

- Department of Neurosurgery, Ashikaga Red Cross Hospital, Ashikaga-shi, Tochigi, Japan
Correspondence Address:
Hideyuki Tomita
Department of Neurosurgery, Ashikaga Red Cross Hospital, Ashikaga-shi, Tochigi, Japan
DOI:10.4103/sni.sni_4_18
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Hideyuki Tomita, Katsuya Saito. A difficult-to-treat Acom aneurysm with the combined vascular anomaly of Acom fenestration and accessory anterior cerebral artery. 21-Mar-2018;9:67
How to cite this URL: Hideyuki Tomita, Katsuya Saito. A difficult-to-treat Acom aneurysm with the combined vascular anomaly of Acom fenestration and accessory anterior cerebral artery. 21-Mar-2018;9:67. Available from: http://surgicalneurologyint.com/surgicalint-articles/a-difficult%e2%80%91to%e2%80%91treat-acom-aneurysm-with-the-combined-vascular-anomaly-of-acom-fenestration-and-accessory-anterior-cerebral-artery/
Date of Submission
05-Jan-2018
Date of Acceptance
15-Jan-2018
Date of Web Publication
21-Mar-2018
Abstract
Background:Vascular anomaly and aneurysmal formation of an anterior communicating artery (Acom) complex has often been reported. Because of such a complicated relationship between the vascular structure and aneurysms, Acom aneurysm is one of the most difficult aneurysms to treat among other common anterior circulation aneurysms. We experienced an extremely rare and difficult-to-treat case of ruptured Acom aneurysm with the combined vascular anomaly of the Acom fenestration and an accessory anterior cerebral artery (ACA).
Case Description:A 29-year-old man underwent a clipping surgery for a ruptured Acom aneurysm with an Acom fenestration and an accessory ACA. By reasons of the complicated Acom structure and a posteriorly-projecting aneurysm, the patient was operated via an interhemispheric approach, which is generally reported to provide the best operative view for all types of Acom aneurysms. However, we could not help applying a clip in the narrow working space and the limited operative view, due to the poor mobilization of Acom complex and the interruption by an accessory ACA.
Conclusion:The interhemispheric approach may exceptionally have a blind area behind the Acom complex in the case of Acom aneurysms with an accessory ACA. Additionally, the aneurysms arising from the Acom fenestration strongly require neurosurgeons to take a more accurate surgical approach to obtain a direct visualization for an aneurysmal neck.
