

- Department of Neurosurgery, National Institute of Neurology Tunis, Tunisia Faculty of Medicine, University of Tunis el MANAR, Tunisia
- Department of Histopathology, la Rabta, Faculty of Medicine, University of Tunis El Manar, Tunis, Tunisia
- Department of Neuroradiology, National Institute of Neurology Tunis, Tunisia Faculty of Medicine, University of Tunis el MANAR, Tunisia
Correspondence Address:
Sofiene Bouali
Department of Neurosurgery, National Institute of Neurology Tunis, Tunisia Faculty of Medicine, University of Tunis el MANAR, Tunisia
DOI:10.4103/sni.sni_295_17
Copyright: © 2018 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Sofiene Bouali, Nidhal Maatar, Alia Zehani, Maha Mahmoud, Jalel Kallel, Hafedh Jemel. A case of adult anaplastic cerebellar ganglioglioma. 14-Feb-2018;9:31
How to cite this URL: Sofiene Bouali, Nidhal Maatar, Alia Zehani, Maha Mahmoud, Jalel Kallel, Hafedh Jemel. A case of adult anaplastic cerebellar ganglioglioma. 14-Feb-2018;9:31. Available from: http://surgicalneurologyint.com/surgicalint-articles/a-case-of-adult-anaplastic-cerebellar-ganglioglioma/
Date of Submission
18-Aug-2017
Date of Acceptance
20-Dec-2017
Date of Web Publication
14-Feb-2018
Abstract
Background:Anaplastic posterior fossa ganglioglioma in adults is exceedingly rare. To date, only one case of adult anaplastic posterior fossa ganglioglioma has been reported in the English literature and none has been described at the cerebellum. To our knowledge, this report is the third case of malignant posterior fossa ganglioglioma in adults and the first at the cerebellum. In general, this entity can be misdiagnosed preoperatively as a primary posterior fossa neoplasm, and by reporting our clinical and radiographic observations we want to add to the existing literature on this rare entity.
Case Description:A 40-year-old man presented with a history of headaches and dizziness and progressive gait disturbance and was diagnosed with anaplastic ganglioglioma in the posterior fossa.
Conclusions:Although rare, our case demonstrates that anaplastic ganglioglioma should be considered in the differential diagnosis of infratentorial tumors in adult patients.
Keywords: Anaplastic ganglioglioma, cerebellum, posterior cranial fossa, prognosis
INTRODUCTION
Anaplastic ganglioglioma is a very infrequent primary neoplasm of the central nervous system. These tumors are most commonly found in the supratentorial compartment, and any occurrence in the posterior fossa is considered a rare event.[
To date, only few cases of malignant infratentorial gangliogliomas have been documented, and commonly among children.[
Here, we report an adult patient with anaplastic ganglioglioma of the cerebellum; the first such reported case in the literature. We also review the literature related to infratentorial malignant gangliogliomas, and discuss the clinical manifestations, imaging and histopathological findings, reported treatments, and the outcome associated with such lesions.
CASE REPORT
A comprehensive literature search for this review was conducted on PubMEd, MedLine, and Google Scholar. There were no limitations on the date, type, or language of the publication. The first search was conducted using the term “posterior fossa ganglioglioma” followed by “posterior fossa anaplastic ganglioglioma,” “cerebellar anaplastic ganglioglioma,” and “posterior fossa ganglioblastoma.”
The titles and abstracts were reviewed and only11 publications were selected relating to malignant posterior fossa ganglioglioma; 3 in adults and 8 in children. These cases are reviewed in
CASE DESCRIPTION
A 40-year-old man presented to the neurosurgical department with a history of headache for 3 months. His headache was associated with a progressive staggering gait, dizziness, and nausea. Past and family history was unremarkable.
General physical examination and review of systems were not contributory. Routine blood tests were normal, and chest X-ray was normal. The patient was HIV-negative. Neurological examination showed focal cerebellar signs, including ipsilateral cerebellar ataxia, and slurred speech. The fundus oculi were normal bilaterally.
