

- Department of Surgery, Section of Neurosurgery, Aga Khan University Hospital, Karachi, Pakistan
- Medical College, Aga Khan University, Karachi, Pakistan
- Department of Neurosurgery, Great Ormond Street Hospital, London, UK
Correspondence Address:
Muhammad Shahzad Shamim
Department of Neurosurgery, Great Ormond Street Hospital, London, UK
DOI:10.4103/2152-7806.180764
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Akhtar S, Azeem A, Shamim MS, Tahir MZ. Composite split cord malformation associated with a dermal sinus tract, dermoid cyst, and epidural abscess: A case report and review of literature. Surg Neurol Int 19-Apr-2016;7:43
How to cite this URL: Akhtar S, Azeem A, Shamim MS, Tahir MZ. Composite split cord malformation associated with a dermal sinus tract, dermoid cyst, and epidural abscess: A case report and review of literature. Surg Neurol Int 19-Apr-2016;7:43. Available from: http://surgicalneurologyint.com/surgicalint_articles/composite-split-cord-malformation-associated-with-a-dermal-sinus-tract-dermoid-cyst-and-epidural-abscess-a-case-report-and-review-of-literature/
Abstract
Background:Split cord malformation (SCM) is typically present at a single level but rarely, may be present at multiple levels in the spinal cord and can be associated with a wide array of lesions such as myelomeningoceles, lipomas, teratomas, and dermal sinus tracts (DSTs).
Case Description:We describe a case of a 15-month-old female child who presented with high-grade fever and progressive motor weakness in the lower limbs. Magnetic resonance imaging revealed the presence of SCM along with an epidural abscess, DST, and dermoid cyst. The child underwent surgery for excision of DST along with removal of the dermoid cyst and drainage of epidural abscess. The postoperative course was uneventful. Elective repair of the SCM was performed 4 weeks later. The postoperative course was uneventful again.
Conclusion:To the best of our knowledge, the combination of a composite SCM with a DST and dermoid cyst with associated epidural abscess has rarely been reported in literature.
Keywords: Dermal sinus tract, dermoid cyst, empyema, split cord malformation
INTRODUCTION
Split cord malformation (SCM) has been classified by Pang et al., into Types 1 and 2.[
Congenital dermal sinus tract (DST) formation is an anomaly resulting from the abnormal separation of the neuroectoderm from the cutaneous ectoderm.[
The combination of Type 1 SCM with associated anomalies has been reviewed in literature; however, to the best of our knowledge, a combination of SCM at various levels in continuation with DST and dermoid cyst has rarely been reported. This case report also reviews the relevant literature related to this presentation.
CASE REPORT
A 15-month-old female child presented with high-grade fever and progressive bilateral leg weakness with difficulty in balance for 2 weeks. There was no history of trauma, and the birth history was unremarkable. The patient was the first child of consanguineous parents.
