

- Department of Neurosurgery, Stanford University School of Medicine, Los Angeles, California, USA
- Department of Neurosurgery, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA
- Department of Neurological Surgery, Stritch School of Medicine, Loyola University Chicago, Chicago, Illinois, USA
- Department of Neurosurgery, Baylor College of Medicine, Texas Children's Hospital, Houston, Texas, USA
- Department of Neurosurgery, University of California Los Angeles David Geffen School of Medicine, Los Angeles, California, USA
Correspondence Address:
Isaac Yang
Department of Neurosurgery, University of California Los Angeles David Geffen School of Medicine, Los Angeles, California, USA
DOI:10.4103/2152-7806.171220
Copyright: © 2015 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Li G, Dahdaleh NS, Germanwala AV, Lam S, Choy W, Smith ZA, Yang I. Key perspectives on donepezil following brain irradiation, sacroiliac joint fusion, indocyanine green fluorescence endoscope in endonasal transsphenoidal surgery, postconcussion syndrome in young athletes. Surg Neurol Int 08-Dec-2015;6:
How to cite this URL: Li G, Dahdaleh NS, Germanwala AV, Lam S, Choy W, Smith ZA, Yang I. Key perspectives on donepezil following brain irradiation, sacroiliac joint fusion, indocyanine green fluorescence endoscope in endonasal transsphenoidal surgery, postconcussion syndrome in young athletes. Surg Neurol Int 08-Dec-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/key-perspectives-on-donepezil-following-brain-irradiation-sacroiliac-joint-fusion-indocyanine-green-fluorescence-endoscope-in-endonasal-transsphenoidal-surgery-postconcussion-syndrome-in-young-athl/
Abstract
Keywords: Donepezil, metastasis, radiosurgery, sacroiliac joint
DONEPEZIL FOR IRRADIATED BRAIN TUMOR SURVIVORS: A PHASE III RANDOMIZED PLACEBO-CONTROLLED CLINICAL TRIAL[3]
Study Question: Does the addition of donepezil (a neurotransmitter modulator that is used in neurocognitive disorders) after partial or whole brain irradiation decrease cognitive impairment?
A two-center randomized, double blinded, placebo-controlled clinical trial was performed. One hundred and ninety-eight adult brain tumor patients who had partial or whole brain irradiation ≥6 months prior were randomized to receive single dose 5 mg daily donepezil for 6 weeks or 10 mg daily for 18 weeks or placebo. A cognitive test battery assessing memory, attention, language visuomotor, verbal fluency, and executive functions were administered prior to randomization and at 12 and 24 weeks. A cognitive composite score was the primary outcome and individual cognitive domains were measured.
Of the 198 patients, 66% had primary brain tumors, 27% had brain metastases, and 8% had prophylactic cranial irradiation. After 24 weeks of treatment, there was no difference in composite cognitive score between groups (P = 0.48). However, there was significant differences favoring donepezil in memory tasks (recognition, P = 0.027; discrimination, P = 0.007) and motor speed and dexterity (P = 0.016). There was a significant increase in the benefit of donepezil in patients with greater cognitive impairment prior to the treatment.
Perspective: More patients each year are being treated with partial or whole brain irradiation as the number of brain metastases that we treat are increasing. Cognitive impairment from brain irradiation is a major concern and significantly alters the quality of life of these patients. Early data suggested that donepezil could decrease the cognitive side effects of brain irradiation. This randomized, double blinded, placebo-controlled trial demonstrates that the addition of donepezil 6 months or greater after irradiation does not improve overall cognitive composite scores, but does improve certain tasks including memory and motor speed and dexterity. Currently, there is a large randomized multicenter trial being planned to see if hippocampal sparing irradiation can prevent cognitive decline in these patients. Other data suggests that the addition of memantine during irradiation could also decrease the cognitive side effects. This data suggests that donepezil could be another medication in the armamentarium of physicians. It would be interesting to see if daily donepezil during irradiation could have improved results compared to this trial.
Summary Written by: Gordon Li, MD
SURGICAL AND CLINICAL EFFICACY OF SACROILIAC JOINT FUSION: A SYSTEMATIC REVIEW OF THE LITERATURE[4]
Study Question: What are the surgical and clinical efficacy of sacroiliac joint (SIJ) fusion?
