

- Department of Medicine, Escuela de Medicina y Ciencias de la Salud, Tecnologico de Monterrey, Monterrey, Mexico
- Neuroscience and Neurorestoration Research Group, Instituto de Neurología y Neurocirugía, Centro Médico Zambrano Hellion TecSalud, San Pedro Garza García, Mexico.
Correspondence Address:
Jose A. Figueroa-Sanchez, Department of Medicine, Escuela de Medicina y Ciencias de la Salud, Tecnologico de Monterrey, Neuroscience and Neurorestoration Research Group, Instituto de Neurología y Neurocirugía, Centro Médico Zambrano Hellion TecSalud, San Pedro Garza García, Mexico.
DOI:10.25259/SNI_381_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Jose A. Figueroa-Sanchez1,2, Hector R. Martinez1,2, Pablo J. Avalos-Montes2, Carlos A. Arreola-Aldape1,2, Jose Alberto Moran Guerrero1,2, Enrique Caro-Osorio1,2. A simple but effective solution for proximal mark absence on some microcatheters in intracranial aneurysm embolization: Technical note. 21-Jul-2023;14:257
How to cite this URL: Jose A. Figueroa-Sanchez1,2, Hector R. Martinez1,2, Pablo J. Avalos-Montes2, Carlos A. Arreola-Aldape1,2, Jose Alberto Moran Guerrero1,2, Enrique Caro-Osorio1,2. A simple but effective solution for proximal mark absence on some microcatheters in intracranial aneurysm embolization: Technical note. 21-Jul-2023;14:257. Available from: https://surgicalneurologyint.com/surgicalint-articles/12448/
Date of Submission
02-May-2023
Date of Acceptance
08-Jul-2023
Date of Web Publication
21-Jul-2023
Abstract
Background: Endovascular coil embolization is increasingly being used for the treatment of intracranial aneurysms and other pathologies such as arteriovenous (AV) malformations and AV fistulas. Appropriate embolization technique requires a microcatheter with two radiopaque marks, one proximal and one distal. We present an alternative coils deployment technique for intracranial aneurysms, using a microcatheter without a proximal radiopaque mark.
Methods: We describe the technique for embolization that was used in a 36-year-old female patient, in which we used a microcatheter without a proximal radiopaque mark for coil embolization of an intracranial aneurysm.
Results: We used a Headway Duo flow directed microcatheter for a coiling embolization of an intracranial aneurysm, solving the absence of the proximal radiopaque mark by cannulating the microcatheter with a Traxcess 0.014 microguidewire, and placing an external mark on the screen in the proximal portion of the microguidewire 30 mm radiopaque tip to indirectly mark the proximal mark of the microcatheter.
Conclusion: There is scarce evidence supporting the use of microcatheters with no proximal radiopaque mark for coil embolization. This report attempts to disclose how an easy and simple technique can be used as a rescue method to solve the proximal radiopaque mark absence during endovascular coil release procedures. To the best of our knowledge, this technique has not been previously described; therefore, its use is not widespread among neurointerventionists.
Keywords: Brain arteriovenous malformations, Coiling, Headway Dou flow directed microcatheter, Intracranial aneurysm, Radiopaque distal mark
INTRODUCTION
Since the development of the first coils described by Zubillaga et al. in 1994,[
An appropriate embolization technique with coils normally requires a microcatheter with two radiopaque marks, one proximal and one distal, which serve to identify the moment the coil enters the aneurysmal sac entirely and is considered as a safe point for coil release from the microcatheter. Several microcatheters on the market have this feature, such as the Echelon microcatheter from Medtronic Neurovascular, the Headway (17, 21, or 27) microcatheter from MicroVention, the SL10 microcatheter from Stryker Neurovascular, among others.[
We describe the embolization technique that was used in a 36-year-old female patient, which involved the use of a microcatheter without a proximal radiopaque mark for coil embolization of an intracranial aneurysm.