Keywords: Acom fenestration, accessory anterior cerebral artery, interhemispheric approach, pterional approach, subarachnoid hemorrhage
INTRODUCTION
Vascular anomaly of the anterior communicating artery (Acom) complex and anterior cerebral artery (ACA) relates closely with the cerebral aneurysm formation.[
CASE DESCRIPTION
A 29-year-old man was taken to our hospital by ambulance, suffering from severe headache. He had no past medical history and did not take any medication. Head computed tomography (CT) revealed an extensive subarachnoid hemorrhage (SAH) filling basal cisterns, especially the thick hemorrhage in the interhemispheric fissure [
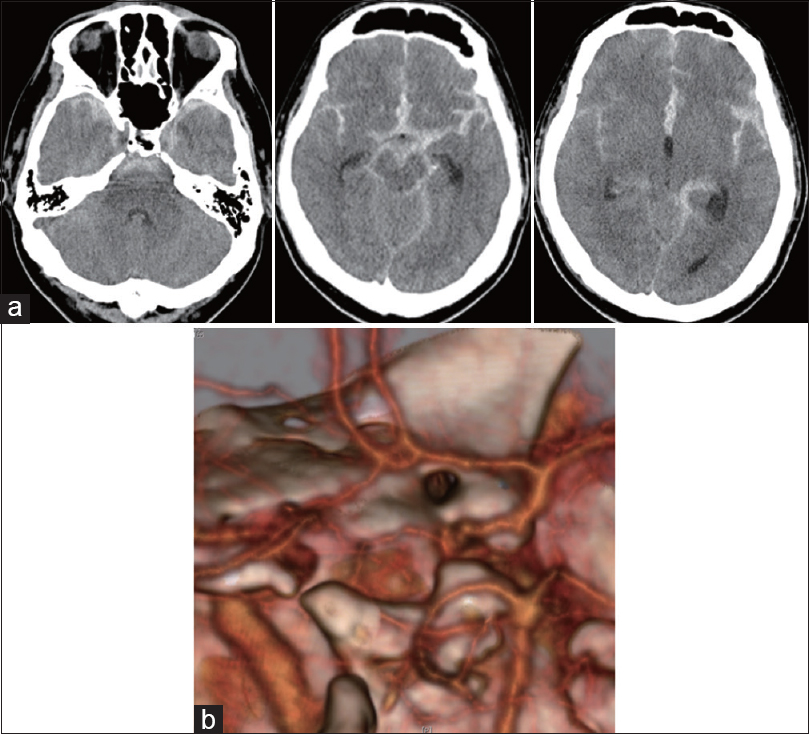
Figure 1
(a) Head computed tomography (CT) on admission. Diffuse subarachnoid hemorrhage in the basal cistern. In particular, a thick subarachnoid hemorrhage in the proximal portion of interhemispheric fissure. (b) Three-dimensional-CT Angiography (3D-CTA) on admission. 3D-CTA showed the anterior communicating artery (Acom) fenestration, but no evidence of aneurysm. The quality of this study was poor, probably due to high intracranial pressure
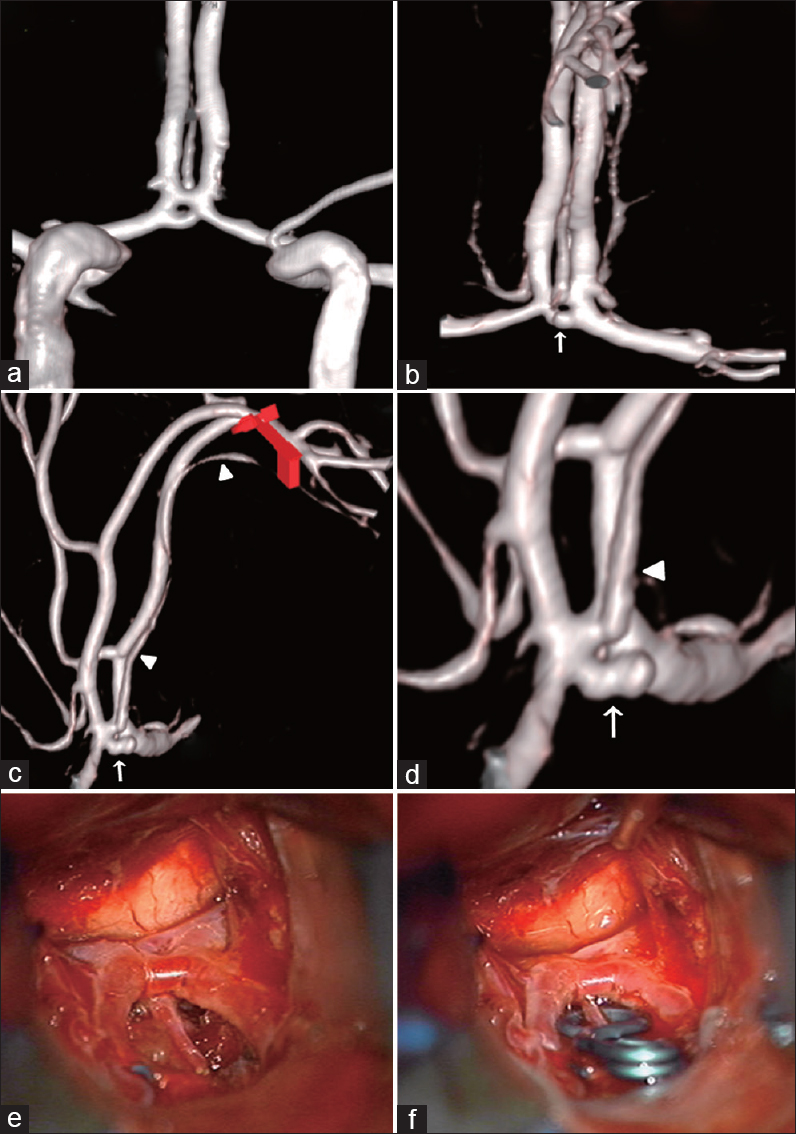
Figure 2
(a-d) Three-dimensional-digital subtraction angiography (3D-DSA) on admission. (a) water's view, (b) A-P view, (c) L-R view, (d) magnification picture of c. 3D-DSA revealed the vascular anomaly [the anterior communicating artery (Acom) fenestration and an accessory anterior cerebral artery] and small Acom aneurysm projecting posteriorly. An accessory anterior cerebral artery (arrow head) arose from the upper limb of the fenestrated segment. In contrast, the Acom aneurysm (arrow) arose from the inferior limb of the fenestrated segment. (e-f) Intraoperative photographs. The surgical view obtained from the interhemispheric approach showed a blind area behind the Acom complex with limited mobilization. A fenestrated clip was applied to be able to preserve an accessory anterior cerebral artery
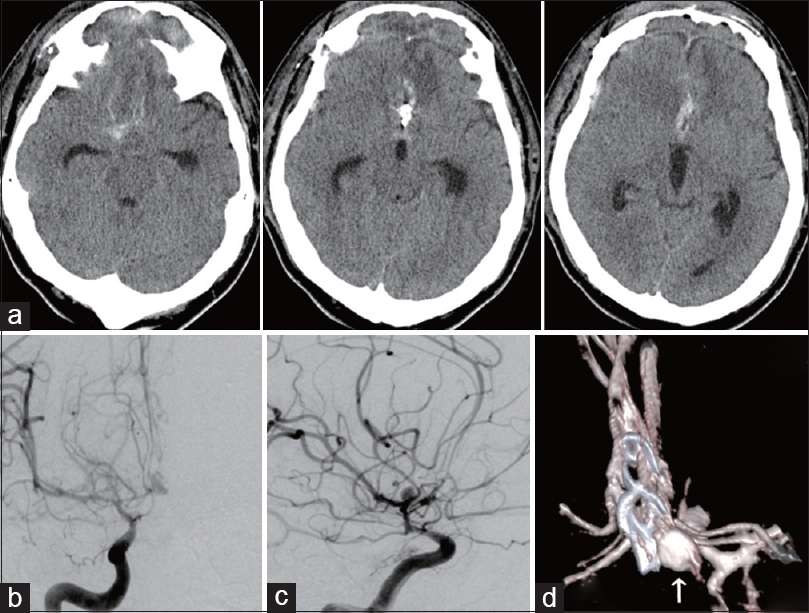
Figure 3
(a) Head computed tomography (CT) on Day 13. The focal subarachnoid hemorrhage was observed around the aneurysmal clip, suggesting the re-rupture from the remnant of anterior communicating artery (Acom) aneurysm. (b-c) Two-dimensional-digital subtraction angiography (2D-DSA) after re-rupture. b: P-A view, c: R-L view. 2D-DSA showed the recurrence of Acom aneurysm. (d) Three-dimensional-digital subtraction angiography (3D-DSA) after re-rupture, posterior view with caudal angulation. The recurrence of an aneurysm (arrow) was observed next to the clip
