

- Department of Neurosurgery, Faculty of medicine of Tunis, El Manar-Tunis University, Burns and Trauma Center, Ben Arous, Tunisia
Correspondence Address:
Ghassen Gader
Department of Neurosurgery, Faculty of medicine of Tunis, El Manar-Tunis University, Burns and Trauma Center, Ben Arous, Tunisia
DOI:10.4103/sni.sni_350_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Mohamed Badri, Ghassen Gader, Kamel Bahri, Ihsen Zammel. Cervicothoracic syringomyelia caused by cervical spinal stenosis: Case report and literature review. 06-Dec-2017;8:288
How to cite this URL: Mohamed Badri, Ghassen Gader, Kamel Bahri, Ihsen Zammel. Cervicothoracic syringomyelia caused by cervical spinal stenosis: Case report and literature review. 06-Dec-2017;8:288. Available from: http://surgicalneurologyint.com/surgicalint-articles/cervicothoracic-syringomyelia-caused-by-cervical-spinal-stenosis-case-report-and-literature-review/
Date of Submission
22-Sep-2017
Date of Acceptance
08-Oct-2017
Date of Web Publication
06-Dec-2017
Abstract
Background:Syringomyelia is commonly associated with Chiari malformations, spinal trauma, arachnoiditis, or tumors. However, rarely, cervical canal stenosis is implicated in intramedullary cavitations.
Case Discription:Here, we report the case of a 60-year-old male patient who presented with loss of pain and temperature sensation in upper extremities associated with a spastic tetraparesis. On magnetic resonance imaging, the patient was found to have syringomyelia extending from C1 to Th3. Following posterior decompressive surgery, the syrinx resolved along with the patient's neurological complaints.
Conclusion:Here, the authors presented a case and reviewed the literature regarding how cervical spinal stenosis may contribute to cervical or thoracic syringomyelia.
Keywords: Cervical canal stenosis, surgery, syringomyelia
INTRODUCTION
Syringomyelia is characterized by a cystic, fluid-filled cavity presenting inside the spinal cord.[
However, rarely has cervical spinal stenosis/spondylosis contributed to the formation of a cervicothoracic syrinx.[
CASE DESCRIPTION
A 60-year-old male presented with a 1-year history of a traumatic, increasing radicular pain and loss of pain and temperature in the upper extremities, accompanied by a severe and spastic tetraparesis. Neurological examination revealed mainly spastic tetraparesis and syringomyelic syndrome in the upper limbs. The cervical magnetic resonance imaging (MRI) on T2-weighted studies showed circumferential spondylotic (cervical spondylosis and osteophytes, and posteriorly by ligament flavum hypertrophy) compression at the C3/C4, C4/C5, and C5/C6 levels [
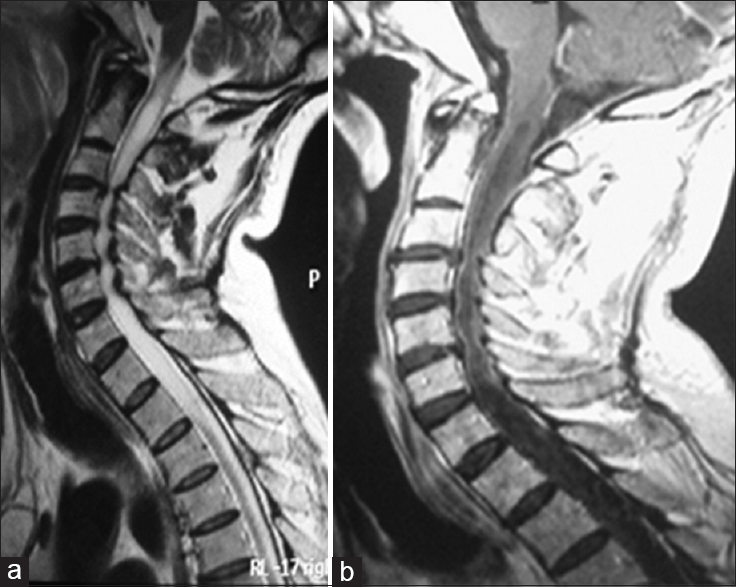
Following a C2–C6 cervical laminectomy, the patient fully recovered. The MRI obtained six months postoperatively showed complete regression of the prior syrinx [

DISCUSSION
Syringomyelia is associated with numerous different pathologies, including spinal trauma, Chiari malformation or other craniocervical anomalies, meningitis, but rarely, cervical spondylosis.