Cranial magnetic resonance imaging (MRI) revealed a solid mass with a maximum diameter of 3 cm, which appeared hypointense on T1-weighted sequences and hyperintense on T2-weighted images. The lesion enhanced irregularly after the administration of intravenous gadolinium. MR spectroscopy was obtained and showed a high choline/creatine ratio with increased myoinositol level, suggesting anaplastic behavior of the lesion [
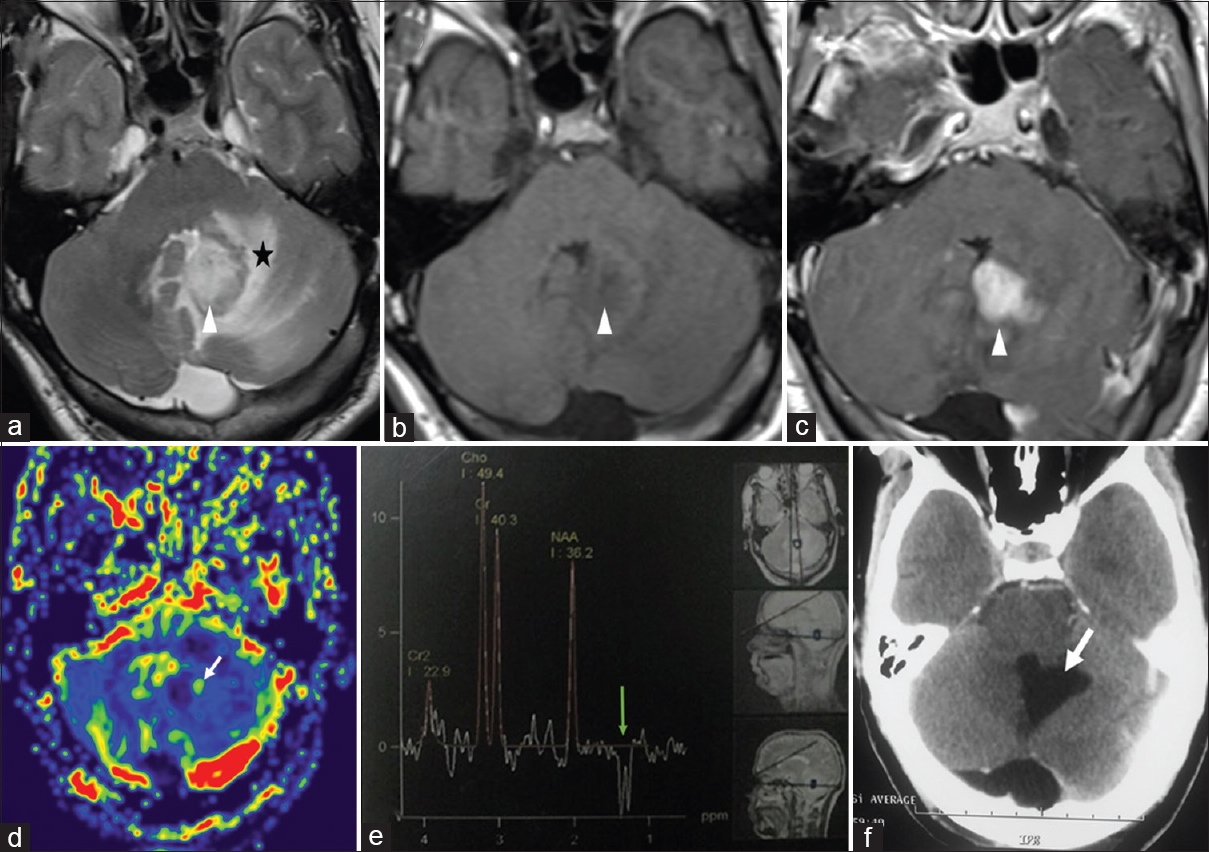
Figure 1
Preoperative magnetic resonance imaging (MRI). T2 (a), T1 native (b), and T1 after gadolinium administration (c): left cerebellar lesion (arrowhead) slightly hypointense on T1-weighted images and hyperintense on T2-weighted images, with peritumoral edema (black star) and strong ill-defined contrast enhancement. (d) MR perfusion with cerebral blood volume (CBV) cartography: slight peripheral hyperperfusion (white arrow); rCBV = 1.9 × normal contralateral cerebellum white matter. (e) Proton MR spectroscopy: elevated doublet of lactate at 1.33 ppm which is inverted on the spectrum with long echo-time (green arrow). NAA/Creatine ratio is reduced (f) Postoperative CT scan: resection cavity (white arrow)
Under a working diagnosis of a neoplastic process, a standard suboccipital craniotomy was performed in the prone position. After opening the dura mater and performing a corticectomy for access and after transvermian approach, the lesion was found to be infiltrative and hypervascular. Complete tumor resection was performed, as shown in the postoperative CT scan. The postoperative course was uneventful. The histological diagnosis of the lesion yielded an anaplastic ganglioglioma, with the tumor showing biphasic pattern of ganglion cells and neoplastic glial cells. The malignant glial component characterized by hypercellularity, nuclear atypia, and increased mitotic activity; however, no microvascular proliferation or necrosis was present [

Figure 2
