

- Department of Neurosurgery, Sher-I-Kashmir Institute of Medical Sciences, Srinagar, Jammu and Kashmir, India
- Department of Obstetrics and Gynaecology, Government Lalla Ded Hospital, Srinagar, Jammu and Kashmir, India
Correspondence Address:
Arif Hussain Sarmast
Department of Neurosurgery, Sher-I-Kashmir Institute of Medical Sciences, Srinagar, Jammu and Kashmir, India
DOI:10.4103/2152-7806.180088
Copyright: © Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Laharwal MA, Sarmast AH, Ramzan AU, Wani AA, Malik NK, Arif SH, Rizvi M. Epidemiology of the neural tube defects in Kashmir Valley. Surg Neurol Int 11-Apr-2016;7:35
How to cite this URL: Laharwal MA, Sarmast AH, Ramzan AU, Wani AA, Malik NK, Arif SH, Rizvi M. Epidemiology of the neural tube defects in Kashmir Valley. Surg Neurol Int 11-Apr-2016;7:35. Available from: http://surgicalneurologyint.com/surgicalint_articles/epidemiology-of-the-neural-tube-defects-in-kashmir-valley/
Abstract
Background:Neural tube defects (NTDs) are the most common congenital malformations affecting the brain and spinal cord and have a multifactorial etiology. Genetic and environmental factors have been found to cause these defects, both individually and in combination.
Methods:A 2-year hospital-based prospective study was carried out from November 2013 to October 2015 to determine the incidence, types, demographics, risk factors, and other associated anamolies relevant to NTDs in Kashmir Valley. A detailed history of the mother was taken along with detailed clinical examination of neonate including measurement of head circumference and checking the status of fontanella, whether lax/full/bulging/or tense, type of NTD. Investigations that were done included were X-ray skull: Anterior-posterior (AP) and lateral, X-ray spine: AP and lateral, ultrasonography abdomen, magnetic resonance imaging: Spine and brain.
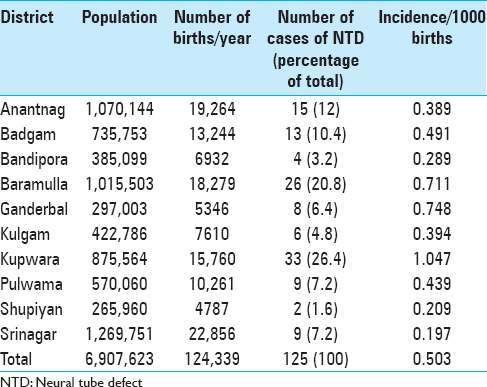
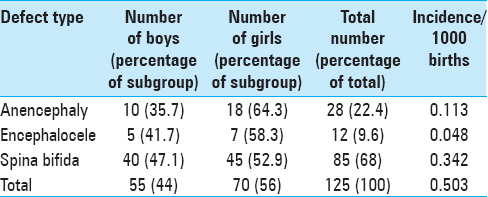
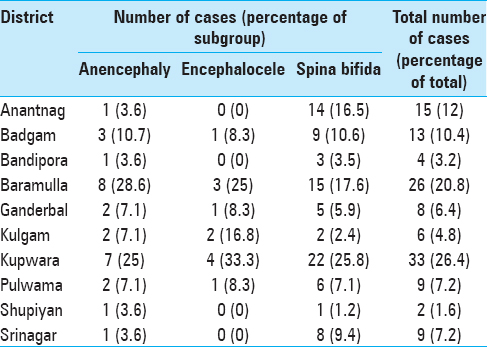
Results:The total number of babies with NTD's was 125 with an overall incidence of 0.503. Kupwara district was having the highest incidence (1.047) and Srinagar district the lowest incidence of NTD's (0.197). Majority of NTD's (116 cases, 92.8%) were found in the rural areas. Among the different types of NTD's, spina bifida had an incidence of 0.342 (85 cases, 68%) and anencephaly had an incidence of 0.113 (28 cases, 22.4%). There was a slight preponderance of females over males with NTD's. There were 70 females (56%) and 55 males (44%), respectively, with a male: female ratio of 0.8:1
Conclusions:The incidence rates of NTDs is very high for Kashmir Valley. Geographical distribution of NTDs at this place confirms a relationship between the socioeconomic status, educational status, maternal too young or advanced age, and environmental factors for the development of a NTD. The results of this study point to the importance establishing a health policy to prevent NTD in Kashmir Valley.
