

- Department of Neurosurgery, Sher I Kashmir Institute of Medical Sciences, Srinagar, Jammu and Kashmir, India
- Department of Neurosurgery, Jawaharlal Nehru Medical College, Aligarh, Uttar Pradesh, India
- Department of Neuroradiology, Sher I Kashmir Institute of Medical Sciences, Srinagar, Jammu and Kashmir, India
Correspondence Address:
Arif H. Sarmast
Department of Neuroradiology, Sher I Kashmir Institute of Medical Sciences, Srinagar, Jammu and Kashmir, India
DOI:10.4103/sni.sni_38_18
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Abrar A. Wani, Arif H. Sarmast, Altaf U. Ramzan, Abdul Q. Khan, Sarabjit S. Chhibber, Nayil K. Malik, Feroz Shaheen. Spinal angiolipoma mimicking a schwannoma: A case report. 10-Apr-2018;9:79
How to cite this URL: Abrar A. Wani, Arif H. Sarmast, Altaf U. Ramzan, Abdul Q. Khan, Sarabjit S. Chhibber, Nayil K. Malik, Feroz Shaheen. Spinal angiolipoma mimicking a schwannoma: A case report. 10-Apr-2018;9:79. Available from: http://surgicalneurologyint.com/surgicalint-articles/spinal-angiolipoma-mimicking-a-schwannoma-a-case-report/
Date of Submission
30-Jan-2018
Date of Acceptance
12-Mar-2018
Date of Web Publication
10-Apr-2018
Abstract
Background:Angiolipomas rarely involve the spinal canal/foramina, and may prove difficult to differentiate from schwannomas.
Case Description:Here we report a patient who presented with a spinal angiolipoma contributing to spinal cord and neural foraminal compression that was difficult to differentiate from a schwannoma.
Conclusion:Spinal angiolipomas rarely involve the spinal canal/foramina. Utilizing neurodiagnostic studies with pathological confirmation, these lesions may be differentiated from schwannomas.
Keywords: Angiolipoma, spine, tumor
INTRODUCTION
Spinal angiolipomas are benign tumors of adipose tissue that rarely involve the spinal neuraxis.[
The two major pathological types include the noninfiltrating vs. infiltrating variants. The former noninfiltrating angiolipomas are more common, well-capsulated lesions; the patient we present had a thoracic lesion.[
CASE REPORT
Clinical and radiographic presentation
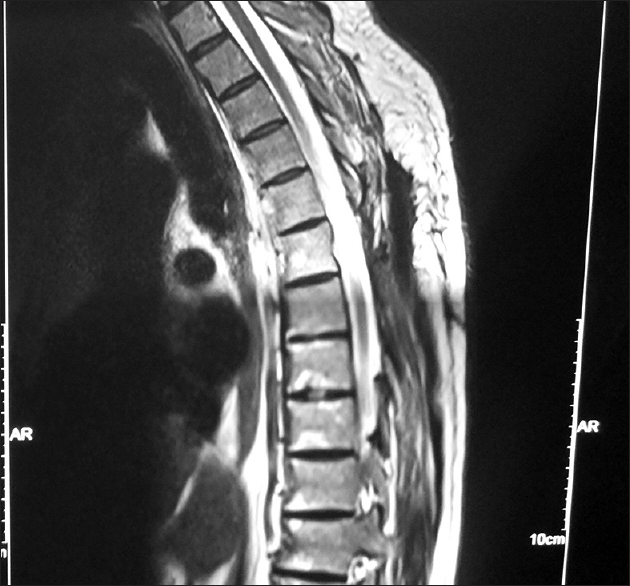
A 60-year-old male presented with progressive weakness in the right (3/5) greater than the left (4/5) lower extremities. The thoracic magnetic resonance imaging (MRI) revealed an extradural tumor at the D-6-7 level that was hyperintense on both T1 and T2-weighted images and enhanced with contrast [

Surgical intervention
During the D-6-7 laminectomy, the tumor was found to extend from dorsal to the dura and into the left neural foramen. Although it first appeared to be a schwannoma, its vascular areas containing well-encapsulated fat were consistent with a fat angiolipoma. Histopathology confirmed this diagnosis, documenting multiple small blood vessels and intervening areas of fat. The postoperative MRI showed no evidence of residual tumor, and the patient regained normal function within five postoperative weeks.
