

- Department of Neurosurgery, Juntendo University, Faculty of Medicine, Bunkyo, Tokyo.
DOI:10.25259/SNI_214_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Yuzaburo Shimizu, Naohide Fujita, Osamu Akiyama, Mario Suzuki, Akihide Kondo. A rare presentation of a pediatric neurenteric cyst as an intra-axial pontine lesion: A case report with a 5-year follow-up. 06-Dec-2019;10:236
How to cite this URL: Yuzaburo Shimizu, Naohide Fujita, Osamu Akiyama, Mario Suzuki, Akihide Kondo. A rare presentation of a pediatric neurenteric cyst as an intra-axial pontine lesion: A case report with a 5-year follow-up. 06-Dec-2019;10:236. Available from: http://surgicalneurologyint.com/surgicalint-articles/9787/
Date of Submission
18-Nov-2019
Date of Acceptance
21-Nov-2019
Date of Web Publication
06-Dec-2019
Abstract
Background: Intracranial neurenteric cysts are rare, benign, and slow-growing tumors. However, we encountered a pediatric case that the cyst expansion occurred in a short period of time resulting in rapid deterioration of the patient’s symptoms.
Case Description: A previously healthy 7-year-old girl had a week history of dysarthric speech and diplopia along with headaches. Her magnetic resonance images (MRI) showed an abnormal cystic mass in her brainstem. Her symptoms were deteriorated for 1 month and her second MRI revealed an enlargement of the cystic lesion. The tumor biopsy and cyst drainage were carried out and histopathological examination of the cyst wall showed columnar epithelium containing ciliated cells. The final diagnosis of her tumor was neurenteric cyst.
Conclusion: We report a pediatric case of a neurenteric cyst in the brainstem, which expanded in a short period, and review this rare entity.
Keywords: Brainstem cyst, Neurenteric cyst, Pediatric brain tumor, Pons
INTRODUCTION
Neurenteric cysts are rare benign lesions that typically arise within the thoracic spine but can be encountered anywhere in the central nervous system from the cranium to the coccyx. Although over 140 cases of intracranial neurenteric cysts have been reported to date, brainstem neurenteric cysts are rare.[
CASE DESCRIPTION
