

- Department of Neurosurgery, School of Medicine, Keio University, Tokyo, Japan
Correspondence Address:
Masahiro Toda
Department of Neurosurgery, School of Medicine, Keio University, Tokyo, Japan
DOI:10.4103/2152-7806.199556
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Yu Nakagawa, Masahiro Toda, Shunsuke Shibao, Kazunari Yoshida. Delayed and isolated oculomotor nerve palsy following minor head trauma. 06-Feb-2017;8:20
How to cite this URL: Yu Nakagawa, Masahiro Toda, Shunsuke Shibao, Kazunari Yoshida. Delayed and isolated oculomotor nerve palsy following minor head trauma. 06-Feb-2017;8:20. Available from: http://surgicalneurologyint.com/surgicalint_articles/delayed-and-isolated-oculomotor-nerve-palsy-following-minor-head-trauma/
Date of Submission
02-Aug-2016
Date of Acceptance
05-Dec-2016
Date of Web Publication
06-Feb-2017
Abstract
Background:The purpose of this study was to consider the mechanism of isolated oculomotor nerve palsy after minor head trauma.
Case Description:We report a rare case of delayed and isolated oculomotor nerve palsy following minor head trauma. A 19-year-old boy complained of double vision 1 day after a minor head trauma. Neuro-ophthalmic examination showed isolated left oculomotor nerve palsy. Computed tomography and magnetic resonance imaging examination revealed no abnormal findings and steroid therapy was administered for a week. Three months after the injury, the ptosis and extraocular movements had fully resolved, although the pupillary light reflex was still abnormal.
Conclusions:Delayed and isolated oculomotor nerve palsy may be caused by an injury at the point where the oculomotor nerve runs over the posterior petroclinoid ligament. Because edema of the damaged oculomotor nerve might result in constriction at the point where the nerve pierces the dura of the cavernous sinus, symptoms of oculomotor nerve palsy appeared late after trauma. Steroid treatment reducing edema could be effective for delayed and isolated oculomotor nerve palsy following minor head trauma.
Keywords: Minor head trauma, oculomotor nerve injury, steroid
INTRODUCTION
The severity of head trauma is significantly higher in patients with traumatic brain injury (TBI) and cranial nerve injury than in those with intact cranial nerve function, with a greater number of radiological abnormalities on computed tomography (CT) scans and poor neurological outcome.[
Therefore, an isolated oculomotor nerve palsy that occurs after minor head trauma should raise concerns about an underlying lesion that could be compressing, stretching, or infiltrating the oculomotor nerve, predisposing it to dysfunction following an otherwise inconsequential injury. Previous studies have reported that oculomotor nerve palsy after minor head trauma is the presenting sign of cerebral aneurysmal compression or uncal herniation due to intracranial tumor in some patients.[
CASE REPORT
A 19-year-old boy with an unremarkable medical history suffered a bruise to his occiput during a game of rugby. He did not lose consciousness and continued playing. Next day, he visited the Department of Neurosurgery complaining of headache. The neurological exam and CT was normal [
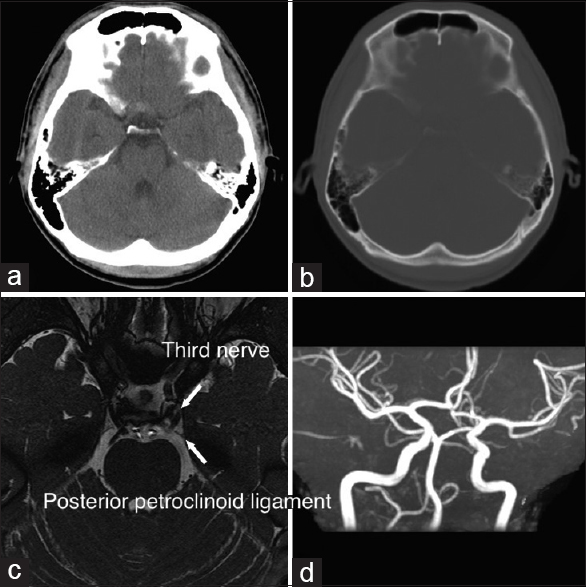
Figure 1
Computed tomography and magnetic resonance imaging. CT and MRI examinations demonstrate no abnormal findings. No intracranial hemorrhage (a) and no basilar fracture (b) are apparent in axial CT images on day 1. An axial heavy T2-weighted MRI image (c) shows the left oculomotor nerve running over the posterior petroclinoid ligament and no apparent damage to the nerve on day 7. No aneurysm is visible in MR angiography (d)
DISCUSSION
Oculomotor nerve palsy may be caused by damage to the nerve at any point along its path between the oculomotor nucleus in the midbrain and the extraocular muscles within the orbit. There are reports of injury to the oculomotor nerve at its exit from the brainstem, from the superior orbital fissure,[
It has been suggested that traumatic oculomotor nerve injury with minor head trauma occurs because of differential movements between the brainstem and supratentorial structures, which can stretch the nerve and cause distal fascicular damage.[
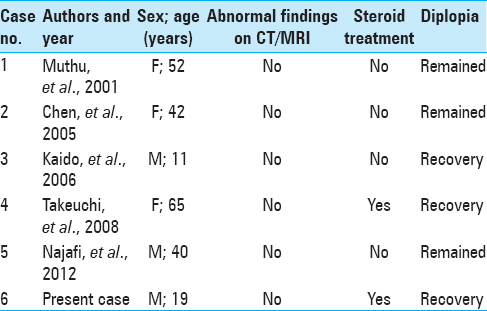
Isolated third nerve palsy without any other symptoms such as loss of consciousness or radiological abnormalities is exceptionally rare, this being the 6th case reported in the literature [
Prism therapy and strabismus surgery may be helpful in patients with oculomotor nerve palsy. However, indications for these treatments and their effectiveness are limited. Until now, there is no satisfactory surgical treatment for patients with complete oculomotor nerve palsy.
