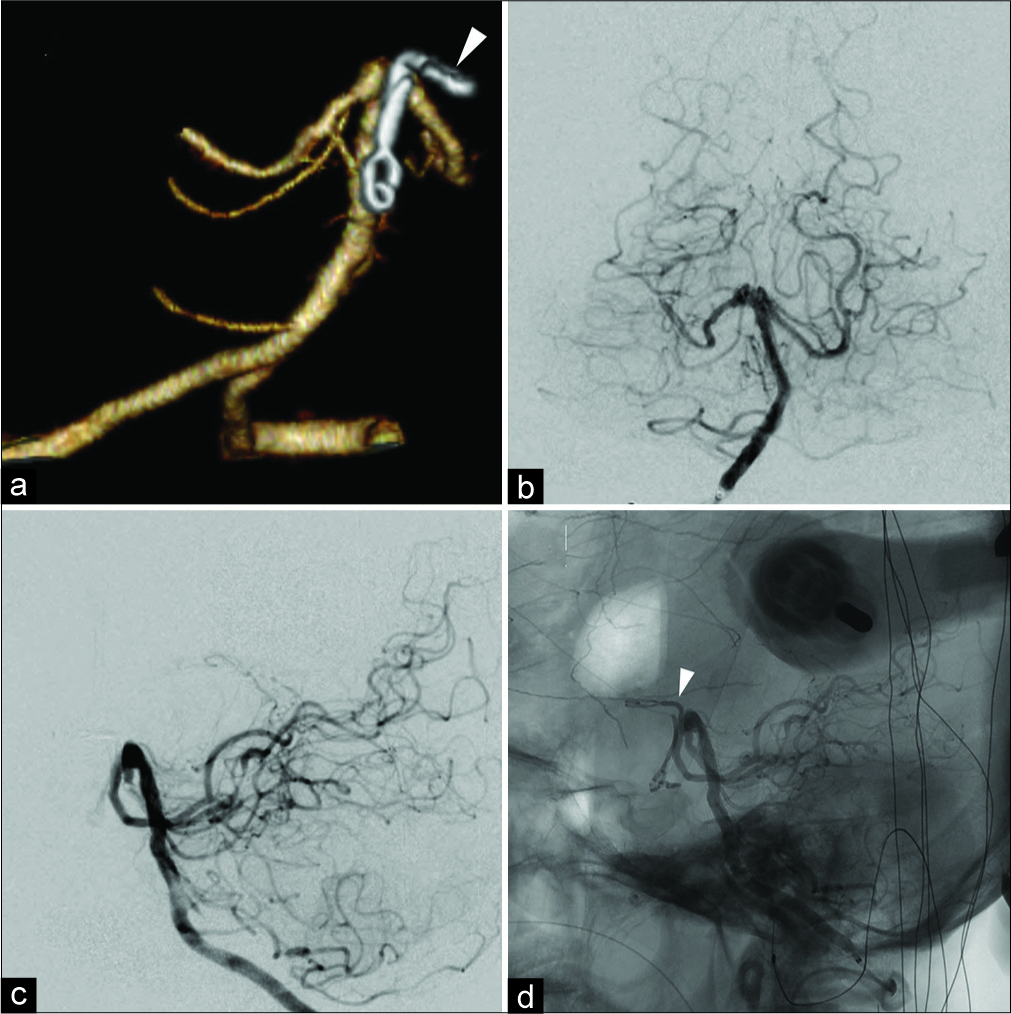
Figure 2:
Intraoperative images. (a) Lamina terminalis; (b) entrance into the third ventricle after the lamina terminalis was opened; (c) after the third ventricle floor was opened, a red friable bulge on the right side of the previous clip was confirmed. A thrombus on top of the tiny bulge was observed and confirmed to be a bleeding source; (d) L-shaped clip applied under the previous clip.
