

- Department of Neurological and Sensory Sciences, Division of Neurosurgery, Siena University Hospital, Siena, Italy
- Department of Medicine, Surgery, and Neurosciences, Section of Neurosurgery, University of Siena, Siena, Italy
- Department of Medicine, Surgery, and Neurosciences, Section of Human Pathology, University of Siena, Siena, Italy
Correspondence Address:
Vitaliano F. Muzii
Department of Medicine, Surgery, and Neurosciences, Section of Neurosurgery, University of Siena, Siena, Italy
DOI:10.4103/2152-7806.207115
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Biagio R. Carangelo, Giovanni Muscas, Clelia Miracco, Vitaliano F. Muzii. A rare association of ganglioglioma and cavernous malformation: Report of two cases and literature review. 26-May-2017;8:94
How to cite this URL: Biagio R. Carangelo, Giovanni Muscas, Clelia Miracco, Vitaliano F. Muzii. A rare association of ganglioglioma and cavernous malformation: Report of two cases and literature review. 26-May-2017;8:94. Available from: http://surgicalneurologyint.com/surgicalint-articles/a-rare-association-of-ganglioglioma-and-cavernous-malformation-report-of-two-cases-and-literature-review/
Date of Submission
12-Sep-2016
Date of Acceptance
13-Dec-2016
Date of Web Publication
26-May-2017
Abstract
Background:Some glial tumors have been observed in association with different types of vascular malformations of the brain (angiogliomas). However, the association of ganglioglioma with other vascular malformations is extremely rare, with only few cases reported in the literature, one of which is referred to as “angioganglioglioma.”
Case Description:Two patients presented with acute onset of neurological symptoms, with magnetic resonance imaging (MRI) finding of cavernoma of the left middle cerebellar penduncle, and small mass of the chiasmatic region, respectively. After microsurgical excision, histopathological examination revealed mixed ganglioglioma and cavernous malformation in both cases. Postoperative course was uneventful, and follow-up MRI showed complete removal of the tumor with no recurrence after 4 years.
Conclusions:Angiogliomas are very uncommon tumors. In literature, we found different interpretations of such lesions, although they should most probably be considered as distinct pathological entities. Although the association of ganglioglioma with cavernoma is extremely rare, it could be considered as a most peculiar form of angioglioma, and supports the existence of angioganglioglioma.
Keywords: Angioglioma, brain tumor, cavernoma, ganglioglioma, mixed tumor
INTRODUCTION
Gangliogliomas are rare, mostly benign intraaxial tumors originating at various sites in the central nervous system (CNS). The term ganglioglioma was first introduced by Perkins in 1926, defining a neoplasm of both astrocytic and neuronal components.[
The term “angioglioma” has been used to describe glial neoplasm with features of both glioma and vascular malformation. The cases described are very few, and such a histological entity is only controversially accepted.[