The authors systematically reviewed studies on SIJ fusion in the neurosurgical and orthopedic literature published from 2000 to 2014 to evaluate the evidence to support its use. Sixteen articles met their inclusion criteria including 5 case series, 8 retrospective studies, and 3 prospective cohort studies. The total number of patients included was 430, of whom 131 underwent open surgery, and 299 underwent minimally invasive surgery (MIS). The mean duration of follow-up was 60 months for open surgery and 21 months for MIS. The indications for surgery were SIJ degeneration followed by SIJ dysfunction (defined by SIJ pain but no radiographic evidence of degeneration). Fusion rates ranged from 20% to 90% for open surgery and 13–100% for MIS. The mean rate of excellent satisfaction, determined by pain reduction, function, and quality of life, was 54% (18–100%) in open surgical cases and 84% (56–100%) for MIS patients judged by patients’ stated satisfaction with the surgery. The mean reoperation rate after open surgery was 15% (0–65%) and 6% (0–17%) for MIS surgery. The most common serious complication following open SIJ fusion was painful hardware leading to removal (9.9%), and following MIS SIJ fusion was new onset facet joint pain (2.7%).
Perspective: The SIJ is a complex joint that connects the spine to the pelvis. It is stabilized by complex ligamentous and muscular attachments, and it only allows 4° of rotation and <2 mm of translation. Although the SIJ has been considered as a pain generator in patients with low back pain, surgical treatment by fusing the SIJ has not been gaining momentum until recently. The variety of multiple clinical presentations attributed to the SIJ as back pain, hip pain, buttock pain, and others makes it a diagnostic challenge as these symptoms overlap with other conditions that cause similar symptoms as spinal stenosis, lumbar spondylosis, and spondylolisthesis. These conditions are also often found in patients with suspect SIJ pain. Improvement of pain induced by certain provocative tests following an SIJ injection can help with the diagnosis; however, these methods have yet to be validated.
Although a subset of patients may benefit from SIJ fusions, the data presented in this systematic review is heterogeneous indicating the need of well-controlled prospective studies and randomized trials to provide more insight on efficacy and complication profile. At this stage, a multidisciplinary approach in treating patients with suspected SIJ pain must involve a pain specialist, a physiatrist, a physical therapist, and a spine surgeon. This approach would pave the way to a better understanding of this entity and hence the arrival to an appropriate treatment.
Summary Written by: Nader S. Dahdaleh, MD and Angela Bohnen, MD
USEFULNESS OF THE INDOCYANINE GREEN FLUORESCENSTUDY QUESTION: WHAT IS THE CLINICAL USEFULNESS OF THE INDOCYANINE GREEN (ICG) ENDOSCOPE FOR ENDOSCOPIC ENDONASAL SKULL BASE SURGERY[1]
Study Question: What is the clinical usefulness of the indocyanine green (ICG) endoscope for endoscopic endonasal skull base surgery?
The authors review the use of the ICG endoscope during endoscopic endonasal skull base surgery to assess its effectiveness in identifying the internal carotid artery (ICA), cavernous sinus (CS), and intercavernous sinus (ICS); evaluating real-time fluorescence changes within these structures and the skull base mass lesion, and discerning the patency of optic apparatus and infundibular perforators before and after tumor resection. A Karl Storz ICG endoscope with a light source capable of alternating between white and infrared light was used. A peripheral intravenous bolus of 12.5 mg of ICG was given before and after lesion resection. Data of the endoscopic images were recorded digitally on the video monitor. These images were further analyzed at 1-s intervals by investigating changes in the fluorescent intensity signals within the noted structures. Fluorescent intensity data were measured in a similar fashion to a red, green, and blue color model. For each anatomic structure, blue color values per pixel were calculated using the photoshop color sampler tool. These values range from 0 (black) to 255 (white).
A total of 38 patients underwent ICG endoscopic endonasal surgery over a period of 9 months at a single institution. The majority of the skull base pathology was pituitary adenomas. Approximately, 10–15 s after ICG administration, the cavernous segments of the ICAs were visible through the mucosa, bone, and dura. This time of reference was designated as second 1. Roughly 3–5 s later, the CS and ICS could be identified. The normal pituitary gland was able to be visualized 30 s later and was the dominant fluorescent signal intensity at 60 s. Following ICA visualization, meningioma arterial feeders and its dural attachment point were noted at 3 and 15 s, respectively. In addition to small perforators, fluorescent perfusion of the optic apparatus and infundibulum could also be visualized following lesion resection. Median time at peak color value and median peak color value in the studied locations are listed in the following
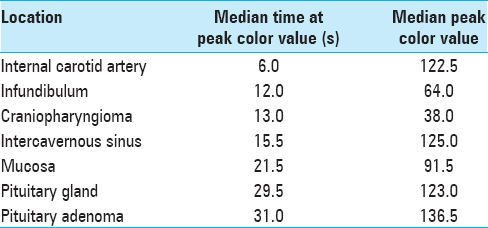
The differences in time at peak color value were not statistically significant between the pituitary gland and adenoma. Statistical significance of peak color values could not be determined due to a small sample size.