CASE AND TECHNICAL DESCRIPTION
A 36-year-old female patient diagnosed with Spetzler Martin 4 brain arteriovenous malformation (bAVM) underwent endovascular treatment at our institution. We identified an intranidal aneurysm during the endovascular super selective approach of bAVM using a Headway Duo flow directed microcatheter. When cannulating the aneurysm with the microcatheter, the absence of the proximal mark for coil release was noticed. Sometimes, particularly in flow directed microcatheters, this mark may be absent, preventing safe coil release.
Nevertheless, we solved this issue quickly and easily by cannulating the microcatheter with Traxces 0.014 microguidewire, which has a 30 mm radiopaque tip, and indirectly marking on the screen the proximal portion of the microguidewire [
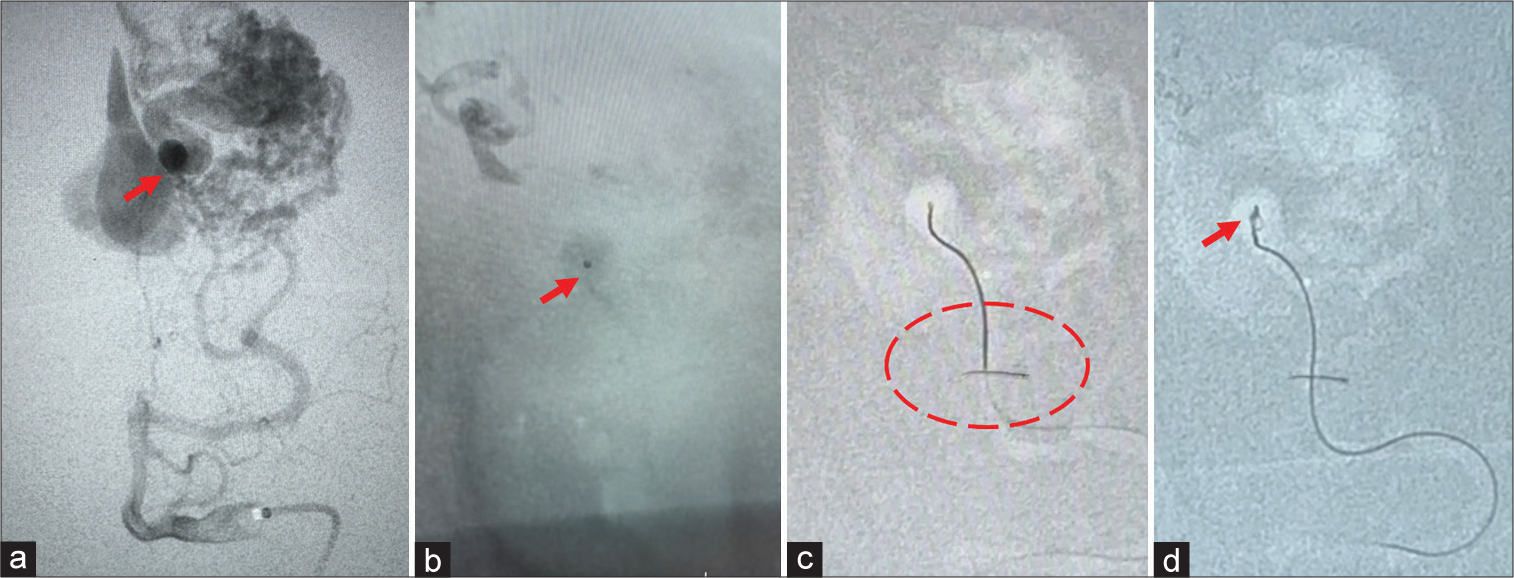
Figure 1:
Illustrative step by step technique used to treat the intranidal aneurysm. (a) Intranidal aneurysm (red arrow). (b) Headway Duo flow directed microcatheter with radiopaque distal mark (red arrow) and not radiopaque proximal mark. (c) Indirect mark on the screen that replicates the proximal mark of the microcatheter (inside red dotted circle). (d) Start of the embolization with coils (red arrow).