Keywords: Kashmir, meningoceles, myeloceles, myelomeningoceles, neural tube defects
INTRODUCTION
Neural tube defects in Kashmir valley
Neural tube defects (NTDs) are the most common congenital malformations affecting the brain and spinal cord. They assume significance by virtue of their morbidity, mortality, health care expenditure, and human suffering. These defects can be categorized into two groups: Open defects and closed defects. Open defects where the neural tissue is exposed to the air (or amniotic fluid) include spina bifida (SB) cystica, which encompasses meningoceles, myeloceles, and myelomeningoceles. Myelomeningocele is a defect in the closure of the neural tube that occurs in the vertebral column. This type of defect can occur anywhere along the spinal column, but is more likely to be placed in thelumbo-sacral region. Closed defects in which the skin completely covers the neural tissue, include occult spinal dysraphism, which encompasses diastematomyelia, dorsal dermal sinus, and tight filum terminale. SB occulta refers strictly to bone fusion defects of the lower spine, generally in the lumbo-sacral region. Anencephaly is a defect in which the head end of the neural tube does not close; this results in the lack of a cranial vault and cerebral hemispheres.[
NTD's have a multifactorial etiology.[
MATERIALS AND METHODS
The present study “Epidemiology of The NTDs in Kashmir Valley” – A hospital-based prospective study was conducted in the Neurosurgical Centre of Sher-I-Kashmir Institute of Medical Sciences (SKIMS), Srinagar, the only referral center for neurological/neurosurgical problems (hence all cases of NTDs are referred here) and at the Lal Ded Women's Obstetrical/Gynecological Disease Hospital, Srinagar; the main referral center for obstetrical/gynecological disease, situated in the center of Kashmir Valley. The study was conducted over a period of 2 years from November 2013 to October 2015.
A detailed history of the mother was taken with special impetus on age, occupation: Housewife/professional worker, dietary history-fruit intake, vegetarian/nonvegetarian diet, smoking/drug addiction – type/duration, exposure to fertilizers, folic acid/vitamin intake, any other drugs, number of times conceived/abortions/intrauterine fetal deaths/previous malformations, mode of delivery, hypertension treatment/drug defaulter, diabetes – duration and type, tuberculosis, Cardiovascular (CVS) disease, epilepsy – type and duration, etc., and examination of the neonate done at Lal Ded Hospital detailed clinical examination of neonate included general physical examination, head circumference, fontanella-lax/full/bulging/tense
Type of neural tube defect
Anencephaly, encephalocele, myelomeningocele, meningocele, lipomeningocele, SB occulted, etc., site of defect: Cranial/cervical/dorsal/lumbar/sacral. Characteristics of defect: Skin covered or not/leaking or not/transilluminant or not, presence or absence of skin dimple, sinus, hemangioma, hypertrichosis, etc., spine: Normal/scoliosis/kyphosis., other associated malformations, cleft palate, cleft lip, talipes equinovarus hypospadias, etc.
Complete neurological examination of neonate with following, Investigations done were X-ray skull: Anterior-posterior (AP) and lateral, X-ray spine: AP and lateral, ultrasonography: Abdomen, magnetic resonance imaging: Spine and brain.
To gauge the most accurate epidemiological pattern of NTD's in Kashmir Valley, the patients referred from regions of the state of Jammu and Kashmir other than the valley were excluded from this study.
For statistical analysis, the total number of deliveries in different districts of the Kashmir Valley during the study period was obtained from the Department of Population Research, University of Kashmir, which was calculated on the basis of prevailing crude birth rate (taken as average of last 3 years) by the Ministry of Health and Family Welfare, Jammu and Kashmir state.
The neural tube defects were categorized into three main types:
Anencephaly: A congenital malformation characterized by the total or partial absence of the cranial vault, the covering skin, and the brain missing or reduced to a small mass Encephalocoele: A congenital malformation characterized by herniation of the brain and/or meninges through a defect in the skull. Encephalocoele is not counted as a separate defect when present with SB SB: A family of congenital malformation defects in the closure of the spinal column characterized by herniation or exposure of the spinal cord and/or meninges through an incompletely closed spine. This definition includes meningocele, meningomyelocele, myelocele, myelomeningocele, and rachischisis. SB is not counted as a separate defect when present with anencephalus.
Disease frequency was measured by incidence rates.
Incidence rates of NTD's was calculated by the formula:
Comparisons were made with other studies conducted by various people from time to time with regards to incidence and possible risk factors.