DISCUSSION
Benign infiltrating spinal epidural angiolipomas are rare benign tumors They are composed of mature adipocytes and proliferating blood vessels. They predominantly appear in middle-aged females and males.[
These tumors are divided into two histological subtypes: infiltrating and noninfiltrating (benign).[
Neurodiagnostic studies of angiolipomas
Diagnosing angiolipomas on X-rays, MRI, and CT studies and differentiating them from schwannomas may be difficult. Plain X-rays are usually negative, only showing changes where infiltration of vertebral bodies by tumor causes a loss of trabeculation.[
Pathology
Pathologically, angiolipomas contain mature adipocytes, fibrinous material, and many small blood vessels. Thin fibrous capsules with fibrous septa usually divide these masses into lobules. There are often fibrinous microthrombi within the lumen of its capillaries (e.g., containing some fibrin thrombi).[
Surgery
The mainstay of treatment is complete surgical excision.[
CONCLUSION
Spinal angiolipomas, both the infiltrating and nonfiltrating variants, are rare, well-defined tumors. The treatment for both types is gross total surgical excision. Notably, as patients with residual, infiltrating lesions have good prognoses, they do not require additional radiation therapy.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bardosi A, Schaake T, Friede RL, Roessmann U. Extradural spinal angiolipoma with secretory activity. An ultrastructural, clinico-pathological study. Virchows Arch A Pathol Anat Histopathol. 1985. 406: 253-9
2. Fourney DR, Tong KA, Macaulay RJ, Griebel RW. Spinal angiolipoma. Can J Neurol Sci. 2001. 28: 82-8
3. Gelabert-González M, Agulleiro-Díaz J, Reyes-Santías RM. Spinal extradural angiolipoma, with a literature review. Childs Nerv Syst. 2002. 18: 725-8
4. Gelabert-González M, García-Allut A. Spinal extradural angiolipoma: Report of two cases and review of the literature. Eur Spine J. 2009. 18: 324-35
5. Guzey FK, Bas NS, Ozkan N, Karabulut C, Bas SC, Turgut H. Lumbar extradural infiltrating angiolipoma: A case report and review of 17 previously reported cases with infiltrating spinal angiolipomas. Spine J. 2007. 7: 739-44
6. Hungs M, Paré LS. Spinal angiolipoma: Case report and literature review. J Spinal Cord Med. 2008. 31: 315-8
7. Koul R, Dubey A. Spinal Angiolipoma. Case report. J HK Coll Radiol. 2009. 12: 20-3
8. Labram EK, el-Shunnar K, Hilton DA, Robertson NJ. Revisited: Spinal angiolipoma--three additional cases. Br J Neurosurg. 1999. 13: 25-9
9. Leu NH, Chen CY, Shy CG, Lu CY, Wu CS, Chen DC. MR imaging of an infiltrating spinal epidural angiolipoma. AJNR Am J Neuroradiol. 2003. 24: 1008-11
10. Lin JJ, Lin F. Two entities in angiolipoma. A study of 459 cases of lipoma with review of literature on infiltrating angiolipoma. Cancer. 1974. 34: 720-7
11. Nanassis K, Tsitsopoulos P, Marinopoulos D, Mintelis A, Tsitsopoulos P. Lumbar spinal epidural angiolipoma. J Clin Neurosci. 2008. 15: 460-3
12. Preul MC, Leblanc R, Tampieri D, Robitaille Y, Pokrupa R. Spinal angiolipomas. Report of three cases. J Neurosurg. 1993. 78: 280-6
13. Rabin D, Hon BA, Pelz DM, Ang LC, Lee DH, Duggal N. Infiltrating spinal angiolipoma: A case report and review of the literature. J Spinal Disord Tech. 2004. 17: 456-61
14. Samdani AF, Garonzik IM, Jallo G, Eberhart CG, Zahos P. Spinal angiolipoma: Case report and review of the literature. Acta Neurochir (Wien). 2004. 146: 299-302
15. Sanchez AG, Salvan SR, Garcia PA. Angiolipoma of the cheek: Report of a case. J Oral Maxillofac Surg. 1990. 48: 512-5

