

- Department of Neurosurgery, Kanazawa University, Kanazawa, Japan
Correspondence Address:
Yasuhiko Hayashi
Department of Neurosurgery, Kanazawa University, Kanazawa, Japan
DOI:10.4103/sni.sni_377_17
Copyright: © 2018 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Sho Tamai, Yasuhiko Hayashi, Yasuo Sasagawa, Masahiro Oishi, Mitsutoshi Nakada. A case of a mobile choroid plexus cyst presenting with different types of obstructive hydrocephalus. 23-Feb-2018;9:47
How to cite this URL: Sho Tamai, Yasuhiko Hayashi, Yasuo Sasagawa, Masahiro Oishi, Mitsutoshi Nakada. A case of a mobile choroid plexus cyst presenting with different types of obstructive hydrocephalus. 23-Feb-2018;9:47. Available from: http://surgicalneurologyint.com/surgicalint-articles/a-case-of-a-mobile-choroid-plexus-cyst-presenting-with-different-types-of-obstructive-hydrocephalus/
Date of Submission
06-Oct-2017
Date of Acceptance
19-Dec-2017
Date of Web Publication
23-Feb-2018
Abstract
Background:Although it is well known that most choroid plexus cysts (CPCs) are asymptomatic, previous studies have reported that they can infrequently cause progressive hydrocephalus along with their increasing sizes. Among those cases, some patients needed cyst fenestration or cerebrospinal fluid (CSF) diversion to recover neurological deterioration. Meanwhile, some CPCs revealed spontaneous resolution, and in rare cases, they developed re-accumulation. Some reports have described series of radiological findings about their changes in location.
Case Description:We present a 47-year-old male with CPC manifesting obstructive hydrocephalus. Radiological findings of the lateral and the third ventricles changed along with their different obstructive points, leading to their own symptoms. Because the patient's symptoms were not resolved completely, he underwent endoscopic fenestration for the cyst at the third ventricle. We could perform near-total resection, resulting in recovery of normal CSF flow. Postoperatively, the size of the ventricles decreased, with histological confirmation of a CPC. His symptoms resolved clearly without any complications.
Conclusions:It seems quite unusual that shift of the CPC location in the ventricle systems could induce not only different types of hydrocephalus but also their own symptoms. We need to consider that the location of CPCs might change when patients present with fluctuating symptoms over time.
Keywords: Choroid plexus cyst, endoscopic surgery, obstructive hydrocephalus
INTRODUCTION
Choroid plexus cysts (CPCs) rarely become symptomatic and are reported in 2.8% of fetal subjects upon second-trimester ultrasound examinations.[
CASE REPORT
A 47-year-old healthy man consulted a local hospital with complaints of unsteadiness and dizziness. Despite magnetic resonance imaging (MRI) revealing a cystic lesion in the third ventricle, he presented with no neurological abnormalities and his symptoms disappeared shortly. One year later, he was referred to the hospital again with complaints of headache. MRI revealed unilateral obstructive hydrocephalus with enlargement of the cyst, which occluded the foramen of Monro and protruded into the left lateral ventricle [

Figure 1
T2-weighted coronal magnetic resonance images. (a) The cystic lesion (black arrow) located in the third ventricle caused obstructive hydrocephalus with asymmetrical enlargement of the ventricles. (b) Preoperative image showing the asymmetrical enlargement of ventricles was resolved but the enlargement of ventricles remained because of previous protrusion of the cyst into the left lateral ventricle regressed into the third ventricle (white arrow). (c) Postoperative image revealing the ventricular size decreased
The patient underwent endoscopic cyst fenestration at the third ventricle via the left lateral ventricle with a fiberscope (VEF-V, Olympus, Japan). The cystic lesion occupied the enlarged foramen of Monro [
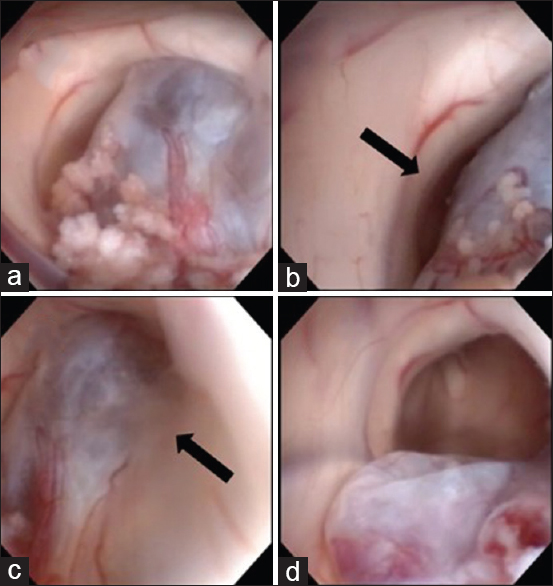
Figure 2
Operative findings. (a) The cyst arising from the third ventricle and protruding into the left foramen of Monro. (b) A slight gap between the cyst wall and the edge of the foramen of Monro (black arrow). (c) The cyst adhered to the choroid plexus at the edge of the foramen of Monro (black arrow). d) The cyst decreased in size after surgery, confirming the bottom of the third ventricle
Upon pathological examination of the surgical specimen, cuboidal epithelia lined with connective tissue were found in papillary patterns with some calcification and no malignant appearances [