OBSERVATIONS AND RESULTS
Kashmir Valley is topographically and geographically different from the rest of India. It is situated at an altitude of 5000–6000 feet, between 33.5° and 35° north latitudes and 74–76° east longitude. It has ten districts and a total population of 6,907,623 with a district wise distribution as shown in
Mothers of six neonates, in our study, were smokers (hooka smoker). None of the mothers was alcoholic. Mother of only one case was having hypertension and was regularly using amlodipine. Mother of one case was having epilepsy and was on sodium valproate which she had used throughout the pregnancy. None of the mothers gave history of diabetes. Mothers of five neonates were of non-Kashmiri origin (four Bengalis and one Maharashtrian) married to Kashmiri male.
DISCUSSION
Overall incidence
The incidence of NTDs varies not only from country to country but also from region to region within a country. The incidence of NTDs, in our study, was 0.503/1000 live births. Nikkilä et al.[
Incidence of subgroups
The incidence of various types of NTD's, in our study, was anencephaly (0.113/1000 live births), encephalocele (0.048/1000 live births), and SB (0.342/1000 live births). Thunem et al.[
Male:female ratio
In our study, there was a slight preponderance of females over males with NTD's in total (male:female ratio of 0.8:1) as well as in sub groups. This is in concordance with the study of Jorde et al.,[
Maternal age
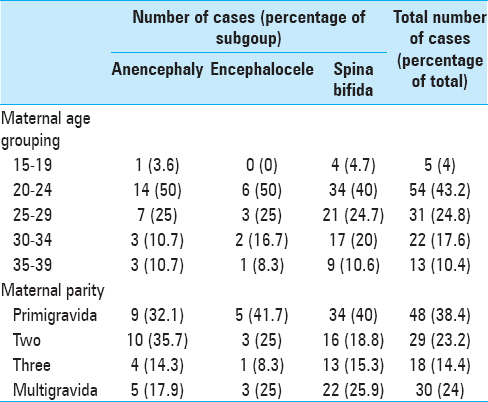
In our study, we found that most of the NTD's 54 (43.2%) including the subgroups of NTD's i.e., 14 patients (50%) of anencephaly, 6 patients (50%) of encephalocele, and 34 (40%) patients of SB occurred in mothers of younger age group (20–24 years). A number of studies have reported maternal age risk for NTD's to be U-shaped, i.e., highest among youngest and oldest women, while other studies have found risk to decrease with increasing age or the reverse.[
Parity
In our study, the highest number of NTD's was found in primigravidas 48 cases (38.4%) followed by multigravidas 30 cases (24%). This is in concordance with the study of Little and Elwood[
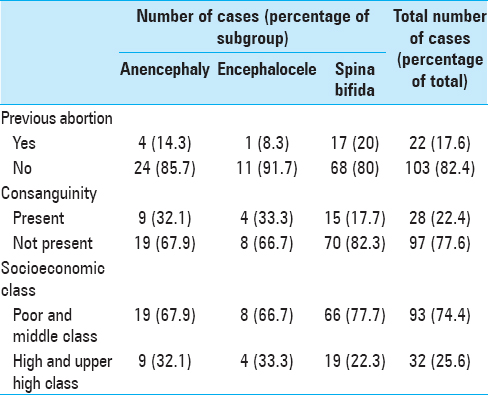
Prior abortions
In our study, 82.4% of mothers did not give history of previous abortion. Whiteman et al.[
Consanguinity
About 77.6% of the cases of NTD, in our study, were a product of nonconsanguineous marriage. In concordance with our study, Asindi and Al-Shehri,[
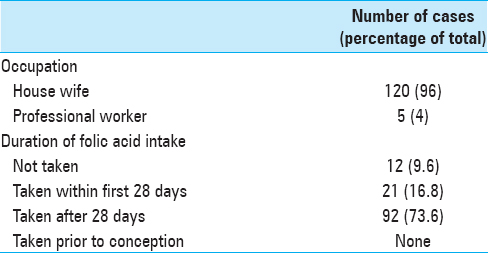
Occupation of mother
In our study, 12 (96%) mothers were housewife. Although a number of studies have shown an increased risk of NTD's in mothers with occupation like cleaning, healthcare,[
Socioeconomic status
Majority of the cases, i.e., 93 (74.4%), in our study, belonged to low or middle class families. The SES of the families was assessed by modified Prasad's classification. This finding goes in concordance with other studies where increased incidences of NTD's have been found in families of low SES. Blanco Muñoz et al.,[
Educational status of parents
Majority of the mothers, i.e., 82 (65.6%), in our study, were illiterate and majority of fathers, i.e., 84 (67.2%) though literate were undergraduates. In concordance with our study Grewal et al.,[
Folic acid intake
Majority of the mothers, i.e., 92 (73.6%), in our study, had taken folic acid after 28 days of conception. Only 12 (9.6%) of the mothers had consumed folic acid within 28 days of conception and none before conception. In patients who have a family history of an NTD, folic acid taken orally on a daily basis is shown to lower the occurrence and recurrence of NTD's in their own offspring and in their relatives. The Medical Research Council (Group MRCVSR 1991)[