DISCUSSION
We successfully achieved intracranial aneurysm coiling using a Headway Duo Flow directed microcatheter. Care should be taken to readjust the manually placed external proximal mark whenever the distal marking of the microcatheter moves.
As background, we have evidence that Beckett et al.,[
Developing countries with limited access to medical devices and supplies for endovascular therapy can benefit from implementing this technique as a rescue step since it offers an alternative method for coil release without the need of specialized equipment with proximal radiopaque marks.
Limitations
It is important to note that this technique should not be implemented as a standard therapeutic approach. The safest way to perform coiling embolization is using a microcatheter with both radiopaque marks, guaranteeing a safe and adequate coil release. This technique should only be used as a rescue method in specific situations in which material availability and individual clinical scenarios do not allow for the use of an appropriate microcatheter designed for coil release. Equipment from different manufacturers can have variable distance between the proximal and distal marks, as well as subtle differences in the distance between the release portion of the coil delivery system and the release mark. For this reason, it can be risky to perform measurements with additional equipment such as a microguidewire. It is important to ensure that the flow-directed microcatheter and the coil delivery system have comparable lengths before starting the embolization procedure.
CONCLUSION
With this simple but effective modification to the endovascular technique, we demonstrate that coil deployment can be performed safely using a Headway Duo Flow directed microcatheter (or a variant with distal radiopaque marking) if a microguidewire with a 30 mm radiopaque tip length is available. This implies that patients who need two endovascular treatments (for example, a bAVM with an intranidal aneurysm, as in this case) can be treated with less materials, which reduces procedure cost.
To the best of our knowledge, this simple but effective variation in endovascular techniques has not been previously described in the literature. Therefore, its use has not been widespread among neurointerventionists. This could be of value especially for young neurointerventionists or trainees.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Beckett JS, Duckwiler GR, Tateshima S, Szeder V, Jahan R, Gonzalez N. Coil embolization through the Marathon microcatheter: Advantages and pitfalls. Interv Neuroradiol. 2017. 23: 28-33
2. Campos JK, Lien BV, Wang AS, Lin LM. Advances in endovascular aneurysm management: Coiling and adjunctive devices. Stroke Vasc Neurol. 2020. 5: 14-21
3. Fernandez Zubillaga A, Guglielmi G, Vinuela F, Duckwiler GR. Endovascular occlusion of intracranial aneurysms with electrically detachable coils: Correlation of aneurysm neck size and treatment results. AJNR Am J Neuroradiol. 1994. 15: 815-20
4. Harsan , editors. Basic endovascular technique for aneurysm coiling. Neurovascular Surgery. Singapore: Springer; 2019. p. 79-84
5. Kanemaru K, Ezura M, Nishiyama Y, Yagi T, Yoshioka H, Fukumoto Y. Anchor coil technique for arteriovenous fistula embolization: A technical note. Interv Neuroradiol. 2014. 20: 283-6
6. Leacy R, Ansari SA, Schirmer CM, Cooke DL, Prestigiacomo CJ, Bulsara KR. Endovascular treatment in the multimodality management of brain arteriovenous malformations: Report of the Society of NeuroInterventional Surgery Standards and Guidelines Committee. J Neurointerv Surg. 2022. 14: 1118-24
7. Liao M, Huynh K, Cicilioni K, Kumar RP. Endovascular coiling of fenestrated vertebrobasilar cerebral aneurysms. Neurointervention. 2022. 17: 195-9
8. Moran CJ, editors. Neurointervention, embolization materials. The Curated Reference Collection in Neuroscience and Biobehavioral Psychology. Netherlands: Elsevier Science Ltd; 2016. p. 400-5
9. Rodriguez JN, Hwang W, Horn J, Landsman TL, Boyle A, Wierzbicki MA. Design and biocompatibility of endovascular aneurysm filling devices. J Biomed Mater Res A. 2015. 103: 1577-94

