

- Department of Neurosurgery, Albert Einstein College of Medicine of Yeshiva University, Montefiore Medical Center, Bronx, NY 10467, USA
- Department of Neuroradiology, Albert Einstein College of Medicine of Yeshiva University, Montefiore Medical Center, Bronx, NY 10467, USA
Correspondence Address:
Jonathan Nakhla
Department of Neurosurgery, Albert Einstein College of Medicine of Yeshiva University, Montefiore Medical Center, Bronx, NY 10467, USA
DOI:10.4103/2152-7806.175072
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nakhla J, Nasser R, Yassari R, Pasquale D, Altschul D. Ruptured anterior spinal artery aneurysm from a herniated cervical disc. A case report and review of the literature. Surg Neurol Int 28-Jan-2016;7:10
How to cite this URL: Nakhla J, Nasser R, Yassari R, Pasquale D, Altschul D. Ruptured anterior spinal artery aneurysm from a herniated cervical disc. A case report and review of the literature. Surg Neurol Int 28-Jan-2016;7:10. Available from: http://surgicalneurologyint.com/surgicalint_articles/ruptured-anterior-spinal-artery-aneurysm-from-a-herniated-cervical-disc-a-case-report-and-review-of-the-literature/
Abstract
Background:Subarachnoid hemorrhage (SAH) caused by a ruptured cervical anterior spinal artery aneurysm is extremely rare and in the setting of cervical spondylosis. This case presentation reviews the diagnosis, management, and treatment of such aneurysms.
Case Presentation:An 88-year-old female presented with the worst headache of her life without focal deficits. She was found to have diffuse SAH in the basal cisterns extending inferiorly down the spinal canal. Review of the neurodiagnostic images revealed an anterior spinal artery aneurysm in the setting of cervical spondylosis.
Conclusions:Clinicians should be suspicious of cervical spondylosis as a rare etiology for an SAH when cerebral angiograms prove negative for intracranial aneurysms.
Keywords: Aneurysm, cervical, spine, subarachnoid hemorrhage, trauma
BACKGROUND
Spontaneous subarachnoid hemorrhages (SAH) caused by spinal artery aneurysms are exceedingly rare. Vincent in 1981 first reported the angiographic finding of an anterior spinal artery rupture.[
CASE DESCRIPTION
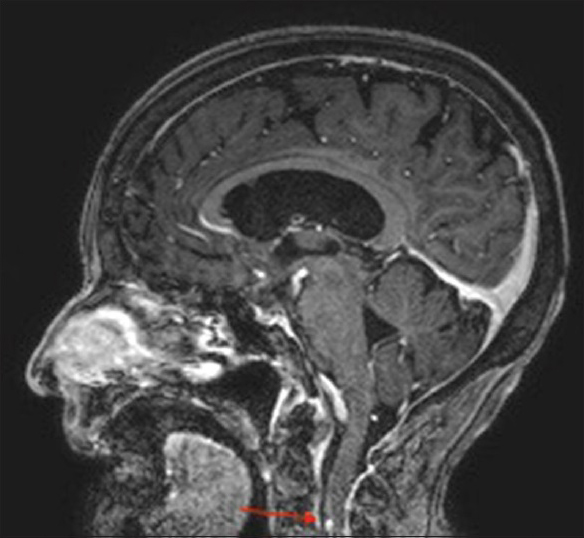
An 88-year-old female with a history of anemia and hypertension presented to the emergency room with the acute onset of the worst headache of her life after walking into a supermarket. On neurological examination, she had no focal deficits; her only complaint was a severe global headache and neck pain. A computed tomography (CT) scan of the head and cervical spine revealed diffuse acute SAH within the basal cisterns that extended inferiorly down to through the cervical-medullary junction, attended by mild acute hydrocephalus [Figures



CONCLUSION
Frequency and etiology of spinal aneurysms
Less than 1% of SAHs result from ruptured spinal aneurysms.[
Location of spinal aneurysms
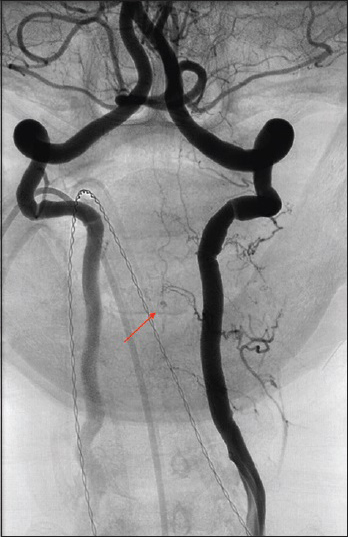
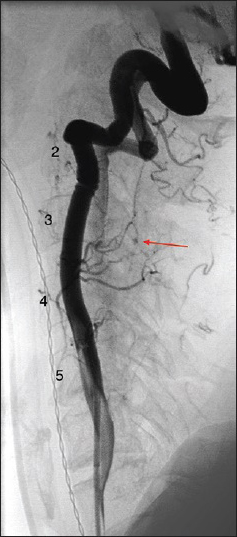
Although the majority of spinal aneurysms are located in the thoracic spine, in this case, it was found at the C5–C6 level.[
Treatment of spinal aneurysms
The treatment of spinal aneurysms poses significant technical challenges with attendant severe complications.[
Conservative treatment of spinal aneurysms
There is insufficient data on the historical outcomes of spinal artery aneurysms treated without any intervention (e.g., rebleed rates).[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Berlis A, Scheufler KM, Schmahl C, Rauer S, Götz F, Schumacher M. Solitary spinal artery aneurysms as a rare source of spinal subarachnoid hemorrhage: Potential etiology and treatment strategy. AJNR Am J Neuroradiol. 2005. 26: 405-10
2. Boeris D, Mortimer A, Sakthithasan M, Evins AI, Sandeman D, Renowden S. Conservative management of a post-traumatic pseudoaneurysm of the artery of cervical enlargement-anterior spinal artery junction. J Neurointerv Surg. 2015. p.
3. Gutierrez Romero D, Batista AL, Gentric JC, Raymond J, Roy D, Weill A. Ruptured isolated spinal artery aneurysms. Report of two cases and review of the literature. Interv Neuroradiol. 2014. 20: 774-80
4. Karakama J, Nakagawa K, Maehara T, Ohno K. Subarachnoid hemorrhage caused by a ruptured anterior spinal artery aneurysm. Neurol Med Chir (Tokyo). 2010. 50: 1015-9
5. Lavoie P, Raymond J, Roy D, Guilbert F, Weill A. Selective treatment of an anterior spinal artery aneurysm with endosaccular coil therapy. Case report. J Neurosurg Spine. 2007. 6: 460-4
6. Longatti P, Sgubin D, Di Paola F. Bleeding spinal artery aneurysms. J Neurosurg Spine. 2008. 8: 574-8
7. Massand MG, Wallace RC, Gonzalez LF, Zabramski JM, Spetzler RF. Subarachnoid hemorrhage due to isolated spinal artery aneurysm in four patients. AJNR Am J Neuroradiol. 2005. 26: 2415-9
8. Peltier J, Bougeois P, Baroncini M, Thines L, Leclerc X, Lejeune JP. Ultra-early rebleeding of an anterior spinal artery aneurysm. Br J Neurosurg. 2010. 24: 468-70
9. Rosenørn J, Eskesen V, Schmidt K, Rønde F. The risk of rebleeding from ruptured intracranial aneurysms. J Neurosurg. 1987. 67: 329-32
10. Vincent FM. Anterior spinal artery aneurysm presenting as a subarachnoid hemorrhage. Stroke. 1981. 12: 230-2