On clinical examination, power in the left lower limb was 3/5 and 4/5 in the right lower limb. Examination of the back revealed a very small, abnormal tuft of hair in the midline in the mid lumbar region suggesting the presence of occult spinal dysraphism [
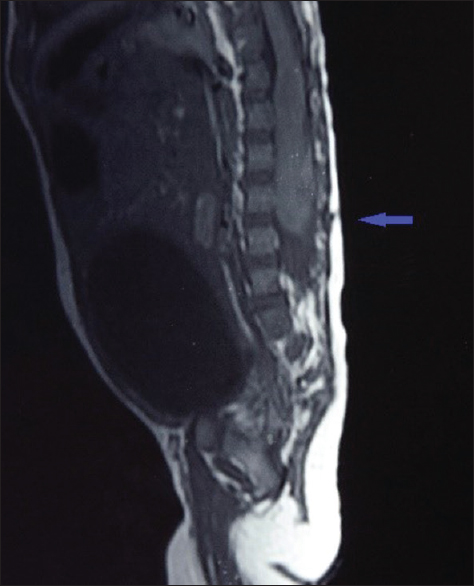
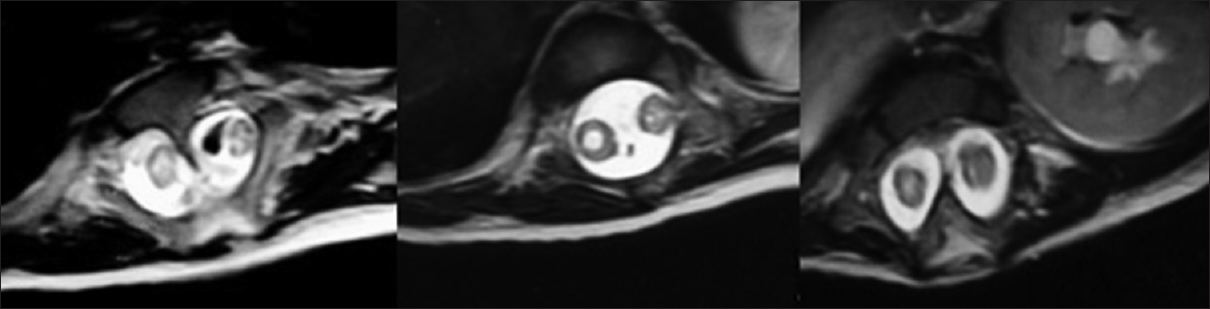
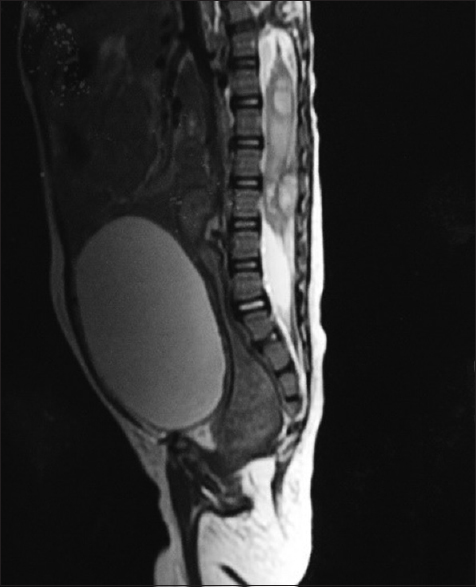
Magnetic resonance imaging (MRI) of the brain and full spine was carried out which revealed the presence of two Type 1 SCM in the thoracolumbar regions. The malformation started as a Type 1 SCM from T4 to T6, separated by a bony spur. The two hemicords then entered the same dural sheath but before uniting into a single, normal spinal cord, divided into another Type 1 SCM from T9 to T11, separated by another bony spur. The two hemicords then fused into a single dural sheath before continuing as a single spinal cord from T12 onward [
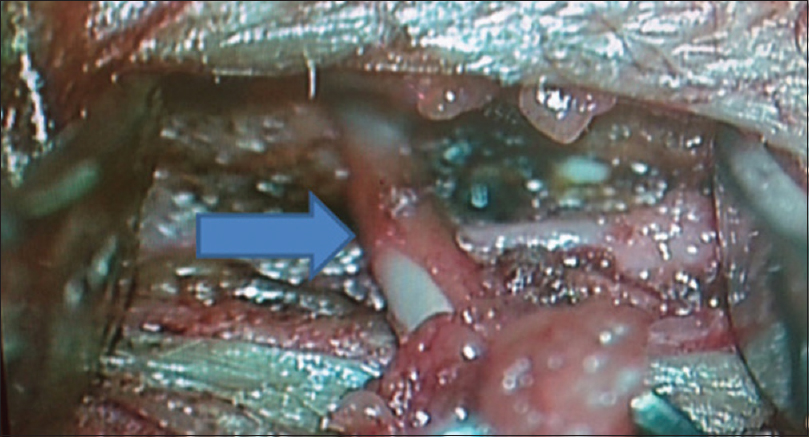
The child underwent surgery through a limited exposure, incorporating the tuft of hair. Upon dissecting the lumbar fascia, a thick-walled, pearly white, elongated sinus tract was soon visible [
Culture from the pus showed growth of Staphylococcus aureus which was also resistant to all beta-lactams. Histopathology revealed a sinus tract with collagenous tissue without any lining, along with separate keratin flakes and a small bony chip. The cystic lesion showed skin tissue lined by keratinizing squamous epithelium. The lumen had keratin flakes and a granular layer was seen. Focally, hair follicles were also present. However, no other germ cell component was seen. The features favored those of a dermoid cyst. The child made an uneventful postoperative recovery and was kept on broad-spectrum antibiotics which were then changed to specific Gram-positive coverage, extending to a full 2 weeks of administration. No new neurological deficits were noted, and she was subsequently discharged. At subsequent follow-ups, the child regained full function in both the lower limbs.
