

- Department of Neurosurgery and Neurology, IRCCS Galeazzi Hospital, Milan, Italy
Correspondence Address:
Edvin Zekaj
Department of Neurosurgery and Neurology, IRCCS Galeazzi Hospital, Milan, Italy
DOI:10.4103/sni.sni_144_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Domenico Servello, Christian Saleh, Alberto R. Bona, Marina Minichiello, Edvin Zekaj. Dual floor burr hole technique in deep brain stimulation: A retrospective study on 209 patients. 20-Nov-2017;8:280
How to cite this URL: Domenico Servello, Christian Saleh, Alberto R. Bona, Marina Minichiello, Edvin Zekaj. Dual floor burr hole technique in deep brain stimulation: A retrospective study on 209 patients. 20-Nov-2017;8:280. Available from: http://surgicalneurologyint.com/surgicalint-articles/dual-floor-burr-hole-technique-in-deep-brain-stimulation-a-retrospective-study-on-209-patients/
Date of Submission
04-May-2017
Date of Acceptance
31-Aug-2017
Date of Web Publication
20-Nov-2017
Abstract
Background:Skin erosion/infections due to deep brain stimulation hardware are highly worrisome complications. They can lead to the removal of the entire deep brain stimulation device, and consequently hold the whole treatment in otherwise pharmacologically refractory patients. Several techniques have been used such as C-shape skin incision and dual floor burr hole or single passage of connecting cables to reduce the incidence of skin complications.
Methods:In this paper, we describe our experience in 209 patients using a dual-floor burr hole technique to reduce skin adverse effects.
Conclusion:The dual floor burr hole technique is a safe technique with a low incidence of skin erosions and complications.
Keywords: Complications, deep brain stimulation, dual floor burr hole, surgical technique
INTRODUCTION
Over the last three decades since the renaissance of deep brain stimulation (DBS) for pharmacological refractory motor diseases, its indications have rapidly expanded to other conditions such as psychiatric disorders and Alzheimer's disease. To date there have been approximately 100,000 patients treated with DBS. Surgical objectives are to improve clinical symptoms and reduce surgical side effects and complications. Regarding other surgeries where permanent hardware implants are used hardware-related (HWR) complications constitute in DBS surgery a worrisome chapter. In DBS HWR, complications can be broadly divided into hardware malfunctioning and complications caused by the permanent hardware presence such as skin erosions/infections or even poor aesthetical results.
In DBS hardware, complications have been reported up to 26%.[
MATERIALS AND METHODS
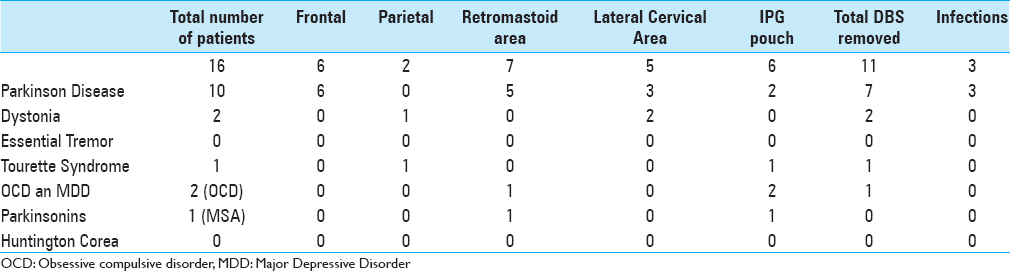