In 2003, Kupnicka et al. first described an unusual brain tumor consisting of three components, namely, pylocytic astrocytoma, arteriovenous malformation (AVM)-like vascular proliferation, and gangliomatic proliferation. The term “angioganglioglioma” was proposed to define a transitional form between angioglioma and ganglioglioma.[
CASE HISTORY
Case 1
M.C., a 58-year-old male presented with sudden onset of headache and postural instability owing to recurrent bleeding from a known cavernous angioma of the left middle cerebellar peduncle. Compared with previous scan, the new magnetic resonance imaging (MRI) scan showed an increased lesion with recent bleeding [
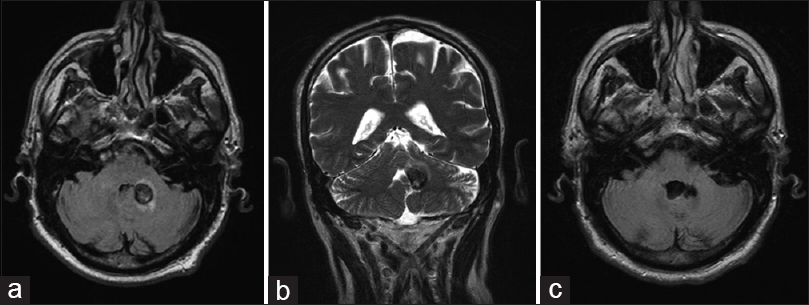
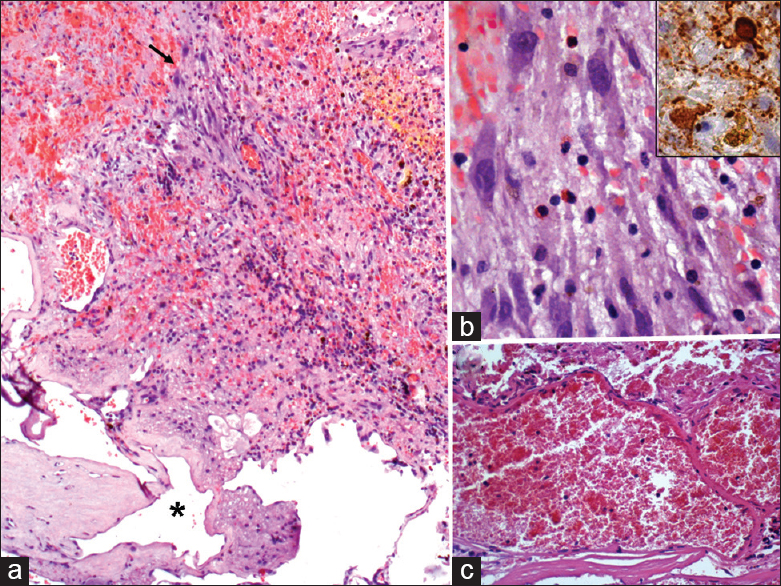
Figure 2
Case 1. (a) distinct tumor types in this picture, depicting ganglioglioma mixed with cavernous angioma at the bottom (asterisk). The arrow indicates the tumor area enlarged in b, showing ganglion cells intermingled with small lymphocytes, erythrocytes, and glial cells. (b) inset: synaptophysin-immunoreactive ganglion cells. (c) detail of cavernoma portion. (a-c) haematoxylin and eosin; original magnification: (a) ×50; (b), ×400; (c), ×200. (b) inset: automated immunohistochemistry, chromogen: diaminobenzidine; original magnification: ×400
Case 2
F.P., a 66-year-old male came to our emergency department for rapidly progressing visual disturbances. Brain MRI scan showed a small mass in the chiasmatic region [
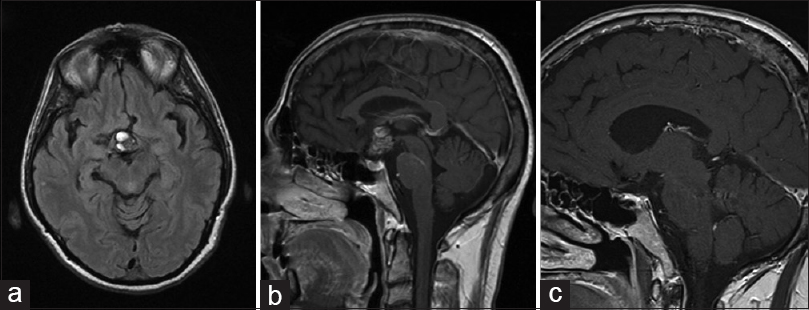
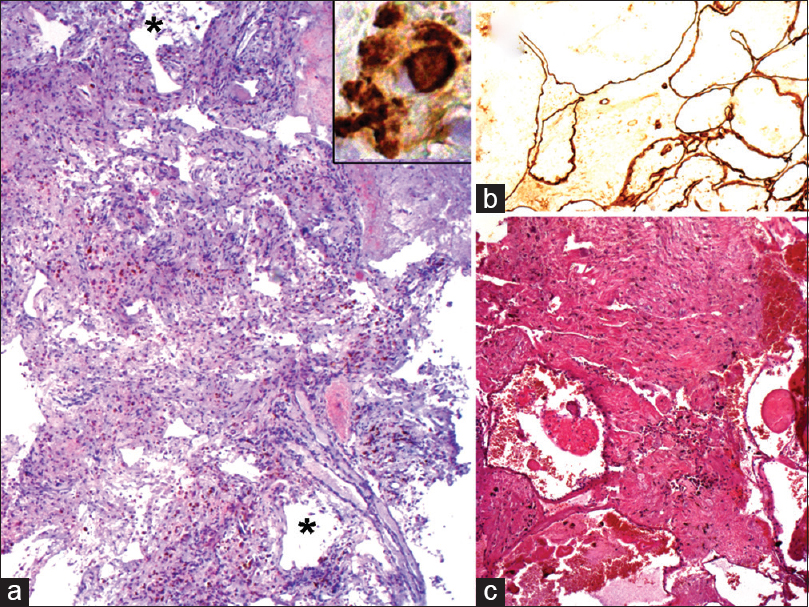
Figure 4
Case 2. (a) dilated vessels (as the ones indicated by asterisks) of the cavernous malformation admixed with tumor cells. (a) inset: ganglion cells are identified by immunopositivity for synaptophysin. (b) cavernous vessels are evidenced by endothelial positivity for CD34. (c) in another area, the cavernous portion (bottom of picture) is quite distinct from ganglioglioma. (a), and, (c) hematoxylin and eosin; original magnification: (a) ×25; (c) ×50; (a) inset, and (b) automated immunohistochemistry, chromogen: diaminobenzidine; original magnification: A, inset, ×400; (b) ×100
DISCUSSION
Although uncommon, the coexistence of a benign brain tumor, mostly glioma, and a vascular malformation (namely, cavernous malformation, or AVM) has been described and often referred to as angioglioma.[
Among the authors not considering angiogliomas as independent disease, Lombardi et al.[
Some authors[
Interestingly, Kupnicka et al.[
On the other hand, ganglioglioma are rare CNS tumours defined by the presence of neoplastic ganglion and glial cells.[
In both of our cases, cavernoma pattern was present, showing a complex of vascular spaces in varying sizes without intervening parenchyma, and endothelial positivity for CD34 [
CONCLUSION
In conclusion, we found several different interpretation of angiogliomas proposed in the literature.[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Councilman WT. The gliomatous tumors of the brain. Long Island Med J. 1914. 8: 401-9
