

- Department of Neurosurgery, Keio University School of Medicine, Shinjuku, Tokyo, Japan
- Department of Pathology, Keio University School of Medicine, Shinjuku, Tokyo, Japan
Correspondence Address:
Kenzo Kosugi
Department of Neurosurgery, Keio University School of Medicine, Shinjuku, Tokyo, Japan
DOI:10.4103/2152-7806.200582
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Kenzo Kosugi, Satoshi Takahashi, Hikaru Sasaki, Ryota Tamura, Kentaro Ohara, Kazunari Yoshida. A case of acute subdural hematoma due to bleeding from metastatic chondrosarcoma of the skull. 20-Feb-2017;8:23
How to cite this URL: Kenzo Kosugi, Satoshi Takahashi, Hikaru Sasaki, Ryota Tamura, Kentaro Ohara, Kazunari Yoshida. A case of acute subdural hematoma due to bleeding from metastatic chondrosarcoma of the skull. 20-Feb-2017;8:23. Available from: http://surgicalneurologyint.com/surgicalint_articles/a-case-of-acute-subdural-hematoma-due-to-bleeding-from-metastatic-chondrosarcoma-of-the-skull/
Date of Submission
31-Oct-2016
Date of Acceptance
15-Dec-2016
Date of Web Publication
20-Feb-2017
Abstract
Background:Intra or peritumoral hemorrhage of brain and skull tumors sometimes presents as stroke. Skull metastasis of chondrosarcoma is relatively rare, and furthermore, a case of intratumoural hemorrhage of skull metastasis of chondrosarcoma has not been reported.
Case Description:A 73-year-old man underwent right lower leg amputation in the past because of chondrosarcoma and was operated for a skull metastasis. He presented with a sudden headache, and head computed tomography revealed a right acute subdural hematoma (SDH) adjacent to the recurrent skull metastatic tumor. The removal of the SDH and tumor resection were performed emergently. The intraoperative findings included metastatic invasion beyond the dura mater to as deep as the subdural space, and the histological diagnosis was metastatic chondrosarcoma. His postoperative course was uneventful.
Conclusion:In the event of subdural invasion of a metastatic lesion, intratumoral hemorrhage may induce acute SDH, as in the present case. Similar to our case, most previous reports of intracranial chondrosarcoma hemorrhage have had an unclear etiology. Despite the rarity of this event, a patient with a history of malignancy presenting with nontraumatic acute SDH should be examined for the intratumoral hemorrhage of skull metastasis in the differential diagnosis.
Keywords: Acute subdural hematoma, chondrosarcoma, intratumoral hemorrhage, skull metastasis
INTRODUCTION
Cases of skull metastases of chondrosarcoma and of subdural hematomas (SDHs) caused by the intratumoral hemorrhage of skull metastases of malignant tumors are relatively rare. Because intracerebral hemorrhage in meningioma is also rare, with a frequency of 1.3%,[
CASE DESCRIPTION
A 73-year-old man underwent right lower leg amputation 16 years earlier because of chondrosarcoma. He previously had surgeries for lung and liver metastases of the lesion. One year ago, he underwent extended resection and subsequent cranioplasty for a skull metastasis. Because of the recurrence of the skull metastasis, another surgical resection was planned [
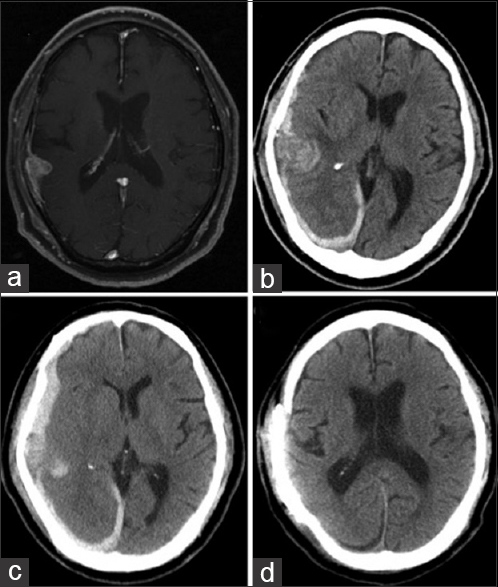
Figure 1