A previously healthy 7-year-old girl was referred to our hospital for an abnormal cystic mass in her brainstem found using magnetic resonance imaging (MRI). She had a week history of dysarthric speech and diplopia along with headaches. Neurological examinations revealed facial and abducens nerve palsy on her left side. The MRI data showed a cystic mass measuring 22 mm×21 mm×18 mm, located in the pons with no connection to adjacent cisterns. The cystic component appeared as hypointense on the T1-weighted images, hyperintense on the T2-weighted images, and isointense on the diffusion- weighted images [
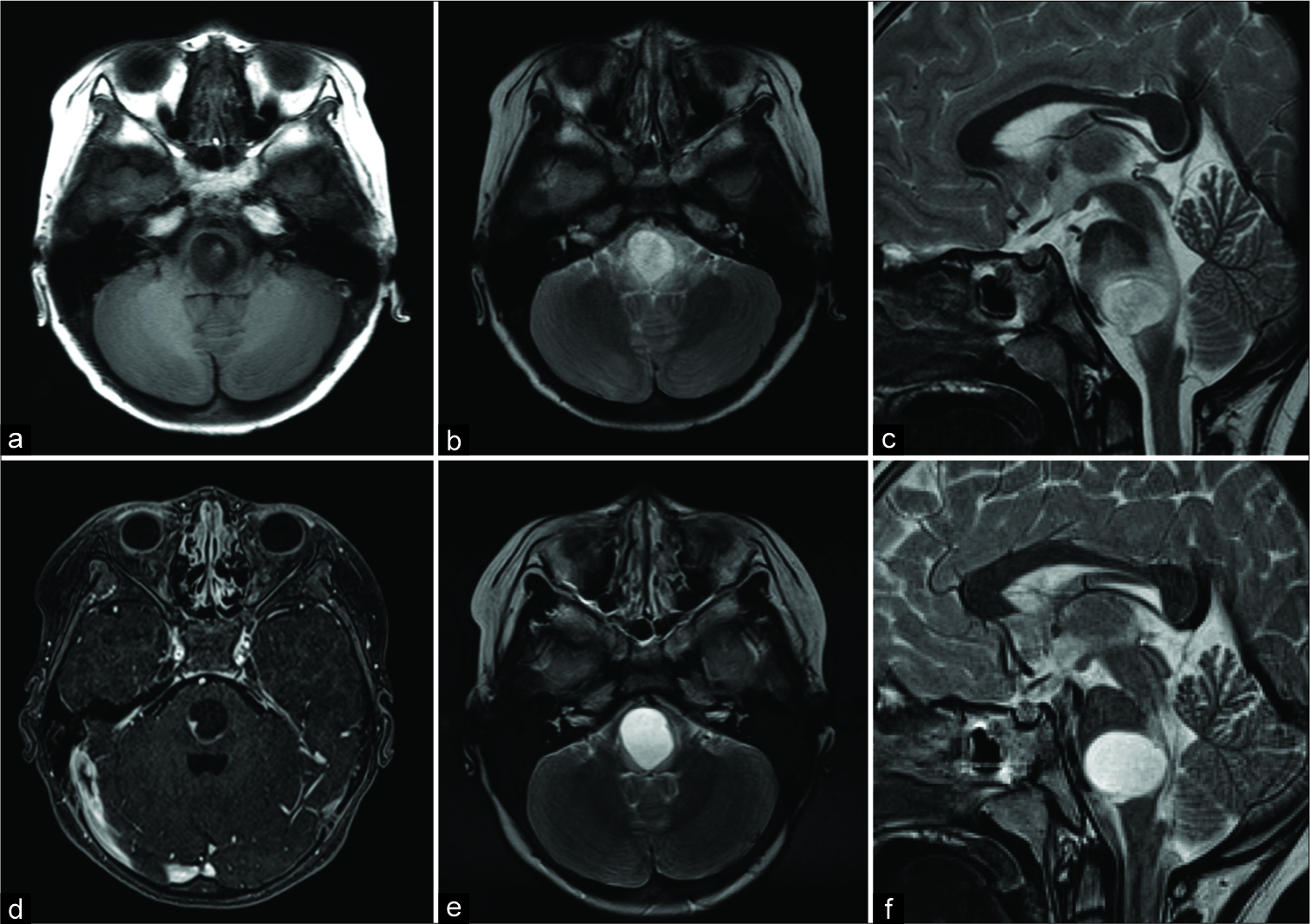
Figure 1:
Preoperative magnetic resonance (MR) images: (a) T1-weighted image (T1WI) showing cyst contents as hypointense, (b and c) axial and sagittal T2-weighted images (T2WI) showing a hyperintense cyst in the pons, (d) contrast-enhanced T1WI showing a mural nodule in the cyst, (e and f) subsequent magnetic resonance images (after 1 month) showing cyst enlargement in axial and sagittal T2WI.
Due to the patient’s progressive clinical course, tumor biopsy and cyst drainage were scheduled. The patient was placed in the prone position, and midline suboccipital craniotomy was performed. After dividing the arachnoid over the cisterna magna and cerebellomedullary fissure, the bilateral cerebellar hemispheres were gently retracted. The floor of the fourth ventricle was covered with the ependymal layer that appeared normal [
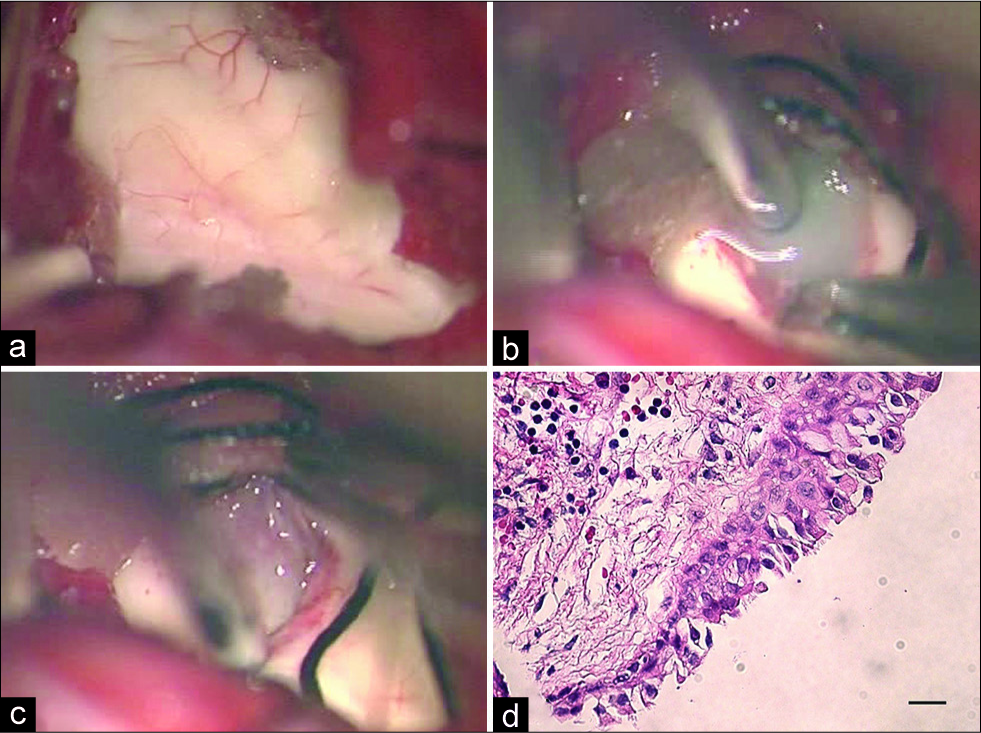
Figure 2:
Intraoperative imaging. (a) Intraoperative images through the microscope showing bilateral cerebellar hemispheres retraction exposing the intact fourth ventricle floor, (b and c) intraoperative images showing the presence of cyst containing milky white viscous fluid and mural nodule. (d) Histopathological examination of the cyst wall showed columnar epithelium containing ciliated cells.
DISCUSSION
The first neurenteric cysts were described by Kubie and Fulton, in 1928, as teratomatous cysts and later named neurenteric cysts in 1954 by Holcomb and Matson.[
Neurenteric cysts are considered to be benign and slow growing, with few studies reporting very gradual cyst expansion that occurs over several years.[