(A): (Hematoxylin eosin ×20): tumor showing biphasic pattern of ganglion cells and neoplastic glial cells. (b): (Hematoxylin eosin ×20): malignant glial component characterized by hypercellularity, nuclear atypia and increased mitotic activity. (B) Immunohistochemistry ×400. (c) GFAP: the neoplastic glial cells are immunoreactive for GFAP. (d) Ki67: Ki67 proliferation index was 20%. (e) Synaptophysin: the neoplastic ganglion cells are immunoreactive for synaptophysin
The patient received standard fractionated radiotherapy at a total dose of 54 Gy (1.8 Gy per day, 5 days a week) for 6 weeks. Follow-up of the patient with a computed tomography (CT) scan for 6 months after the surgery did not show any evidence of tumor recurrence [
Despite two cycles of adjuvant temozolomide, the tumor recurred and progressed with cerebellar multiple nodular location and died 10 months after the surgery.
Only 3 cases of malignant posterior fossa ganglioglioma in adults have been reported in the English literature (A summary of patient characteristics at presentation and surgical outcome is presented in
DISCUSSION
Gangliogliomas are rare mixed glioneuronal tumors that represent less than 1% of central nerve system neoplasms[
Gangliogliomas are staged according to the most recent WHO classification[
While the exact etiology and pathogenesis remains unclear, the cell of origin is thought to be a glioneuronal precursor.[
To be considered an anaplastic ganglioglioma, the tumor had to have five or more mitoses per 10 high-power fields, and at least one of the additional criteria, angiogenesis and/or necrosis, in the glial component.[
Anaplastic ganglioglioma can arise de novo or secondary via malignant transformation of a pre-existing WHO grade I ganglioglioma. The rate of intracranial gangliogliomas malignant transformation has been calculated to range from 0.6 to 14.5%.[
Only 11 infratentorial anaplastic ganglioglioma cases have been reported in the literature that are preferentially diagnosed in children with a slight preponderance among males.[
There have been no previous reports describing an anaplastic ganglioglioma (grade III) located in the parenchyma of the cerebellum.