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
Commentary
- Bombay Hospital Institute of Medical Sciences, Mumbai, Maharashtra, India. E-mail:
E-mail: cdeopujari@hotmail.com
Study of the “Prevalence of Neural Tube Defects in India” is important as a higher incidence is presumed to occur compared to the western world, and a wide variation in various regions within the country has been reported. The prevalence rate all over India is reported to be 6.63/1000 births, the highest being reported from the northern states of Punjab, Uttar Pradesh, and Bihar.[
The majority of the studies included in these reviews are hospital-based except a few community-based study in North India (Balrampur, Uttar Pradesh) which showed a prevalence of 8.2/1000 births.[
Kashmir is further north of Haryana and this may partly explain the higher incidence in the accompanying paper. The detailed analysis of various districts in the Kashmir valley is a unique feature of this study. Although this study is based on hospital-based statistics, this relatively isolated geographic area with limited health facilities has made the study almost a community-based survey. The study also shows that the majority defects occurred in the rural area, in relatively lower socioeconomic group, especially in young mothers. Most mothers took folic acid for several weeks into pregnancy, but none took folic acid before conception. Maternal malnutrition has been suggested as the main cause in India and suggested strategies including food fortification, vitamin supplementation, and dietary modification.[
Although India has witnessed a substantial decrease in infant mortality attributed to infectious diseases and malnutrition, significant reduction in neural tube defects has not been seen in many areas, emphasizing further the need for greater attention to this problem.
References
1. Agarwal SS. Neural tube defect: A preventable congenital malformation. Indian Pediatr. 1999. 36: 643-8
2. Asindi A, Al-Shehri A. Neural tube defects in the Asir Region of Saudi Arabia. Ann Saudi Med. 2001. 21: 26-9
3. Berry RJ, Li Z, Erickson JD, Li S, Moore CA, Wang H. Prevention of neural-tube defects with folic acid in China. China-U.S Collaborative project for neural tube defect prevention. N Engl J Med. 1999. 341: 1485-90
4. Blanco Muñoz J, Lacasaña M, Borja Aburto VH, Torres Sánchez LE, García García AM, López Carrillo L. Socioeconomic factors and the risk of anencephaly in a Mexican population: A case-control study. Public Health Rep. 2005. 120: 39-45
5. Blatter BM, Roeleveld N, Zielhuis GA, Gabreëls FJ, Verbeek AL. Maternal occupational exposure during pregnancy and the risk of spina bifida. Occup Environ Med. 1996. 53: 80-6
6. Brender J, Suarez L, Hendricks K, Baetz RA, Larsen R. Parental occupation and neural tube defect-affected pregnancies among Mexican Americans. J Occup Environ Med. 2002. 44: 650-6
7. Cabrera RM, Hill DS, Etheredge AJ, Finnell RH. Investigations into the etiology of neural tube defects. Birth Defects Res C Embryo Today. 2004. 72: 330-44
8. Hook EB. Congenital malformations worldwide: A report from the international clearinghouse for birth defect monitoring systems. Am J Hum Genet. 1992. 51: 919-20
9. Detrait ER, George TM, Etchevers HC, Gilbert JR, Vekemans M, Speer MC. Human neural tube defects: Developmental biology, epidemiology, and genetics. Neurotoxicol Teratol. 2005. 27: 515-24
10. Elwood JH, Elwood JM. Investigation of area differences in the prevalence at birth of anencephalus in Belfast. Int J Epidemiol. 1984. 13: 45-52
11. Elwood JM, Little J, Elwood JH.editorsEpidemiology and Control of Neural Tube Defects. New York: Oxford University Press; 1992. p.