We conducted a retrospective study on skin erosions in all patients undergoing DBS at our department from January 2010 to December 2015. We divided and allocated patients based on the sites of the skin erosions in five groups – frontal, parietal, retro-mastoid, lateral-cervical, and internal pulse generator (IPG) pouch level. The frontal group included erosions at the level of the burr hole cap area, the parietal group included erosions at the connecting cables level, the retromastoid group included erosions at the connectors level, the lateral-cervical group included erosions at the level of the connecting cables in the lateral cervical area, and IPG pouch for erosions at the IPG level. Clinical data were collected by the surgical registry of the senior neurosurgeon (D.S.) and by all computerized patient medical records. Patients with skin erosions were carefully evaluated to find any risk factor that might be correlated with skin erosion. All the DBS surgical procedures were performed by the senior neurosurgeon (D.S.). A total of 209 DBS procedures were performed with bilateral lead positioning in all cases (418 dual burr hole procedures). There were 131 males and 78 females, aged between 21 to 77 years (mean 57 years). One hundred and seventy-one patients were treated for PD, 8 patients had dystonia, 3 patients had essential tremor, 15 patients were treated for TS, 5 patients had obsessive compulsive disorder (OCD), 1 patients had major depressive disorder, 5 patients had parkinsonism (3 patients with progressive supranuclear palsy, 1 with post-anoxic parkinsonism, and 1 with multiple system atrophy), and one patient had Huntington Chorea [

Surgical procedure
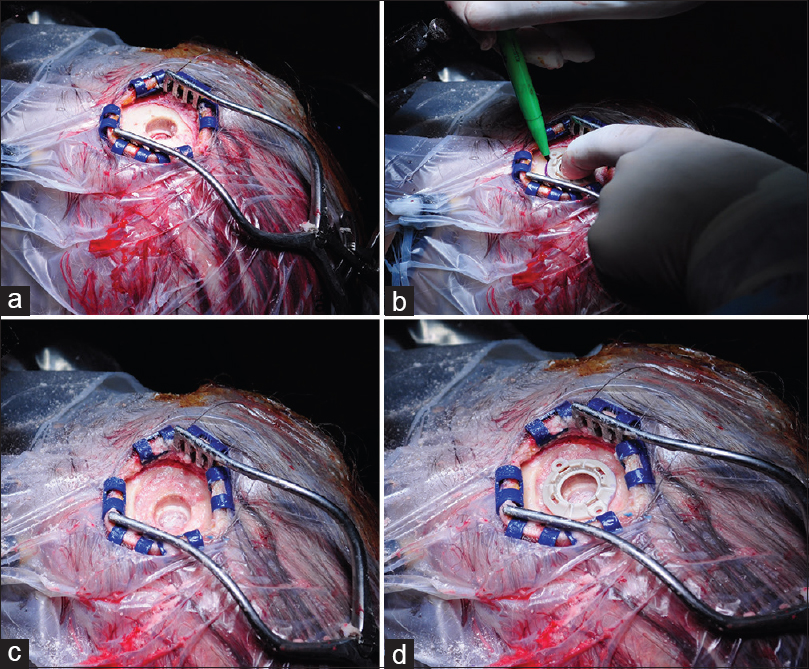
The patient was positioned in a supine position with the head fixed to the operating table by the head frame. We performed an accurate hair washing or scalp brushing with povidone iodine solution and betadine (hair cutting was not performed). The O-Arm was positioned to acquire the intraoperative radiological examinations. A sterile drape was fixed to the patient's head and to the O-Arm. Under local anesthesia, a 5–6 cm linear skin incision was performed centered at the trajectory of the electrodes. With a high speed drill a 14-mm burr hole was performed [

RESULTS
Sixteen patients (7.6%) had skin erosions. Five patients exhibited multiple skin erosions in sequential time. The frontal region at the burr hole cap level skin erosions occurred in 6 patients, retromastoid area in 7 patients, subclavicular region at the IPG level in 6 cases, lateral cervical region in 5 patients, and parietal area in 2 patients. In all patients, we performed a surgical revision surgery, but in 11 patients we had to remove the entire DBS system [

DISCUSSION
Hardware-related complication can be divided in hardware malfunctioning and tissue complications related to the permanent presence of the hardware. The most frequent tissue complications are skin erosions and infections, and are one of the main concerns for functional neurosurgeon as they can result in surgical revision or even removal of the entire system. The etiology is multifactorial, and in our opinion the most important factors may be summarized as three principal causes: factors related to characteristics of the device, to patients features, and to the surgical procedure.