Complete surgical resection is the gold standard for the treatment of neurenteric cysts and is associated with the most favorable outcomes.[
CONCLUSION
We reported a case of a neurenteric cyst in the brainstem of a 7-year-old girl, which expanded in a short period, and review this rare entity. Neurenteric cysts in the brainstem should be considered to be distinct from other brainstem cystic lesions and need close observation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors thank the cooperation of this patient involved. The present study was supported by Juntendo.
References
1. Chen CT, Lee CY, Lee ST, Chang CN, Wei KC, Wu CT. Neurenteric cysts: Risk factors and management of recurrence. Acta Neurochir (Wien). 2016. 158: 1325-31
2. Cho JM, Ahn JY, Kim SH, Lee KS, Chang JH. An endodermal cyst mimicking an intra-axial tumor in the medulla oblongata. Childs Nerv Syst. 2010. 26: 853-6
3. Gauden AJ, Khurana VG, Tsui AE, Kaye AH. Intracranial neuroenteric cysts: A concise review including an illustrative patient. J Clin Neurosci. 2012. 19: 352-9
4. Holcomb GW, Matson DD. Thoracic neurenteric cyst. Surgery. 1954. 35: 115-21
5. Lach B, Russell N, Atack D, Benoit B. Intraparenchymal epithelial (enterogenous) cyst of the medulla oblongata. Can J Neurol Sci. 1989. 16: 206-10
6. Li T, Wu X, Zhang Y. A rare presentation of an enterogenous cyst as an intra-axial pontine lesion. World Neurosurg. 2017. 100: 707.e1-3
7. Nakajima M, Miyajima M, Hishii M, Arai H, Sato K, Fujii H. Endodermal cyst of the quadrigeminal cistern: Case report. Surg Neurol. 2001. 56: 385-8
8. Priamo FA, Jimenez ED, Benardete EA. Posterior fossa neurenteric cysts can expand rapidly: Case report. Skull Base Rep. 2011. 1: 115-24
9. Wang L, Zhang J, Wu Z, Jia G, Zhang L, Hao S. Diagnosis and management of adult intracranial neurenteric cysts. Neurosurgery. 2011. 68: 44-52
10. Yamamoto J, Shimajiri S, Akiba D, Nakano Y, Nishizawa S. Intracranial neurenteric cyst with an enhanced mural nodule and melanin pigmentation: Radiologic-pathologic correlation. World Neurosurg. 2017. 97: 758.e11-9
11. Zalatnai A. Neurenteric cyst of medulla oblongata--a curiosity. Neuropediatrics. 1987. 18: 40-1