The patient’s postoperative course was uneventful [
DISCUSSION
Basilar tip aneurysms have traditionally been the most difficult cerebral aneurysms to clip, and nowadays, coil embolization has become an increasingly common treatment option. However, in this case, the bleeding source was only a small bulge, and there was no space for coil insertion even with the use of an adjunctive technique; thus, endovascular treatment was impossible. The major surgical interventions include the pterional and subtemporal approaches,[
Trans-lamina terminalis approach is rarely selected for basilar tip aneurysms; only six cases have been reported.[
Transient hypothermia, endocrine disturbances, and memory impairment may occur following this approach.[
Furthermore, the trans-lamina terminalis approach involves the risk of a premature rupture of the aneurysm without safe control of the proximal segment of the artery. To overcome this disadvantage, we combined this surgical approach with endovascular proximal control by placing and inflating a balloon microcatheter in the hybrid OR, which is fully equipped with digital subtraction angiography. There are few reports on the use of temporary balloon occlusion during surgical intervention for vertebrobasilar aneurysms.[
To the best of our knowledge, this is the first report of a combined application of the trans-lamina terminalis approach with an endovascular technique. As this case demonstrates, the recent development of the hybrid OR has provided new strategies for neurosurgeons to approach complex basilar tip aneurysms.[
CONCLUSION
Microsurgical clipping through the trans-lamina terminalis approach combined with an endovascular technique can be effective for basilar tip aneurysms. This approach is particularly useful for high-positioned, small, anterior projective aneurysms and cases with dilation of the third ventricle due to hydrocephalus or clot.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bailes JE, Deeb ZL, Wilson JA, Jungreis CA, Horton JA. Intraoperative angiography and temporary balloon occlusion of the basilar artery as an adjunct to surgical clipping: Technical note. Neurosurgery. 1992. 30: 949-53
2. Canbolat A, Onal C, Kiriş T. A high-position basilar top aneurysm approached via third ventricle: Case report. Surg Neurol. 1993. 39: 196-9
3. Drake CG. Bleeding aneurysms of the basilar artery. Direct surgical management in four cases. J Neurosurg. 1961. 18: 230-8
4. Fandino J, Taussky P, Marbacher S, Muroi C, Diepers M, Fathi AR. The concept of a hybrid operating room: Applications in cerebrovascular surgery. Acta Neurochir Suppl. 2013. 115: 113-7
5. Fong YW, Hsu SK, Huang CT, Hsieh CT, Chen MH, Huang JS. Impact of intraoperative 3-dimensional volume-rendering rotational angiography on clip repositioning rates in aneurysmal surgery. World Neurosurg. 2018. 114: e573-80
6. Fujitsu K, Kuwabara T. Zygomatic approach for lesions in the interpeduncular cistern. J Neurosurg. 1985. 62: 340-3
7. Hidaka T, Ikawa F, Hamasaki O, Kurokawa Y, Yonezawa U, Kurisu K. A case of transient hypothermia after trans-lamina terminalis and third ventricle clipping of an extremely high-position basilar tip aneurysm. SAGE Open Med Case Rep. 2015. 3: 2050313X15578318-
8. Ikeda K, Yamashita J, Hashimoto M, Futami K. Orbitozygomatic temporopolar approach for a high basilar tip aneurysm associated with a short intracranial internal carotid artery: A new surgical approach. Neurosurgery. 1991. 28: 105-10
9. Jeon HJ, Lee JY, Cho BM, Yoon DY, Oh SM. Four-year experience using an advanced interdisciplinary hybrid operating room: Potentials in treatment of cerebrovascular disease. J Korean Neurosurg Soc. 2019. 62: 35-45
10. Kodama N, Sasaki T, Sakurai Y. Transthird ventricular approach for a high basilar bifurcation aneurysm. Report of three cases. J Neurosurg. 1995. 82: 664-8
11. Mizoi K, Yoshimoto T, Takahashi A, Ogawa A. Direct clipping of basilar trunk aneurysms using temporary balloon occlusion. J Neurosurg. 1994. 80: 230-6
12. Mori R, Yuki I, Kajiwara I, Nonaka Y, Ishibashi T, Karagiozov K. Hybrid operating room for combined neuroendovascular and endoscopic treatment of ruptured cerebral aneurysms with intraventricular hemorrhage. World Neurosurg. 2016. 89: 727-
13. Murayama Y, Arakawa H, Ishibashi T, Kawamura D, Ebara M, Irie K. Combined surgical and endovascular treatment of complex cerebrovascular diseases in the hybrid operating room. J Neurointerv Surg. 2013. 5: 489-93
14. Murayama Y, Irie K, Saguchi T, Ishibashi T, Ebara M, Nagashima H. Robotic digital subtraction angiography systems within the hybrid operating room. Neurosurgery. 2011. 68: 1427-32
15. Pitelli SD, Almeida GG, Nakagawa EJ, Marchese AJ, Cabral ND. Basilar aneurysm surgery: The subtemporal approach with section of the zygomatic arch. Neurosurgery. 1986. 18: 125-8
16. Ricci G, Ricci A, Gallucci M, Zotta D, Scogna A, Costagliola C. Combined endovascular and microsurgical approach in the treatment of giant paraclinoid and vertebrobasilar aneurysms. J Neurosurg Sci. 2005. 49: 1-6
17. Sano H, Kato Y, Hayakawa M, Akashi K, Kanno T. A transcrista galli, translamina terminalis approach for highly placed basilar bifurcation aneurysms. Acta Neurochir (Wien). 1997. 139: 1020-4
18. Shucart WA, Kwan ES, Heilman CB. Temporary balloon occlusion of a proximal vessel as an aid to clipping aneurysms of the basilar and paraclinoid internal carotid arteries: Technical note. Neurosurgery. 1990. 27: 116-9
19. Skrap M, Petralia B, Toniato G. Temporary balloon occlusion during the surgical treatment of giant paraclinoid and vertebrobasilar aneurysms. Acta Neurochir (Wien). 2010. 152: 435-42
20. Spiessberger A, Strange F, Fandino J, Marbacher S. Microsurgical clipping of basilar apex aneurysms: A systematic historical review of approaches and their results. World Neurosurg. 2018. 114: 305-16
21. Sugita K, Kobayashi S, Shintani A, Mutsuga N. Microneurosurgery for aneurysms of the basilar artery. J Neurosurg. 1979. 51: 615-20
22. Yasargil MG, Antic J, Laciga R, Jain KK, Hodosh RM, Smith RD. Microsurgical pterional approach to aneurysms of the basilar bifurcation. Surg Neurol. 1976. 6: 83-91