Device features: Thicker and sharper devices increase the risk of skin erosions. The three main companies in DBS market (Medtronic, Boston Scientific, and Saint Jude Medical) have invested in improving devices. The latest burr hole cap and IPG are thinner than the older ones. Other companies such as Neuropace for epilepsy have developed a cranial IPG to reduce complication rates related to the internalization of the DBS electrode Patients features: It is well known that diabetic patients have more difficulties in wound healing, hence a higher incidence of skin problems in these patients is expected. Notoriously, PD patients may have important skin atrophy, which also increases risk of skin erosions. Another category of patients with higher risk in skin lesions are OCD patients or TS patients with OCD/OCB components. In these cases, the higher incidence of skin erosions and infection maybe due to the tendency of these patients to scratch the wounds. Warning and education of the patients on the risk of skin erosion due to repetitive touching and scratching of the wounds maybe sufficient for most patients. In rare cases, unorthodox solutions might be needed. For example, in one of the first patients with TS who underwent DBS at our department and presented with skin erosions due to repetitive scratching of the surgical wounds, we were forced to plaster the upper limbs of the patient for 2 months. With this medieval-like solution, the patient did well on wound healing and on response to DBS treatment Surgical procedure: Sites of skin complications are at the cranial cap, in the-retro mastoid area, the location of the connectors, and at the IPG pouch. There are few reports on how to lower the risk of skin erosions and infections. A recent and interesting study by Falowski et al.[
In our experience with the double floor burr hole we had 6 cases (0.9%) of skin erosions at the cranial cap level; all patients had PD. In all patients, we tried a surgical revision, which consisted of wound borders removal and deeper positioning of the distal end of the DBS electrodes; in 1 patient, a cutaneous flap was tried. In all patients, the DBS system was removed due to several skin erosions.
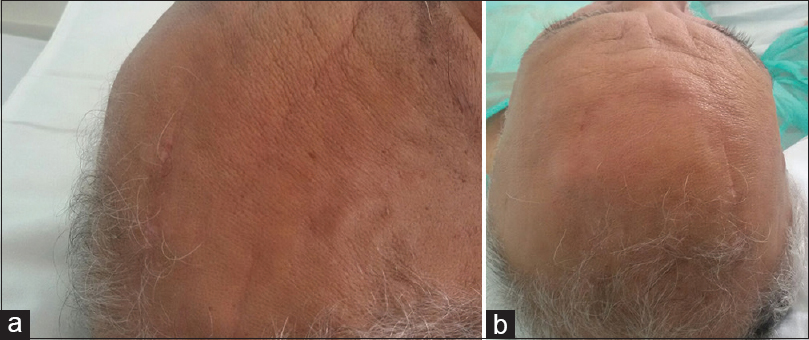
A poor aesthetic outcome was the result of skin groove formation in 8 patients, where the double burr hole was too deep. In none of these patients skin erosions were noted.
Tips and tricks
The dual floor burr hole does not require particular surgical skills but some precautions need to be kept in mind. In some patients, the cranial vault bone was so friable that during drilling with the cutting drill an excessive bone drilling was done which led to a deeper dual floor burr hole. In these cases, the burr hole cap was located deeper than the cranial vault favoring the formation of skin groove around the burr hole cap similar to the case reported in
CONCLUSION
The aim of our paper was to describe our technique on positioning the new burr hole cap generation for DBS surgery. These techniques aim on one side to improve the aesthetic result and on the other hand aim to reduce skin erosions at the stim lock level. From January 2010 to December 2015, 209 patients were treated with bilateral DBS. We had 6 cases of skin erosions at the cranial burr hole cap, which is 1.8% of the treated patients and only 0.9% considering the overall bilateral procedures. Another complication is the formation of peripheral skin groove which did not lead to skin erosions. The dual floor burr hole technique is a safe technique with a low incidence of skin erosions and complications.