The postoperative course was excellent, and his symptoms disappeared completely. MRI revealed the ventricles were reduced in size compared to preoperatively [
DISCUSSION
In the present report, we described a case of a previously healthy man who complained of fluctuating symptoms with a CPC at the third ventricle. The cyst changed its location and caused different types of obstructive hydrocephalus. Endoscopic surgery relieved his symptoms without any neurological deficits. This is the first case report that demonstrates a flexible CPC manifesting different types of obstructive hydrocephalus, as revealed on the chronological MRI findings.
CPCs are kinds of neuroepithelial cysts, usually located in the lateral ventricles, and rarely in the third ventricle.[
Flexible CPCs sometimes recur as symptomatic obstructive hydrocephalus. These cysts change their locations causing obstructive hydrocephalus along with the alternation of CSF pressure balance. In cerebral ultrasonography, some case reports described CPC in childhood showed that the CPC obstructed CSF pathways at the foramen of Monro while crying.[
The effectiveness of endoscopic surgery for intraventricular cysts has been reported by many authors.[
There are some differences in clinical symptoms between adults and children. Most cases of flexible CPCs in childhood have been reported to present as acute obstructive hydrocephalus.[
We experienced the first case of an adult patient who suffered from a flexible CPC inducing different types of obstructive hydrocephalus. These cysts in adults would sometimes develop as chronic obscure symptoms. We need to consider CPCs that are flexible when patients present with fluctuating symptoms as a possible operative indication.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Azab WA, Mijalcic RM, Aboalhasan AA, Khan TA, Abdelnabi EA. Endoscopic management of a choroid plexus cyst of the third ventricle: Case report and documentation of dynamic behavior. Childs Nerv Syst. 2015. 31: 815-9
2. Chamczuk AJ, Grand W. Endoscopic cauterization of a symptomatic choroid plexus cyst at the foramen of Monro: Case report. Neurosurgery. 2010. 66: 376-7
3. Filardi TZ, Finn L, Gabikian P, Giussani C, Ebenezer S, Avellino AM. Treatment of intermittent obstructive hydrocephalus secondary to a choroid plexus cyst. J Neurosurg Pediatr. 2009. 4: 571-4
4. Gangemi M, Maiuri F, Godano U, Mascari C, Longatti PL, Marzucco M. Endoscopic treatment of para- and intraventricular cerebrospinal fluid cysts. Minim Invasive Neurosurg. 2000. 43: 153-8
5. Hanbali F, Fuller GN, Leeds NE, Sawaya R. Choroid plexus cyst and chordoid glioma. Report of two cases. Neurosurg Focus. 2001. 10: E5-
6. Jeon JH, Lee SW, Ko JK, Choi BG, Cha SH, Song GS. Neuroendoscopic removal of large choroid plexus cyst: A case report. J Korean Med Sci. 2005. 20: 335-9
7. Morcos CL, Platt LD, Carlson DE, Gregory KD, Greene NH, Korst LM. The isolated choroid plexus cyst. Obstet Gynecol. 1998. 92: 232-6
8. Nahed BV, Darbar A, Doiron R, Saad A, Robson CD, Smith ER. Acute hydrocephalus secondary to obstruction of the foramen of Monro and cerebral aqueduct caused by a choroid plexus cyst in the lateral ventricle. Case report. J Neurosurg. 2007. 107: 236-9
9. Ormond DR, Omeis I, Mohan A, Murali R, Narayan P. Obstructive hydrocephalus due to a third ventricular neuroepithelial cyst. J Neurosurg Pediatr. 2008. 1: 481-4
10. Parizek J, Jakubec J, Hobza V, Nemeckova J, Cernoch Z, Sercl M. Choroid plexus cyst of the left lateral ventricle with intermittent blockage of the foramen of Monro, and initial invagination into the III ventricle in a child. Childs Nerv Syst. 1998. 14: 700-8
11. Spennato P, Chiaramonte C, Cicala D, Donofrio V, Barbarisi M, Nastro A. Acute triventricular hydrocephalus caused by choroid plexus cysts: A diagnostic and neurosurgical challenge. Neurosurg Focus. 2016. 41: E9-
12. van Baalen A, Stephani U. Flexible and floating choroid plexus cyst of the third ventricle: An ultrasonographic video documentation. Child Nerv Syst. 2007. 23: 259-61