12. Farley TF, Hambidge SJ, Daley MF. Association of low maternal education with neural tube defects in Colorado, 1989-1998. Public Health. 2002. 116: 89-94
13. Frey L, Hauser WA. Epidemiology of neural tube defects. Epilepsia. 2003. 44: 4-13
14. Grewal J, Carmichael SL, Song J, Shaw GM. Neural tube defects: An analysis of neighbourhood- and individual-level socio-economic characteristics. Paediatr Perinat Epidemiol. 2009. 23: 116-24
15. Jorde LB, Fineman RM, Martin RA. Epidemiology of neural tube defects in Utah, 1940-1979. Am J Epidemiol. 1984. 119: 487-95
16. Kaufman BA. Neural tube defects. Pediatr Clin North Am. 2004. 51: 389-419
17. Kulkarni ML, Mathew MA, Ramachandran B. High incidence of neural-tube defects in South India. Lancet. 1987. 1: 1260-
18. Kulkarni ML, Mathew MA, Reddy V. The range of neural tube defects in Southern India. Arch Dis Child. 1989. 64: 201-4
19. Lemire RJ. Neural tube defects. JAMA. 1988. 259: 558-62
20. Little L, Elwood JM, Kiley M.editors. Epidemiology of neural tube defects. Reproductive and Perinatal Epidemiology. Boston: CRC Press; 1991. p. 251-336
21. Mathews TJ.editors. Trends in spina bifida and anencephalus in the United States, 1991-2005. Hyattsville, MD: National Center for Health Statistics; 2007. p.
22. McDonnell RJ, Johnson Z, Delaney V, Dack P. East Ireland 1980-1994: Epidemiology of neural tube defects. J Epidemiol Community Health. 1999. 53: 782-8
23. Mutchinick O, Orozco E, Lisker R, Babinsky V, Núñez C. Risk factors associated with neural tube defects: Exposure during the first trimester of gestation. Gac Med Me×. 1990. 126: 227-33
24. Myrianthopoulos NC, Melnick M. Studies in neural tube defects. I. Epidemiologic and etiologic aspects. Am J Med Genet. 1987. 26: 783-96
25. Nikkilä A, Rydhström H, Källén B. The incidence of spina bifida in Sweden 1973-2003: The effect of prenatal diagnosis. Eur J Public Health. 2006. 16: 660-2
26. . Prevention of neural tube defects: Results of the Medical Research Council Vitamin Study. MRC Vitamin Study Research Group. Lancet. 1991. 338: 131-7
27. Rouhani P, Fleming LE, Frías J, Martínez-Frías ML, Bermejo E, Mendioroz J. Pilot study of socioeconomic class, nutrition and birth defects in Spain. Matern Child Health J. 2007. 11: 403-5
28. Sharma AK, Upreti M, Kamboj M, Mehra P, Das K, Misra A. Incidence of neural tube defects of Lucknow over a 10 year period from 1982-1991. Indian J Med Res. 1994. 99: 223-6
29. Strassburg MA, Greenland S, Portigal LD, Sever LE. A population-based case-control study of anencephalus and spina bifida in a low-risk area. Dev Med Child Neurol. 1983. 25: 632-41
30. Thulstrup AM, Bonde JP. Maternal occupational exposure and risk of specific birth defects. Occup Med (Lond). 2006. 56: 532-43
31. Thunem NY, Lowry RB, Tucker BJ, Medd BW. Birth prevalence and recurrence rates of neural tube defects in Southern Alberta in 1970-81. CMAJ. 1988. 138: 819-23
32. Velie EM, Shaw GM. Impact of prenatal diagnosis and elective termination on prevalence and risk estimates of neural tube defects in California, 1989-1991. Am J Epidemiol. 1996. 144: 473-9
33. Vieira AR, Castillo Taucher S. Maternal age and neural tube defects: Evidence for a greater effect in spina bifida than in anencephaly. Rev Med Chil. 2005. 133: 62-70
34. Whiteman D, Murphy M, Hey K, O’Donnell M, Goldacre M. Reproductive factors, subfertility, and risk of neural tube defects: A case-control study based on the Oxford record linkage study register. Am J Epidemiol. 2000. 152: 823-8
35. Allagh KP, Shamanna BR, Murthy GV, Ness AR, Doyle P, Neogi SB. Birth prevalence of neural tube defects and orofacial clefts in India: A systematic review and meta-analysis. PLoS One. 2015. 10: e0118961-
36. Cherian A, Seena S, Bullock RK, Antony AC. Incidence of neural tube defects in the least-developed area of India: A population-based study. Lancet. 2005. 366: 930-1
37. Gupta P, Gupta A. Awareness regarding use of folic acid for prevention of congenital neural tube defects. Natl Med J India. 2000. 13: 105-
38. Sharma JB, Gulati N. Potential relationship between dengue fever and neural tube defects in a northern district of India. Int J Gynaecol Obstet. 1992. 39: 291-5
39. Verma IC. Burden of genetic disorders in India. Indian J Pediatr. 2000. 67: 893-8