Financial support and sponsorship
No funding was received for this research.
Conflicts of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
References
1. Falowski SM, Ooi YC, Bakay RA. Long-Term Evaluation of Changes in Operative Technique and Hardware-Related Complications With Deep Brain Stimulation. Neuromodulation. 2015. 18: 670-7
2. Hu X, Jiang X, Zhou X, Liang J, Wang L, Cao Y. Avoidance and management of surgical and hardware-related complications of deep brain stimulation. Stereotact Funct Neurosurg. 2010. 88: 296-303
3. Linhares P, Carvalho B, Vaz R. One-step tunneling of DBS extensions-a technical note. Acta Neurochir (Wien). 2013. 155: 837-40
4. Park YS, Kang JH, Kim HY, Kang DW, Chang WS, Kim JP. A combination procedure with double C-shaped skin incision and dual-floor burr hole method to prevent skin erosion on the scalp and reduce postoperative skin complications in deep brain stimulation. Stereotact Funct Neurosurg. 2010. 89: 178-84
5. Servello D, Sassi M, Gaeta M, Ricci C, Porta M. Tourette syndrome (TS) bears a higher rate of inflammatory complications at the implanted hardware in deep brain stimulation (DBS). Acta Neurochir (Wien). 2011. 153: 629-32
6. Servello D, Zekaj E, Saleh C, Lange N, Porta M. Deep Brain Stimulation in Gilles de la Tourette Syndrome: What Does the Future Hold. A Cohort of 48 Patients?. Neurosurgery. 2016. 78: 91-100
7. Sillay KA, Larson PS, Starr PA. Deep brain stimulator hardware-related infections: Incidence and management in a large series. Neurosurgery. 2008. 62: 360-
8. Sixel-Doring F, Trenkwalder C, Kappus C, Hellwig D. Skin complications in deep brain stimulation for Parkinson's disease: Frequency, time course, and risk factors. Acta Neurochir (Wien). 2010. 152: 195-200
9. Voges J, Waerzeggers Y, Maarouf M, Lehrke R, Koulousakis A, Lenartz D. Deep-brain stimulation: Long-term analysis of complications caused by hardware and surgery--experiences from a single centre. J Neurol Neurosurg Psychiatry. 2006. 77: 868-72
Commentary
DEEP BRAIN ELECTRODE DEVICE COMPLICATIONS
Antonio De Salles- Editor, SNI: Stereotactic São Paulo, Brazil E-mail:
a.desalles@yahoo.com
The authors touch on several important points to avoid complications of DBS devices installation. Incisions well planned, avoiding devices that are under the line of suture is a very important technical feature, mostly avoiding straight incision over the cap. It is indeed very unfortunate that the incidence of erosion is so high, not only for these authors, but also for all functional neurosurgeons implanting old fashion devices. Better burr-hole cap is overdue in the market. Actually the head implanted generators may indeed decrease the incidence of these unfortunate complications at least in the chest. Better devices are already in the market with low-profile hardware. Many surgeons practicing the installation of DBS no longer use the cap provided by the manufacturer, as it is prone to erosions, poor aesthetics, and high incidence of infections, as shown by the authors. Fortunately, the authors candidly present their complications and described them in detail; this paper may entice manufacturers to offer us better devices. We definitely hope so now that we have more competition in the market. The lowering profile of caps, use of smaller burr-holes (4–6 mm), and holding electrodes with plates and screws avoid all the cap complications that the authors mentioned, without the need of the double-burr hole they suggest. As one of the developers of the cap, we have already abandoned its use.[
References
1. Lee WYM, De Salles AAF, Frighetto L, Torres R, Behnke E, Bronstein J. Imaging techniques and electrode fixation methods for deep brain stimulation – Intraoperative MRI 0.2T, 1.5 T and fluoroscopy. Minimally Invas Neurosurgery. 2005. 48: 1-6