2. Dash RC, Provenzale JM, McComb RD, Perry DA, Longee DC, McLendon RE. Malignant supratentorial ganglioglioma (ganglion cell-giant cell glioblastoma): A case report and review of the literature. Arch Pathol Lab Med. 1999. 12: 342-5
3. De Marchi R, Abu-Abed S, Munoz D, Loch MacDonald R. Malignant ganglioglioma: Case report and review of literature. J Neurooncol. 2011. 101: 311-8
4. Gazzeri R, De Bonis C, Carotenuto V, Catapano D, D’Angelo V, Galarza M. Association between cavernous angioma and cerebral glioma. Report of two cases and literature review of so-called angiogliomas. Neurocirugia. 2011. 22: 562-6
5. Hasegawa H, Bitoh S, Koshino K, Obashi J, Kobayashi Y, Kobayashi M. Mixed cavernous angioma and glioma (angioglioma) in the hypothalamus – Case report. Neurol Med Chir. 1995. 35: 238-42
6. Kupnicka DJ, Sikorska B, Klimek A, Kordek R, Liberski PP. Angioganglioglioma: A transitional form between angioglioma and ganglioglioma?. Ultrastruc Pathol. 2003. 27: 423-32
7. Licata C, Pasqualin A, Freschini A, Barone G, Da Pian R. Management of associated primary cerebral neoplasms and vascular malformations: 2.Intracranial arterio-venous malformations. Acta Neurochir. 1986. 83: 38-46
8. Lombardi D, Scheithauer BW, Piepgras D, Meyer FB, Forbes GS. “Angioglioma” and the arteriovenous malformation-glioma association. J Neurosurg. 1991. 75: 589-66
9. Mathern GW, Cornford ME, Athony Verity M. Angioglioma: Definition and reappraisal. J Neuropathol Exp Neurol. 1989. 48: 306-
10. Matyja E, Grajkowska W, Taraszewska A, Marchel A, Bojarski P, Nauman P. Advanced reactive astrogliosis associated with hemangioblastoma versus astroglial-vascular neoplasm (“angioglioma”). Folia Neuropathol. 2007. 45: 120-5
11. Palma L, Mastronardi L, Celli P, D’Addetta L. Cavernous angioma associated with oligo-astrocytoma-like proliferation. Report of two cases and review of the literature with a reappraisal of the term “angioglioma”. Acta Neurochir. 1995. 133: 169-73
12. Pant I, Suri V, Chaturvedi S, Dua R, Kanodia AK. Ganglioglioma of optic chiasm: Case report and review of the literature. Child Nerv Syst. 2006. 22: 717-20
13. Shuangshoti S, Kirsch E, Bannan P, Fabian VA. Ganglioglioma of the optic chiasm: Case report and review of the literature. AJNR Am J Neuroradiol. 2000. 21: 1486-9
14. Siddique K, Zagardo M, Guijrati M, Olivero V. Ganglioglioma presenting as a meningioma: Case report and review of the literature. Neurosurgery. 2002. 50: 1133-5
15. Yust-Katz S, Anderson MD, Liu D, Wu J, Yuan Y, Olar A. Clinical and prognostic features of adult patients with gangliogliomas. Neuro Oncol. 2014. 16: 409-13
16. Zentner J, Wolf HK, Ostertun B, Hufnagel A, Campos MG, Solymosi L. Gangliogliomas: Clinical, radiological, and histopathological findings in 51 patients. J Neurol Neurosurg Psychiatry. 1994. 57: 1497-502
17. Ziyal IM, Ece K, Bilginer B, Tezel GG, Özcan OE. A glioma with an arteriovenous malformation: An association or a different entity?. Acta Neurochir. 2004. 146: 83-6