Upon completion of her antibiotic course and normalization of CRP, she was readmitted 4 weeks later for elective repair of her multilevel SCM. Both malformations were approached through a single linear midline incision, and after respective laminectomies, the bony spurs at each level were individually drilled and removed. The operative findings correlated with the MRI interpretation and in between the two Type 1 SCM, there existed a single dural sheath. The canal was spacious and no attempts were made to reconstruct the two dural sheaths into one, at either level. The child once again made an uneventful recovery.
DISCUSSION
The unified theory for SCM states that it develops due to the formation of an “accessory neurenteric canal,” which allows communication between the ectoderm and endoderm as stated by Pang et al.[
Our patient presented with two-level, Type 1 SCM along with a DST, a dermoid cyst, and an epidural abscess. Our review of literature focusing on the presence of SCM at more than one level and its presence with a DST (with or without a dermoid cyst) is summarized in
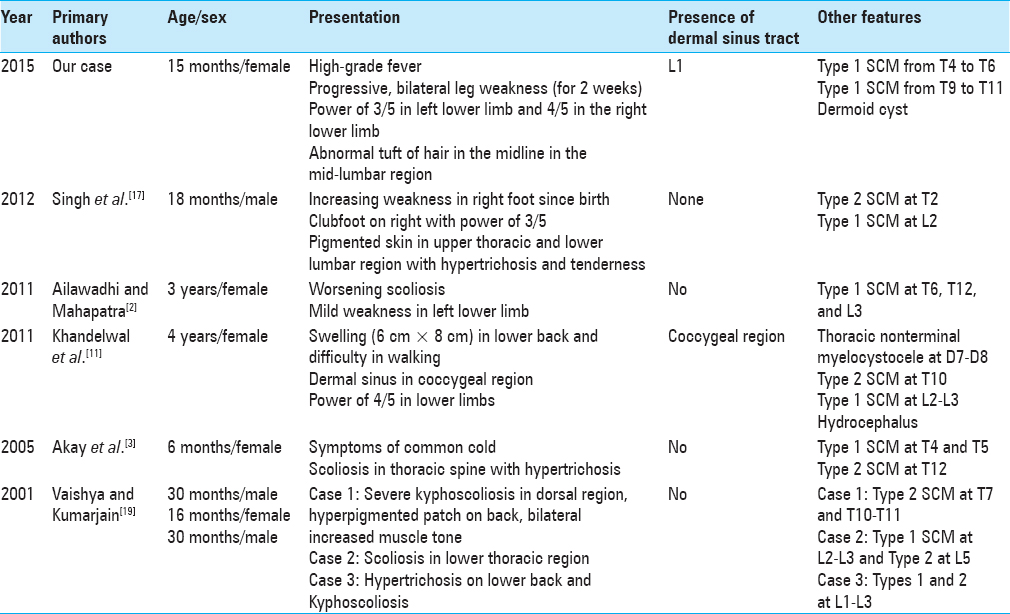
The case series by Ackerman and Menezes reported the prevalence of DSTs as 18.5% in the cervical region, 14.8% in the thoracic region, 33% in the lumbar region, and 33% in the lumbosacral region.[
On reviewing the literature, we were able to find only one case of a multilevel SCM with a DST as reported by Khandelwal et al. and six cases of composite SCM as reported by Ersahin et al. in his series of 131 cases.[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ackerman LL, Menezes AH. Spinal congenital dermal sinuses: A 30-year experience. Pediatrics. 2003. 112: 641-7
2. Ailawadhi P, Mahapatra AK. An unusual case of spinal dysraphism with four splits including three posterior spurs. Pediatr Neurosurg. 2011. 47: 372-5
3. Akay KM, Izci Y, Baysefer A, Timurkaynak E. Composite type of split cord malformation: Two different types at three different levels: Case report. J Neurosurg. 2005. 102: 436-8
4. Dąmbska M, Wisniewski KE.editors. Normal and Pathologic Development of the Human Brain and Spinal Cord 1. England: John Libbey and company Ltd; 1999. p.