Our review of the literature describing gangliogliomas of the posterior fossa has yielded that these tumors can manifest similar to other lesions in this location with hydrocephalus, cranial nerve palsies, gait and speech disorders, and even myoclonus.[
The median history of disease reported by Karremann et al. was 9 months (range, 1.0–43.0 months) and depended on the location and size of the tumor.[
In a majority of the series and reported cases, the characteristics described on MRI were hypointensity in T1, hyperintensity on T2 and FLAIR, and patchy enhancement after contrast administration. The apparent diffusion coefficient value of anaplastic ganglioglioma was reported to be reduced (0.95 × 10-3 mm2/s (SD = 0.053), which likely reflects its high cellularity. In gangliogliomas with anaplastic features, MR spectroscopy has been previously shown do demonstrate peaks of glutamate, choline, and myoinositol.[
Due to their low frequency, a standard treatment for anaplastic ganglioglioma has not been established yet. According to the literature, complete surgical resection is recommended.[
Following resection, radiotherapy seems to improve local control rates in high-grade gangliogliomas and should be applied as an adjuvant therapy. Standard fractionated radiotherapy (54.0–59.4 Gy total dose; doses of 1.8 Gy/day, 5 days/week over 6–7 weeks) was common for most cases.[
The role of systemic chemotherapy has not been established in prospective randomized trials due to low number of cases seen, and previously employed regimen are not well documented in the existing case series. Prognostic factors of poor survival are older age at diagnosis, male sex, and malignant glial features.[
Anaplastic gangliogliomas appear to represent a very aggressive disease with poor overall outcome (median progression-free survival, 10 months; median overall survival; 27 months).[
Varlet et al. have shown that the extent of surgical resection in malignant glioneuronal tumors is significantly correlated to survival.[
In a recent study, immunohistochemical molecular analyses indicated that BRAF V600E mutation is present in 39% of anaplastic gangliogliomas in both glial and neuronal population without prognostic significance.[
Personalized therapies as anti-BRAF inhibitors can be a useful adjuvant therapy together with the first-line oncological treatments, and a few cases of anaplastic gangliogliomas treated by anti-BRAF therapy with promising results have been reported.[
CONCLUSION
We present a rare case of anaplastic ganglioglioma WHO III in the cerebellum of an adult patient along with its clinical diagnosis and treatment. This is only one of a few such cases observed thus far and contributes to our understanding of the characteristics of this rare posterior fossa tumor. The present work demonstrates that anaplastic ganglioglioma need to be considered in the differential diagnosis of malignant primary infratentorial brain tumors in adult patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bautista F, Paci A, Minard-Colin V, Dufour C, Grill J, Lacroix L. Vemurafenib in pediatric patients with BRAFV600E mutated high-grade gliomas. Pediatr Blood Cancer. 2014. 61: 1101-3
2. Dahiya S, Haydon DH, Alvarado D, Gurnett CA, Gutmann DH, Leonard JR. BRAFV600E mutation is a negative prognosticator in pediatric ganglioglioma. Acta Neuropathol. 2013. 125: 901-10
3. De Souza RB, de Aguiar GB, Araújo JLV, Mayrink D, dos Santos ARL. Posterior fossa ganglioglioma: An unusual neoplasm in a rare location. Austin Neurosurg Open Access. 2014. 1: 1010-
4. Erguvan-önal R, Önal Ç, Aydin NE. Anaplastic Ganglioglioma: Is it a Sign of Better Prognosis?. J Nervous Sys Surg. 2009. 2: 72-8
5. Gelabert-González M, Amo JM, Arcos Algaba A, Serramito García R, Castro Bouzas D, Díaz Cabana L. Gangliogliomas intracraneales. Revisión de una serie de 20 pacientes. Neurología. 2011. 26: 405-15