CONCLUSION
We report that minor head trauma can cause isolated oculomotor nerve palsy in the absence of loss of consciousness and abnormalities on brain CT, MRI, and MRA. The mechanism underlying oculomotor nerve injury following minor head trauma is still unclear, although injury at the posterior petroclinoid ligament is suggested. Steroid therapy may possibly be effective for functional recovery.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Balcer LJ, Galetta SL, Bagley LJ, Pakola SJ. Localization of traumatic oculomotor nerve palsy to the midbrain exit site by magnetic resonance imaging. Am J Ophthalmol. 1996. 122: 437-9
2. Chen CC, Pai YM, Wang RF, Wang TL, Chong CF. Isolated oculomotor nerve palsy from minor head trauma. Br J Sports Med. 2005. 39: e34-
3. Coello AF, Canals AG, Gonzalez JM, Martín JJA. Cranial nerve injury after minor head trauma. J Neurosurg. 2010. 113: 547-55
4. Dhaliwal A, West AL, Trobe JD, Musch DC. Third, fourth, and sixth cranial nerve palsies following closed head injury. J Neuroophthalmol. 2006. 26: 4-10
5. Eyster EF, Hoyt WF, Wilson CB. Oculomotor palsy from minor head trauma. An initial sign of basal intracranial tumor. JAMA. 1972. 220: 1083-6
6. Grant G, Rostomily RR, Kim DK, Mayberg MR, Farrell D, Avellino A. Delayed facial palsy after resection of vestibular schwannoma. J Neurosurg. 2002. 97: 93-6
7. Guthikonda B, Pensak ML, Theodosopoulos PV. Delayed facial palsy after the anterior petrosal approach: Case report and review of the literature. Neurosurgery. 2010. 66: E845-6
8. Heinze J. Cranial nerve avulsion and other neural injuries in road accidents. Med J Aust. 1969. 2: 1246-9
9. Jacobson DM, Warner JJ, Choucair AK, Ptacek LJ. Trochlear nerve palsy following minor head trauma. A sign of structural disorder. J Clin Neuroophthalmol. 1988. 8: 263-8
10. Kaido T, Tanaka Y, Kanemoto Y, Katsuragi Y, Okura H. Traumatic oculomotor nerve palsy. J Clin Neurosci. 2006. 13: 849-52
11. Keefe WP, Rucker CW, Kernohan JW. Pathogenesis of paralysis of the third cranial nerve. Arch Ophthalmol. 1960. 63: 585-92
12. Kuo LT, Huang APH, Yang CC, Tsai SY, Tu YK, Huang SJ. Clinical outcome of mild head injury with isolated oculomotor nerve palsy. J Neurotrauma. 2010. 27: 1959-64
13. Levy RL, Geist CE, Miller NR. Isolated oculomotor palsy following minor head trauma. Neurology. 2005. 65: 169-
14. Morton RP, Ackerman PD, Pisansky MT, Krezalek M, Leonetti JP, Raffin MJM. Prognostic factors for the incidence and recovery of delayed facial nerve palsy after vestibular schwannoma resection. J Neurosurg. 2011. 114: 375-80
15. Muthu P, Pritty P. Mild head injury with isolated third nerve palsy. Emerg Med J. 2001. 18: 310-1
16. Nagaseki Y, Shimizu T, Kakizawa T, Fukamachi A, Nukui H. Primary internal ophthalmoplegia due to head injury. Acta Neurochir. 1989. 97: 117-22
17. Najafi MR, Mehrbod N. Isolated third nerve palsy from mild closed head trauma. Arch Iran Med. 2012. 15: 583-4
18. Neetens A, Van Aerde F. Extra-ocular muscle palsy from minor head trauma. Initial sign of intracranial tumour. Bull Soc Belge Ophtalmol. 1981. 193: 161-7
19. Takeuchi S, Takasato Y, Masaoka H, Hayakawa T, Otani N, Yoshino Y. Isolated traumatic oculomotor nerve palsy caused by minor head trauma. Brain Nerve. 2008. 60: 555-8
20. Tiffin P, MacEwen CJ, Craig E, Clayton G. Acquired palsy of the oculomotor, trochlear and abducens nerves. Eye. 1996. 10: 377-84
21. Walter KA, Newman NJ, Lessell S. Oculomotor palsy from minor head trauma: Initial sign of intracranial aneurysm. Neurology. 1994. 44: 148-50

