

- Department of Neurosurgery, Sapporo Teishinkai Hospital, Higashi-ku, Sapporo, Hokkaido, Japan.
DOI:10.25259/SNI-16-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Yuto Hatano, Nakao Ota, Kosumo Noda, Yasuaki Okada, Yosuke Suzuki, Shusei Fukuyama, Shuichi Tanada, Atsumu Hashimoto, Tomomasa Kondo, Takanori Miyazaki, Yu Kinoshita, Hiroyasu Kamiyama, Sadahisa Tokuda, Rokuya Tanikawa. Surgical microanatomy of the occipital artery for suboccipital muscle dissection and intracranial artery reconstruction. 28-Jun-2019;10:127
How to cite this URL: Yuto Hatano, Nakao Ota, Kosumo Noda, Yasuaki Okada, Yosuke Suzuki, Shusei Fukuyama, Shuichi Tanada, Atsumu Hashimoto, Tomomasa Kondo, Takanori Miyazaki, Yu Kinoshita, Hiroyasu Kamiyama, Sadahisa Tokuda, Rokuya Tanikawa. Surgical microanatomy of the occipital artery for suboccipital muscle dissection and intracranial artery reconstruction. 28-Jun-2019;10:127. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=9443
Date of Submission
11-Jan-2019
Date of Acceptance
01-May-2019
Date of Web Publication
28-Jun-2019
Abstract
Background: The occipital artery (OA) is an important donor artery for posterior fossa revascularization. Harvesting the OA is difficult in comparison to the superficial temporal artery because the OA runs between suboccipital muscles. Anatomical knowledge of the suboccipital muscles and OA is essential for harvesting the OA during elevation of the splenius capitis muscle (SPL) for reconstruction of the posterior inferior cerebellar artery. We analyzed the running pattern of the OA and its anatomic variations using preoperative and intraoperative findings.
Methods: From April 2012 to March 2018, we surgically treated 162 patients with suboccipital muscle dissection by OA dissection using the lateral suboccipital approach. The running pattern and relationship between the suboccipital muscles and OA were retrospectively analyzed using the operation video and preoperative enhanced computed tomography (CT) images. The anatomic variation in the running pattern of the OA was classified into two types: lateral type, running lateral to the muscle and medial type, running medial to the longissimus capitis muscle (LNG).
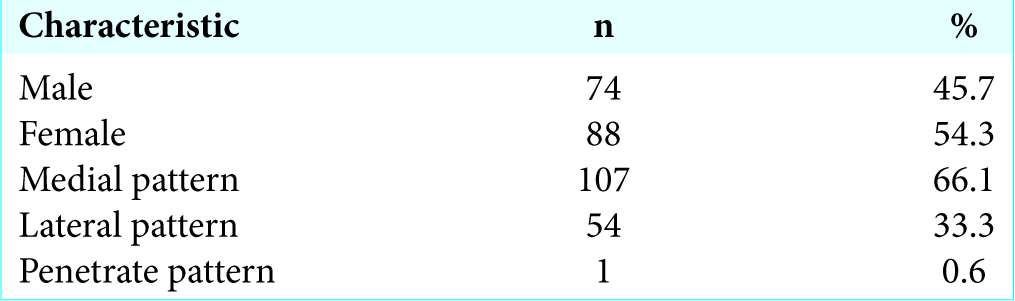
Results: The medial pattern was observed in 107 (66%) patients and the lateral pattern in 54 (33.3%); 1 (0.6%) patient had the OA running between the LNGs.
Conclusion: Preoperative CT is effective in determining the running course of the OA, which is important for safely harvesting the OA during SPL elevation. There is a risk of causing OA injury in patients with the lateral pattern. This is the first report showing that the OA rarely runs in between the LNGs.
Keywords: Occipital artery to posterior inferior cerebellar artery bypass, Occipital artery, Suboccipital muscle dissection
INTRODUCTION
The occipital artery (OA) is often used as an important donor for the reconstruction of the posterior inferior cerebellar artery (PICA) and is rarely available as a donor for the anterior inferior cerebellar artery and posterior cerebral artery.[
MATERIALS AND METHODS
Patients
This study was approved by the institutional review board at our hospital. Patient consent was not required in this study due to its retrospective nature. From April 2012 to March 2018, we surgically treated 162 patients with suboccipital muscle dissection with OA harvesting for the lateral suboccipital approach. The indications were intracranial aneurysms in 79 patients, microvascular decompression in 35, acoustic tumors in 18, other tumors in 27, and other reasons in 3.