6. González Toledo E, Nader M, Thomas-Ogunniyi J, Wilson J. Anaplastic Ganglioglioma of the Brainstem in an Adult. Neuroradiol J. 2012. 25: 325-9
7. Hirose T, Kannuki S, Nishida K, Matsumoto K, Sano T, Hizawa K. Anaplastic ganglioglioma of the brain stem demonstrating active neurosecretory features of neoplastic neuronal cells. Acta Neuropathol. 1992. 83: 365-70
8. Jay V, Squire J, Becker LE, Humphreys R. Malignant transformation in a ganglioglioma with anaplastic neuronal and astrocytic components. Report of a case with flow cytometric and cytogenetic analysis. Cancer. 1994. 73: 2862-8
9. Jay V, Squire J, Blaser S, Hoffman HJ, Hwang P. Intracranial and spinal metastases from a ganglioglioma with unusual cytogenetic abnormalities in a patient with complex partial seizures. Childs Nerv Syst. 1997. 13: 550-5
10. Karremann M, Pietsch T, Janssen G, Kramm CM, Wolff JE. Anaplastic ganglioglioma in children. J Neurooncol. 2009. 92: 157-63
11. Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016. 131: 803-20
12. Lucas JT, Huang AJ, Mott RT, Lesser GJ, Tatter SB, Chan MD. Anaplastic ganglioglioma: A report of three cases and review of the literature. J Neurooncol. 2015. 123: 171-7
13. Lüdemann W, Banan R, Hartmann C, Bertalanffy H, Di Rocco C. Pediatric intracranial primary anaplastic ganglioglioma. Childs Nerv Syst. 2017. 33: 227-31
14. Luyken C, Blumcke I, Fimmers R, Urbach H, Wiestler OD, Schramm J. Supratentorial gangliogliomas: histopathologic grading and tumor recurrence in 184 patients with a median follow-up of 8 years. Cancer. 2004. 101: 146-55
15. Majores M, von Lehe M, Fassunke J, Schramm J, Becker AJ, Simon M. Tumor recurrence and malignant progression of gangliogliomas. Cancer. 2008. 113: 3355-63
16. Matzusaki M, Uno M, Kageji T. Anaplastic ganglioglioma of the cerebellopontine angle. Neurol Med Chir (Tokyo). 2005. 45: 591-5
17. Mekni A, Chelly I, Haouet S, Zitouna M, Kchir N. Malignant cerebellar ganglioglioma. A case report and review of the literature. Neurochirurgie. 2006. 52: 119-22
18. Prabowo AS, Iyer AM, Veersema TJ, Anink JJ, Schouten-van Meeteren AY, Spliet WG. BRAF V600E mutation is associated with mTOR signaling activation in glioneuronal tumors. Brain Pathol. 2014. 24: 52-66
19. Selvanathan SK, Hammouche S, Salminen HJ, Jenkinson MD. Outcome and prognostic features in anaplastic ganglioglioma: Analysis of cases from the SEER database. J Neurooncol. 2011. 105: 539-45
20. Shah MJ, Sircar R, Linder-Luch M, Böhm J, van Velthoven-Wurster V. Anaplastic Posterior Fossa Ganglioglioma in a Child: Case Report and Short Review of the Literature. J Neurol Surg A. 2012. 73: 46-9
21. Siddique K, Zagardo M, Gujrati M, Olivero W. Ganglioglioma presenting as a meningioma: Case report and review of the literature. Neurosurgery. 2002. 50: 1133-5
22. Takei H, Dauser R, Su J, Chintagumpala M, Bhattacharjee MB, Jones J. Anaplastic ganglioglioma arising from a Lhermitte-Duclos-like lesion. Case report. J Neurosurg. 2007. 107: 137-42
23. Terrier LM, Bauchet L, Rigau V, Amelot A, Zouaoui S, Filipiak I. Natural course and prognosis of anaplastic gangliogliomas: A multicenter retrospective study of 43 cases from the French Brain Tumor Database. Neuro Oncol. 2016. 30: 186-
24. Varlet P, Soni D, Miquel C, Roux FX, Meder JF, Chneiweiss H, Daumas-Duport C. New variants of malignant glioneuronal tumors: A clinicopathological study of 40 cases. Neurosurgery. 2004. 55: 1377-91
25. Yust-Katz S, Anderson MD, Liu D, Wu J, Yuan Y, Olar A. Clinical and prognostic features of adult patients with gangliogliomas. Neuro-Oncol. 2014. 16: 409-13
26. Zanello M, Pages M, Tauziède-Espariat A, Saffroy R, Puget S, Lacroix L, Dezamis E. Clinical, Imaging, Histopathological and Molecular Characterization of Anaplastic Ganglioglioma. J Neuropathol Exp Neurol. 2016. 75: 971-80

