

- Department of Neurosurgery, Fujita Health University Banbuntane Hospital,
- Department of Neurosurgery, Graduate School of Medicine, Nagoya University, Division of Neuroendoscope and Pituitary Surgery, Nagoya, Aichi, Japan,
- Department of Neurosurgery, Uttar Pradesh University of Medical Sciences, Etawah, Uttar Pradesh, India,
- Department of Gastroenterology, Fujita Health University Banbuntane Hospital, Nagoya, Aichi, Japan.
Correspondence Address:
Ahmed Ansari
Department of Gastroenterology, Fujita Health University Banbuntane Hospital, Nagoya, Aichi, Japan.
DOI:10.25259/SNI_354_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Riki Tanaka1, Kazuhito Takeuchi2, Ahmed Ansari3, Kento Sasaki1, Kyosuke Miyatani1, Yasuhiro Yamada1, Tsukasa Kawase1, Yoko Kato1, Akihiko Horiguchi4. Endoscopic-assisted paramedian infratentorial supracerebellar approach for pineal cyst – How I do it Video clip. 15-Oct-2020;11:336
How to cite this URL: Riki Tanaka1, Kazuhito Takeuchi2, Ahmed Ansari3, Kento Sasaki1, Kyosuke Miyatani1, Yasuhiro Yamada1, Tsukasa Kawase1, Yoko Kato1, Akihiko Horiguchi4. Endoscopic-assisted paramedian infratentorial supracerebellar approach for pineal cyst – How I do it Video clip. 15-Oct-2020;11:336. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=10336
Date of Submission
14-Jun-2020
Date of Acceptance
22-Aug-2020
Date of Web Publication
15-Oct-2020
Abstract
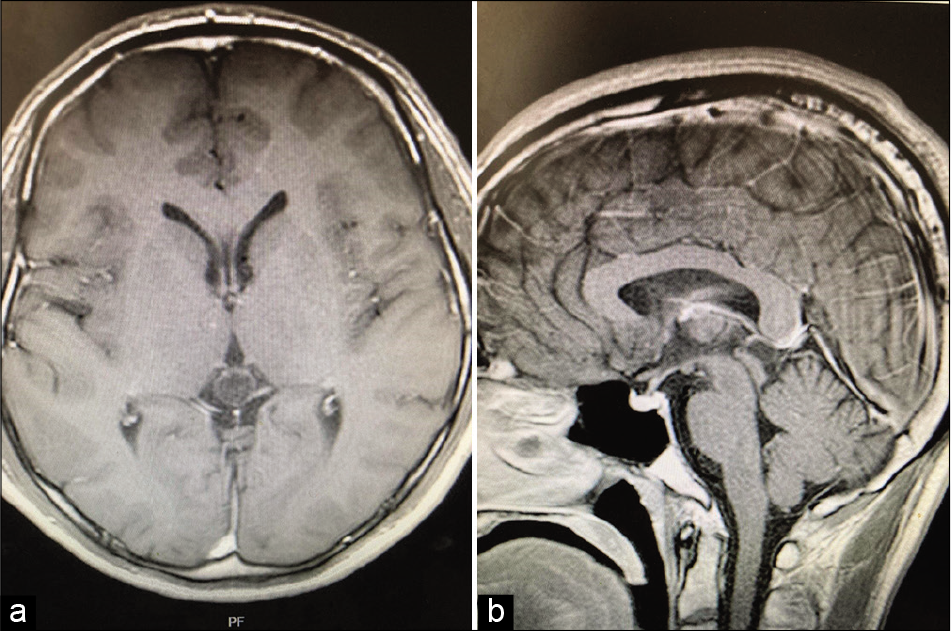
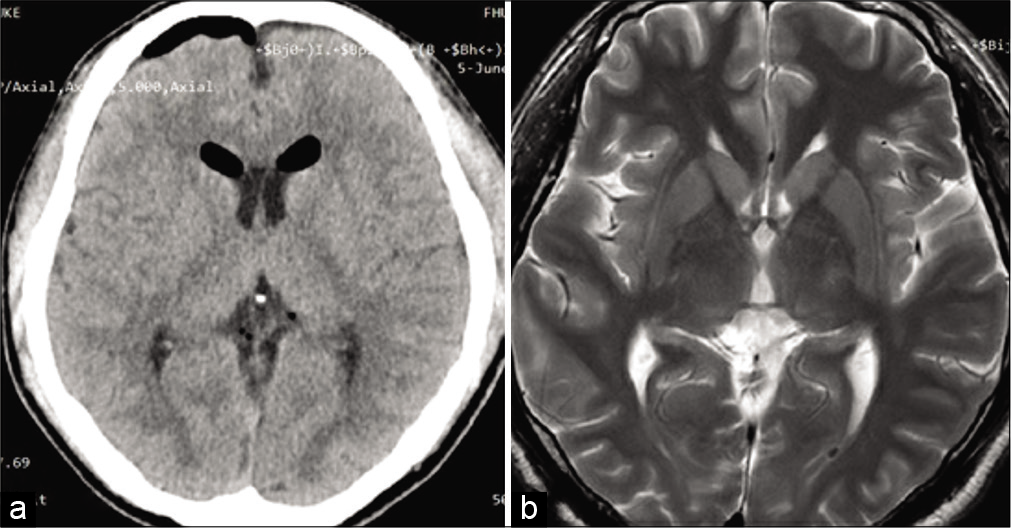
Background: The endoscopic supracerebellar-infratentorial (SCIT) approach is a viable method to access pathology of the posterior incisura, but a narrow working space and frequent instrument conflict can potentially limit its surgical efficacy. We planned an endoscopic-assisted paramedian infratentorial supracerebellar approach for pineal cyst.
Case Description: Patient was placed in prone position under general anesthesia. His head was rotated to the left side slightly. The location of the transverse sinus was detected with navigation system. A 5 cm linear skin incision was performed, and a 2 cm craniectomy was performed about 2 cm left of the median. The transverse sinus was little bit exposed. Dura was incised in a U-shaped incision with the transverse sinus at the base. The endoscope was advanced along with the culmen. At that time, we observed inferior and superior vermian vein. After reaching to the thick arachnoid near by galenic system, the arachnoid membrane was incised and the CSF was evacuated. After that, the cerebellum became soft and the surgical corridor became large. The arachnoid membrane was incised widely. Pineal cyst, precentral cerebellar vein, bilateral internal occipital vein and great vein of galen were exposed. There were some small veins on the pineal cyst, but the adhesion was not so severe. The cyst was dissected from these small veins. There was no adhesion between the cyst and surrounding brain except for the pineal recess. Bilateral ICV was seen behind the cyst. There was feeding artery and draining vein on the antero-lateral part of the cyst. These vessels were coagulated and cut, then the cyst was removed. After the removal, we confirmed complete removal of the cyst and hemostasis.
Conclusion: Endoscopic-assisted paramedian SCIT approach for pineal cyst in prone position is a reasonable and efficient access for posterior third ventricular lesions. The learning curve, maneuverability in small space, and instrument conflict limit efficacy.
Keywords: Endoscopic assisted, Paramedian, Pineal tumor, Supracerebellar infratentorial
Annotations [ Figures 1 and 2 ]
00:01 - 2 cm craniotomy. 00:14 - Cerebellum was carefully retracted. 00:18 - Arachnoid membrane was incised and CSF evacuated. 00:33 - Surgical corridor became wide. 00:36 - Thick arachnoid was incised to expose pineal cyst and Galenic system. 01:15 - Pineal cyst was exposed and dissected. 02:15 - Pineal cyst removed from pineal recess.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.