Analysis of the running pattern of the occipital artery
The running pattern and relationship between the suboccipital muscles and OA were retrospectively analyzed using operation videos and preoperative enhanced computed tomography (CT) images by the author and discussed with other neurosurgeons. Head CT was performed using a 320- row CT scanner Aquilion ONE VISION edition (Toshiba Medical Systems, Tochigi, Japan). All scans were analyzed in their original format with a 0.5 mm slice thickness scaled to Level 60/Window 200.
The longissimus capitis muscle (LNG) is inserted posterior to the margin of the mastoid process. It is easy to identify the insertion and follow the running course of the LNG using thin-slice CT by changing the window width and level. The other muscles that enter the mastoid process, such as the posterior belly of the digastric muscle and the splenius capitis muscle (SPL), can be distinguished by their insertion and running course [
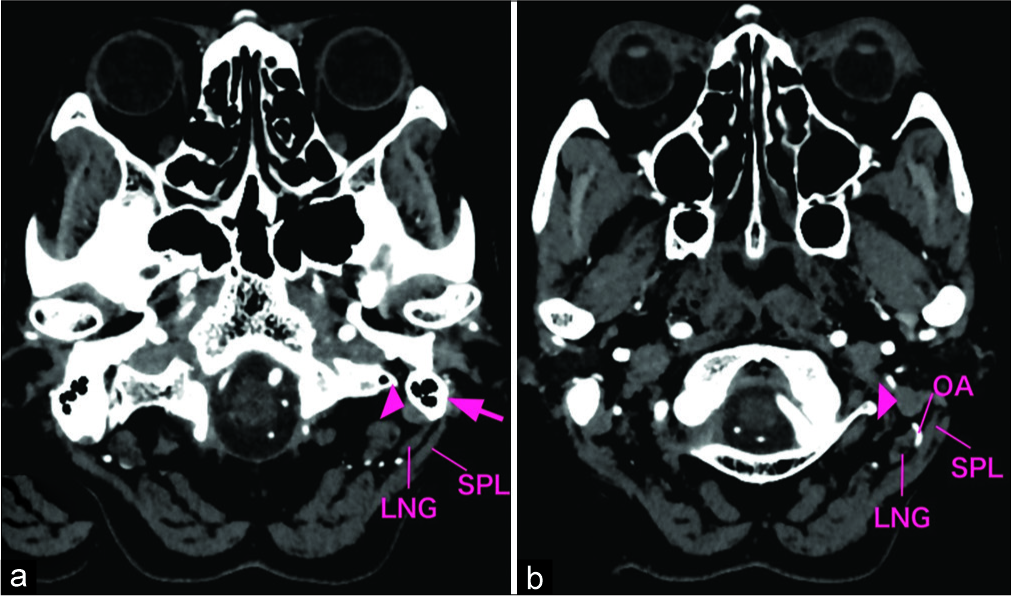
Figure 1:
Enhanced computed tomography images of the suboccipital anatomy (left side). (a) Mastoid process (arrow); arrowhead: posterior belly of the digastric muscle. (b) The lateral running pattern showing an OA running lateral to the LNG. SPL: Splenius capitis muscle; LNG: Longissimus capitis muscle.