Etiologies of syrinx with cervical spondylosis
Theories leading to syrinx formation secondary to cervical spondylosis include ischemia,[
Treatment options for cervicothoracic syrinx
Although there are various treatment options for cervical-thoracic syrinx due to Chiari malformations (e.g., foramen magnum decompression and syringosubarachnoid shunt), there are no established procedure for dealing with syrinxes due to cervical spondylosis with immediate regression of the intramedullary cavitation and symptoms [
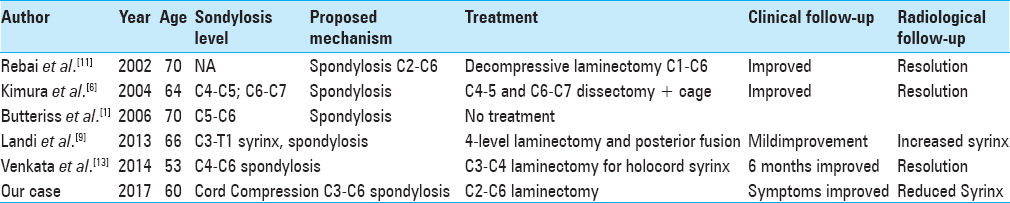
The regression of the syringomyelic cavity in our patient, and in other reports, is that the relief of epidural compression is the main element in the pathophysiology of the formation of syrinx.[
CONCLUSION
Cervicothoracic syringomyelia attributed to cervical spondylosisis is rare. Here, surgical decompression, consisting of a C2–C6 laminectomy, addressing circumferential spondylotic changes resulted in the regression of symptoms and complete radiological resolution of the syrinx.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that name and initial will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
References
1. Butteriss DJ, Birchall D. A Case of Syringomyelia Associated with Cervical Spondylosis. Br J Radiol. 2006. 79: 123-5
2. Chang HS, Nejo T, Yoshida S, Oya S, Matsui T. Increased Flow Signal in Compressed Segments of the Spinal Cord in Patients with Cervical Spondylotic Myelopathy. Spine. 2014. 39: 2136-42
3. Elliott NSJ, Bertram CD, Martin BA, Brodbelt AR. Syringomyelia: A Review of the Biomechanics. J Fluids Structures. 2013. 40: 1-24
4. Greitz D. Unraveling the Riddle of Syringomyelia. Neurosurg Rev. 2006. 29: 251-4
5. Kato N, Tanaka T, Nagashima H, Arai T, Hasegawa Y, Tani S. Syrinx Disappearance Following Laminoplasty in Cervical Canal Stenosis Associated with Chiari Malformation: Case Report. Neurol Med Chir. 2010. 50: 172-4
6. Kimura R, Park YS, Nakase H, Sakaki T. Syringomyelia Caused by Cervical Spondylosis. Acta Neurochir. 2004. 146: 175-8
7. Klekamp J. The Pathophysiology of Syringomyelia-historical Overview and Current Concept. Acta Neurochir. 2002. 144: 649-64
8. Klekamp J. Surgical treatment of multilevel cervical spondylosis in patients with or without a history of syringomyelia. Eur Spine J. 2017. 26: 948-57
9. Landi A, Nigro L, Marotta N, Mancarella C, Donnarumma P, Delfini R. Syringomyelia Associated with Cervical Spondylosis. World J Clin Cases. 2013. 1: 111-5
10. Levine DN. The Pathogenesis of Syringomyelia Associated with Lesions at the Foramen Magnum: A Critical Review of Existing Theories and Proposal of a New Hypothesis. J Neurol Sci. 2004. 220: 3-21
11. Rebai R, Boudawara MZ, Ben Yahia M, Mhiri C. Syringomyelobulbia Associated with Cervical Spondylosis. Pathophysiology and Therapeutic Implications. Neurochirurgie. 2002. 48: 120-3
12. Tortora F, Napoli M, Caranci F, Cirillo M, Pepe D, Cirillo S. Spontaneous Regression of Syringomyelia in a Young Patient with Chiari Type I Malformation. J Neuroradiol. 2012. 25: 593-7
13. Venkata SSB, Arimappamagan A, Lafazanos S, Pruthi N. Syringomyelia Secondary to Cervical Spondylosis: Case Report and Review of Literature. Journal of Neurosciences in Rural Practice. 2014. 5: S78-