5. De Vloo P, Lagae L, Sciot R, Demaerel P, van Loon J, Van Calenbergh F. Spinal dermal sinuses and dermal sinus-like stalks analysis of 14 cases with suggestions for embryologic mechanisms resulting in dermal sinus-like stalks. Eur J Paediatr Neurol. 2013. 17: 575-84
6. Ersahin Y, Mutluer S, Kocaman S, Demirtas E. Split spinal cord malformations in children. J Neurosurg. 1998. 88: 57-65
7. Ersahin Y. Split cord malformation types I and II: A personal series of 131 patients. Childs Nerv Syst. 2013. 29: 1515-26
8. French BN. The embryology of spinal dysraphism. Clin Neurosurg. 1983. 30: 295-340
9. Hung PC, Wang HS, Wu CT, Lui TN, Wong AM. Spinal intramedullary abscess with an epidermoid secondary to a dermal sinus. Pediatr Neurol. 2007. 37: 144-7
10. Jindal A, Mahapatra AK. Spinal congenital dermal sinus: An experience of 23 cases over 7 years. Neurol India. 2001. 49: 243-6
11. Khandelwal A, Tandon V, Mahapatra AK. An unusual case of 4 level spinal dysraphism: Multiple composite type 1 and type 2 split cord malformation, dorsal myelocystocele and hydrocephalous. J Pediatr Neurosci. 2011. 6: 58-61
12. Mahapatra AK, Gupta DK. Split cord malformations: A clinical study of 254 patients and a proposal for a new clinical-imaging classification. J Neurosurg. 2005. 103: 531-6
13. Mete M, Umur AS, Duransoy YK, Barutçuoglu M, Umur N, Gurgen SG. Congenital dermal sinus tract of the spine: Experience of 16 patients. J Child Neurol. 2014. 29: 1277-82
14. Pang D, Dias MS, Ahab-Barmada M. Split cord malformation: Part I: A unified theory of embryogenesis for double spinal cord malformations. Neurosurgery. 1992. 31: 451-80
15. Pang D. Split cord malformation: Part II: Clinical syndrome. Neurosurgery. 1992. 31: 481-500
16. Radmanesh F, Nejat F, El Khashab M. Dermal sinus tract of the spine. Childs Nerv Syst. 2010. 26: 349-57
17. Singh DK, Singh N, Singh R. Widely separated composite split cord malformation. BMJ Case Rep 2012. 2012. p.
18. Thompson DN. Spinal inclusion cysts. Childs Nerv Syst. 2013. 29: 1647-55
19. Vaishya S, Kumarjain P. Split cord malformation: Three unusual cases of composite split cord malformation. Childs Nerv Syst. 2001. 17: 528-30