Surgical technique
The patient was placed in the park-bench position. The head was fixed and flexed to avoid venous congestion and rotated to the side opposite to the site of the lesion using the stretching neck-shoulder angle, in which the ipsilateral mastoid body could be placed at the highest point for surgery.[
RESULTS
The mean age of the 162 patients included in this study was 57 years, with 88 women and 74 men [
DISCUSSION
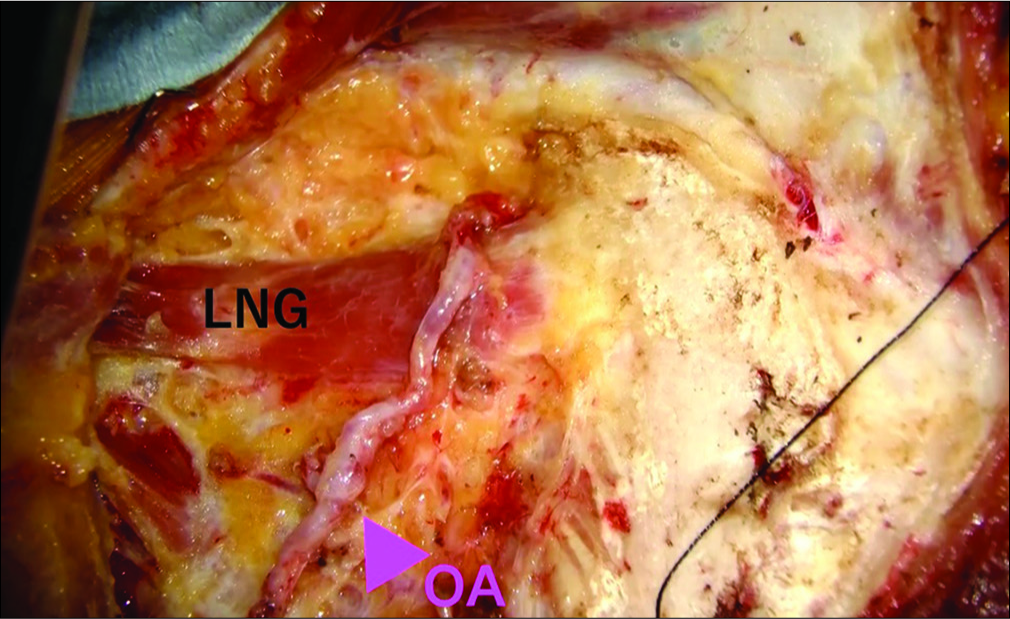
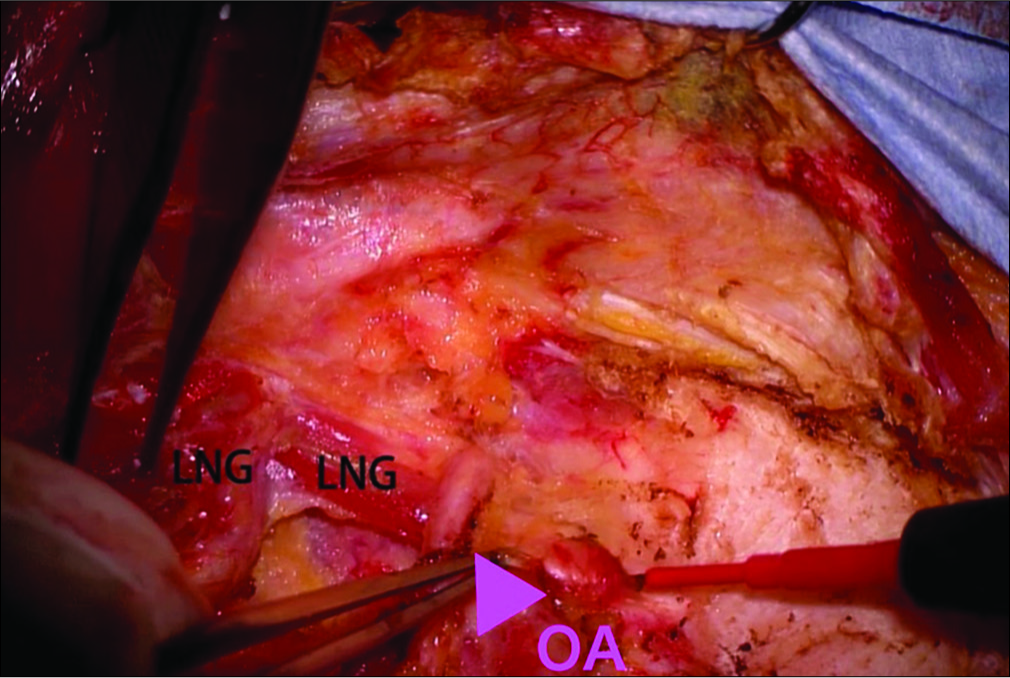
The present study showed that the running pattern of OA can be classified into two types, namely running lateral or medial to the LNG. The medial pattern was observed in approximately 2/3 patients and the lateral pattern in 1/3. Only one patient exhibited an OA running between the LNGs. LNG has been rarely reported to have a superficial and deep insertion since it has multiple muscle bellies (Lang, 1979). This study is the first report that shows the OA running in between the LNGs.