DISCUSSION
Vascular anomalies of the circle of Willis frequently associated with the aneurysm, and several anomalies of the Acom complex and ACA have been described.[
The pterional approach and interhemispheric approach are standard surgical procedures for clipping Acom aneurysms.[
CONCLUSION
Vascular anomaly associated with Acom complex is often observed. The aneurysms of fenestrated Acom should be approached to be able to obtain a direct visualization for an aneurysmal neck, because the Acom complex may be fixed and poorly mobilized. In addition, an interhemispheric approach may exceptionally have a blind area behind the Acom complex in the case of Acom aneurysms with an accessory ACA, although an interhemispheric approach is generally reported to provide the best operative view for all types of Acom aneurysms.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Agrawal A, Kato Y, Chen L, Karagiozov K, Yoneda M, Imizu S. Anterior communicating artery aneurysms: An overview. Minim Invasive Neurosurg. 2008. 51: 131-5
2. Chen L, Agrawal A, Kato Y, Karagiozov KL, Kumar MV, Sano H. Role of aneurysm projection in “A2” fork orientation for determining the side of surgical approach. Acta Neurochir. 2009. 151: 925-33; discussion 933
3. de Gast AN, van Rooij WJ, Sluzewski M. Fenestrations of the anterior communicating artery: Incidence on 3D angiography and relationship to aneurysms. AJNR Am J Neuroradiol. 2008. 29: 296-8
4. Dehdashti AR, Chiluwal AK, Regli L. The Implication of Anterior Communicating Complex Rotation and 3-Dimensional Computerized Tomography Angiography Findings in Surgical Approach to Anterior Communicating Artery Aneurysms. World Neurosurg. 2016. 91: 34-42
5. Dimmick SJ, Faulder KC. Normal variants of the cerebral circulation at multidetector CT angiography. Radiographics. 2009. 29: 1027-43
6. El-Noamany H, Nakagawa F, Hongo K, Kakizawa Y, Kobayashi S. Low anterior interhemispheric approach--a narrow corridor to aneurysms of the anterior communicating artery. Acta Neurochir. 2001. 143: 885-91
7. Inui T, Okuno S, Nakase H, Uranishi R, Hashimoto H, Fujimoto K. [Relationship of Distal Anterior Cerebral Artery Aneurysm Arising from the Supracallosal Portion and Accessory Anterior Cerebral Artery]. No Shinkei Geka. 2016. 44: 103-8