Perspective: The authors note that the ICG endoscope may be clinically useful to distinguish between the pituitary gland and craniopharyngiomas based on differences in peak color value, identify the dural attachment for skull base meningiomas based on fluorescence patterns, and provide real-time feedback regarding the patency of small perforators and perfusion of the optic apparatus and infundibulum. However, recognized limitations of this relatively new technology include the larger endoscope diameter (5.8 mm vs. 4.0 mm), lack of angled ICG endoscopes, and a small sample size of patients that prevents extracting statistically significant conclusions.
This article highlights the natural progression of the field of neurosurgery. Minimally invasive procedures with less brain retraction are becoming increasingly popular, and more challenging lesions are being treated while newer technologies are explored. Analogous to the benefit appreciated with intraoperative ICG use during microsurgery for aneurysm clipping and 5-aminolevulinic acid use for glioma resection, the ICG endoscope may provide useful real-time feedback that may lead to better patient outcomes. However, larger comparative endoscopic studies need to be investigated to draw more definitive conclusions regarding identification and patency of skull base vasculature, the extent of lesion resection, and preservation of neurovascular structures and pituitary function.
Summary Written by: Anand V. Germanwala, MD
PREDICTORS OF POSTCONCUSSION SYNDROME AFTER SPORTS-RELATED CONCUSSION IN YOUNG ATHLETES: A MATCHED CASE–CONTROL STUDY[2]
Study Question: What are predictors of prolonged symptoms and postconcussion syndrome (PCS) after a sports-related concussion in young athletes?
Sports-related concussion is a public health problem affecting American youth. While a majority (~90%) of those who sustain concussions recover to baseline within a week, a minority remain symptomatic for several months. This prolonged manifestation of symptoms (>3 months) is termed PCS. The authors aimed to identify risk factors for young athletes aged 9–18 years developing PCS after sports-related concussion.
The study design was a retrospective case–control study from a single institution's sport concussion clinic database. Forty patients with PCS (symptoms >3 months after injury) were matched 1:2 by age and sex with control patients with <3 weeks of symptoms. Information about demographics, medical/psychiatric/family history, acute-phase postinjury symptoms (at 0–24 h after injury), and subacute phase postinjury symptoms (at 0–3 weeks) were collected. Univariate and multivariate analysis was done to examine the effect of covariates on the outcome of interest, which was the development of PCS.
PCS patients were more likely than control subjects to have a concussion history, delayed concussion symptom onset after injury, migraine headaches, significant life stressors, preinjury preexisting mood disorders or psychiatric illness, and family history of mood disorders or psychiatric illness. Race, insurance status, body mass index, type of sport, helmet use, medications, and the type of symptoms were not associated with increased risk of developing PCS. Final regression analysis showed significant predictors of PCS to be a history of concussion (odds ratio [OR] 1.8, 95% confidence interval [CI] 1.1–2.8, P = 0.016), preinjury mood disorders (OR 17.9, 95% CI 2.9–113.0, P = 0.002), family history of mood disorders (OR 3.1, 95% CI 1.1–8.5, P = 0.026), and delayed concussion symptom onset (OR 20.7, 95% CI 3.2–132.0, P < 0.001).
Perspective: While limited in the small sample size and single institution retrospective design, this study serves to highlight important points about sports-related concussions in youth. The pathophysiology and neurobiology of this disease entity are not yet completely understood by the medical and scientific community. Delayed symptom onset was found to be a strong risk factor for the development of PCS in this study population. This finding suggests the presence of at-risk children who may suffer from consequences of late removal from play after an injury. While sports are a positive part of childhood development and health, the responsibility of weighing those benefits against the risks of neurologic consequences should be taken seriously. The finding that personal or family history of mood or psychiatric disorders is risk factors for the development of PCS points to the need for multidisciplinary care, family-centered assessment, and careful follow-up. A Large-scale prospective studies are needed to further our understanding and advance our ability to diagnose and care for concussions.
Summary Written by: Sandi Lam, MD MBA.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Hide T, Yano S, Shinojima N, Kuratsu J. Usefulness of the indocyanine green fluorescence endoscope in endonasal transsphenoidal surgery. J Neurosurg. 2015. 122: 1185-92
2. Morgan CD, Zuckerman SL, Lee YM, King L, Beaird S, Sills AK. Predictors of postconcussion syndrome after sports-related concussion in young athletes: A matched case-control study. J Neurosurg Pediatr. 2015. 15: 589-98
3. Rapp SR, Case LD, Peiffer A, Naughton MM, Chan MD, Stieber VW. Donepezil for irradiated brain tumor survivors: A phase III randomized placebo-controlled clinical trial. J Clin Oncol. 2015. 33: 1653-9
4. Zaidi HA, Montoure AJ, Dickman CA. Surgical and clinical efficacy of sacroiliac joint fusion: A systematic review of the literature. J Neurosurg Spine. 2015. 23: 59-66