The OA has been widely used as a donor artery for posterior fossa extracranial-intracranial bypass surgery, especially for OA-PICA anastomosis,[
Anatomic variations in the running pattern of the OA were identified around the LNG. SPL elevation is associated with the risk of OA injury in case of the lateral pattern because the tendon of the SPL can be easily confused with the LNG due to their close proximity. The running pattern of OA can be recognized through preoperative enhanced CT images and there were no differences between the intraoperative and preoperative CT findings in this study. Preoperative CT angiography showing the course of the OA superimposed onto the patient’s scalp anatomy can be especially helpful.
The surgical technique used in this study was a widely accepted one. Hence, advancements in this procedure have clinical implications for harvesting the OA. Performing the layer-by-layer muscle dissection can make the operative field wider and shallower in contrast to that achieved in the direct transmuscular approach; thus, making it easy to perform microsurgical anastomosis. In addition, muscle atrophy is less frequent because the muscle belly is not injured. Hence, suboccipital muscle dissection is routinely performed for suboccipital lesions.
The limitations of this study are that it is a retrospective evaluation and includes the unblinded review of the preoperative CT images and intraoperative videos. The frequency of superficial or deep insertion of the LNG is unknown because we could not recognize it during the operation; therefore, we proceeded to detach and confirm the LNG in all operations. Moreover, in this study, only one patient had an OA penetrating through the LNG.
CONCLUSION
Anatomical knowledge of the suboccipital muscles and OA is essential for harvesting the OA as the bypass donor. It is important to understand the variations in the running pattern of the OA and the relationship between suboccipital muscles. In this regard, the present study revealed the effectiveness of preoperative CT imaging to determine the running course of the OA. The findings of this paper can be used as a reference to preoperatively determine the running pattern of the OA to perform the harvest procedure safely and with minimal complications.
References
1. Czabanka M, Ali M, Schmiedek P, Vajkoczy P, Lawton MT. Vertebral artery-posterior inferior cerebellar artery bypass using a radial artery graft for hemorrhagic dissecting vertebral artery aneurysms: Surgical technique and report of 2 cases. J Neurosurg. 2011. 114: 1074-9
2. Fukuda H, Evins AI, Burrell JC, Stieg PE, Bernardo A. A safe and effective technique for harvesting the occipital artery for posterior fossa bypass surgery: A cadaveric study. World Neurosurg. 2014. 82: e459-65
3. Kawashima M, Rhoton AL, Tanriover N, Ulm AJ, Yasuda A, Fujii K. Microsurgical anatomy of cerebral revascularization. Part II: Posterior circulation. J Neurosurg. 2005. 102: 132-47
4. Khodadad G. Short-and long-term results of microvascular anastomosis in the vertebrobasilar system, a critical analysis. Neurol Res. 1981. 3: 33-65
5. Kubota H, Tanikawa R, Katsuno M, Izumi N, Noda K, Ota N. Vertebral artery-to-vertebral artery bypass with interposed radial artery or occipital artery grafts: Surgical technique and report of three cases. World Neurosurg. 2014. 81: 202.e1-8
6. Ota N, Goehre F, Miyazaki T, Kinoshita Y, Matsukawa H, Yanagisawa T. Bypass revascularization applied to the posterior cerebral artery. World Neurosurg. 2016. 96: 460-72
7. Ota N, Tanikawa R, Miyama M, Miyazaki T, Kinoshita Y, Matsukawa H. A contralateral transcondylar fossa approach with bilateral V3 segment exposure for repairing complex vertebral artery aneurysms. World Neurosurg. 2017. 99: 340-7
8. Ota N, Tanikawa R, Yoshikane T, Miyama M, Miyazaki T, Kinoshita Y. Surgical microanatomy of the posterior condylar emissary vein and its anatomical variations for the transcondylar fossa approach. Oper Neurosurg (Hagerstown). 2017. 13: 382-91
9. Tanikawa R, Sugimura T, Seki T, Izumi N, Noda K, Hashimoto M. Basic surgical techniques and pitfalls in vascular reconstruction in the posterior fossa: Surgical anatomy for oa-pica anastomosis. Jpn J Neurosurg. 2008. 17: 587-95