8. Katsuhiko A, Yoko K, Hirotoshi S, Kazuhiro K, Yuko O, Hajime T. Surgical Treatment for Anterior Communicating Artery Aneurysm with Fenestration. Surg Cereb Stroke. 1997. 25: 114-8
9. Kiyofuji S, Inoue T, Tamura A, Saito I. Combined interhemispheric and pterional approach for ACOM and left MCA aneurysms. Neurosurg Focus. 2015. 38: Video15-
10. Kutsuna M, Monden S, Watanabe K. [Two cases of distal anterior cerebral artery aneurysm associated with accessory anterior cerebral artery]. No Shinkei Geka. 2006. 34: 193-200
11. Kwak R, Niizuma H, Hatanaka M, Suzuki J. Anterior communicating artery aneurysms with associated anomalies. J Neurosurg. 1980. 52: 162-4
12. Maeda K, Tanaka S, Hatae R, Maeda Y, Miyazono M. [Two cases of anterior cerebral artery aneurysm associated with accessory anterior cerebral artery: Review of the literature and points of diagnosis]. No Shinkei Geka. 2014. 42: 461-6
13. Makowicz G, Poniatowska R, Lusawa M. Variants of cerebral arteries - anterior circulation. Polish J Radiol. 2013. 78: 42-7
14. Niederberger E, Gauvrit JY, Morandi X, Carsin-Nicol B, Gauthier T, Ferre JC. Anatomic variants of the anterior part of the cerebral arterial circle at multidetector computed tomography angiography. J Neuroradiol. 2010. 37: 139-47
15. Ogawa A, Suzuki M, Sakurai Y, Yoshimoto T. Vascular anomalies associated with aneurysms of the anterior communicating artery: Microsurgical observations. J Neurosurg. 1990. 72: 706-9
16. Sano H. [Surgical approach for aneurysm of the anterior communicating artery]. No Shinkei Geka. 2000. 28: 9-16
17. Suzuki M, Ogawa A, Kayama T, Sakurai Y, Suzuki J. [Vascular anomalies associated with anterior communicating aneurysms]. No Shinkei Geka. 1988. 16(5 Suppl): 498-502
18. van Rooij SB, Bechan RS, Peluso JP, Sluzewski M, van Rooij WJ. Fenestrations of intracranial arteries. AJNR Am J Neuroradiol. 2015. 36: 1167-70
Commentary
C. David Hunt- Hoboken, NJ 07030
huntneurosurgery@mac.com
The authors courageously report the persistence (not recurrence) of an aneurysm of a complex anterior communicating complex following an inter hemispheric approach.
Their chosen operative approach, one of a number of described approaches, was particularly ineffective in this complex configuration.
I would point out that proximal control, enabling a safer and more thorough evaluation of complex configurations, is also a surgical goal. For this reason, a pterional approach from the dominant ACA side, is a preferred approach in this surgeon's experience.