(a) A gadolinium-enhanced T1-weighted magnetic resonance (Gd-T1WI MR) image taken before scheduled surgery revealed the contrasted mass lesion on the left calvarium adjacent to normal brain with subdural invasion. (b) Head computed tomography (CT) taken on the day of admission revealed right-sided acute subdural hematoma (SDH). (c) Head CT performed before the urgent surgery revealed acute SDH with midline shift that indicated intratumoral hemorrhage of the calvarial metastasis. (d) Postoperative head CT showed the resected calvarial tumor and improvement of the midline shift
DISCUSSION
According to the brain tumor registry of Japan, the frequency of malignant calvarial metastasis is approximately 2% among the 14000 recorded metastatic brain tumors.[
To date, there have been 6 reported cases of primary intracranial chondrosarcoma presenting with cranial hemorrhage.[
Here, we report the first case of the calvarial metastasis of chondrosarcoma presenting with acute subdural hematoma. Despite the rarity of this event, a patient with a history of malignancy presenting with nontraumatic acute SDH should be examined for the intratumoral hemorrhage of skull metastasis in the differential diagnosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Fukuchi M, Fushimi S, Yoneya M, Hirayama A, Mineura K, Kowada M. Chondrosarcoma of the skull base associated with fatal intratumoral hemorrhage: Report of an autopsy case and review of the literature. No Shinkei Geka. 1996. 24: 175-80
2. Gallia GL, Binder ZA, Schwarz J, Moriarity JL, Weingart JD. Skull base chondrosarcoma presenting with hemorrhage. Can J Neurol Sci. 2009. 36: 774-5
3. Harada K, Nakahara I, Hayashi J, Tanaka M, Akiyama Y, Iwamuro Y. Chondrosarcoma of the clivus presenting with intratumoral hemorrhage: Case report. J Neurooncol. 2006. 77: 221-3
4. Jumani MI, Channa R, Zafar SN, Enam SA. Pontine haemorrhage due to chondrosarcoma of the skull base. J Coll Physicians Surg Pak. 2010. 20: 692-4
5. Karlawish JH, Smith GW, Gabrielson EW, Liu MC. Spontaneous hemothorax caused by a chest wall chondrosarcoma. Ann Thorac Surg. 1995. 59: 231-3
6. Kawano T, Hamada J, Morioka M, Mihara Y, Ishimaru Y, Kaku M. Skull metastasis from clear cell chondrosarcoma, case report. Neurol Med Chir. 2005. 45: 367-70
7. Kumar PM, Manisha M. Epidural hematoma secondary to solitary skull metastasis from an ovarian cancer. Asian J Neurosurg. 2014. 9: 112-4
8. Kuzeyli K, Cakir E, Usul H, Karaarslan G, Yazar U, Baykal S. Intratumoral haemorrhage: A clinical study. J Clin Neurosci. 2004. 11: 490-2
9. Lagergren C, Lindbom A, Soderberg G. The blood vessels of chondrosarcoma. Acta radiol. 1961. 55: 321-8
10. Little A, Chung C, Perez-Ordonez B, Mikulis D, Valiante TA. High-grade intracranial chondrosarcoma presenting with haemorrhage. J Clin Neurosci. 2013. 20: 1457-60
11. Ohshige H, Kasai H, Imahori T, Ryu T, Azuma K, Yoshimura K. A case of petrous bone myxoid chondrosarcoma associated with cerebellar hemorrhage. Brain Tumor Pathol. 2005. 22: 41-4
12. . Report of brain tumor registry of japan (1984-2000) 12th edition. Neurol Med Chir. 2009. 49: 22-5
13. Shibao S, Kimura T, Sasaki H, Fujiwara H, Akiyama T, Ueno M. Hemorrhagic onset of cerebellar pilocytic astrocytoma in an adult: A case report and review of the literature implying a possible relation of degenerative vascular changes to the massive intratumoral hemorrhage. Brain Tumor Pathol. 2012. 29: 96-102

