

- Department of Neurosurgery, Yokohama Sakae Kyosai Hospital, 132 Katsura-cho, Sakae-ku, Yokohama 247-8581, Japan
Correspondence Address:
Motohiro Nomura
Department of Neurosurgery, Yokohama Sakae Kyosai Hospital, 132 Katsura-cho, Sakae-ku, Yokohama 247-8581, Japan
DOI:10.4103/2152-7806.166179
Copyright: © 2015 Nomura M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Nomura M, Tamase A, Kamide T, Mori K, Seki S, Iida Y. Accessory middle cerebral artery associated with an unruptured aneurysm at its origin. Surg Neurol Int 28-Sep-2015;6:
How to cite this URL: Nomura M, Tamase A, Kamide T, Mori K, Seki S, Iida Y. Accessory middle cerebral artery associated with an unruptured aneurysm at its origin. Surg Neurol Int 28-Sep-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/accessory-middle-cerebral-artery-associated-with-an-unruptured/
Abstract
Background:An aneurysm originating from the junction of the A1 segment of the anterior cerebral artery and accessory middle cerebral artery (Acc-MCA) is markedly rare. We report a rare case of an Acc-MCA aneurysm, and discuss the clinical course and management of this rare condition.
Case Description:A 64-year-old man with a past history of cerebral infarction was revealed to have a left Acc-MCA and an aneurysm at its origin. The aneurysm was clipped via a transsylvian approach. Due to its location and projectile direction, the neck of the aneurysm was left partially unclipped.
Conclusion:Although an Acc-MCA aneurysm is very rare, it has a potential risk of rupture. Therefore, radical treatment is necessary for such aneurysms.
Keywords: Accessory, aneurysm, anomaly, anterior cerebral artery, middle cerebral artery
INTRODUCTION
Some anomalies of the middle cerebral artery (MCA), such as an accessory MCA (Acc-MCA) and a duplicated MCA have been reported.[
CASE REPORT
A 64-year-old man with a past history of diabetes mellitus, hypertension, and cerebral infarction experienced dysarthria. Diffusion-weighted magnetic resonance imaging showed a small fresh cerebral infarction in the left corona radiata. Three-dimensional computed tomography angiography [
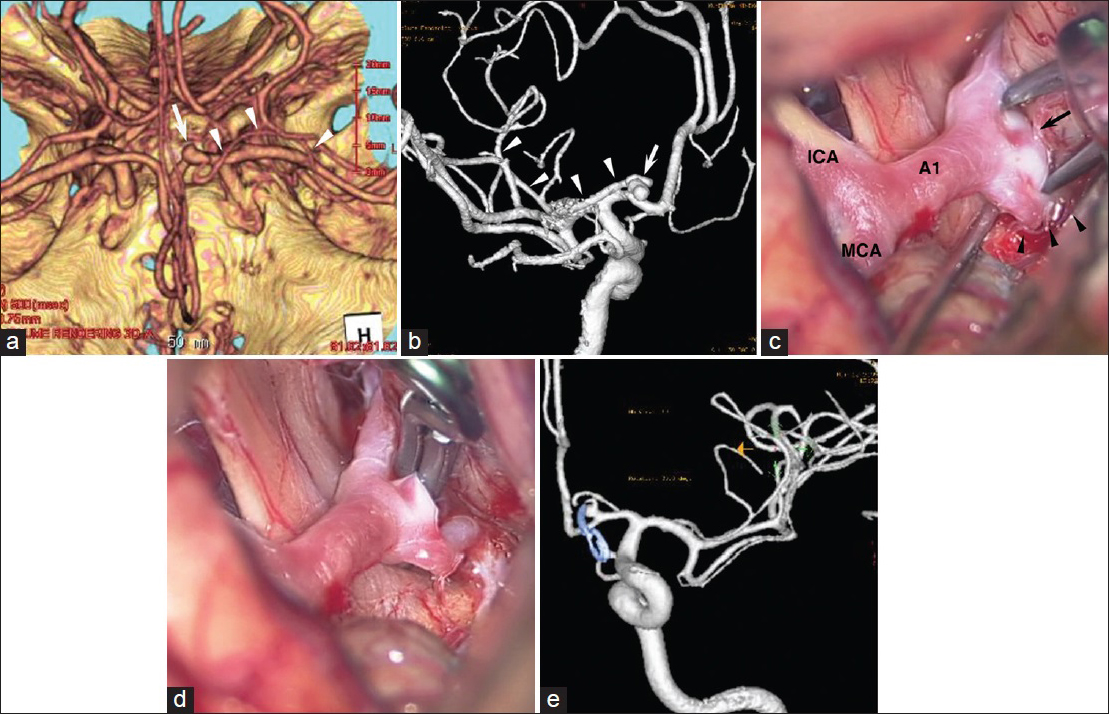
Figure 1
(a) Three-dimensional computed tomography angiography showing an aneurysm (arrow) at the origin of an accessory middle cerebral artery (arrowheads). (b) Angiography demonstrating an aneurysm (arrow) at the junction of A1 of the anterior cerebral artery and accessory middle cerebral artery. The accessory middle cerebral artery (arrowheads) runs laterally along with the middle cerebral artery. (c) An intra-operative photograph showing an aneurysm (arrow) at the origin of the accessory middle cerebral artery (arrowheads). The aneurysm is projecting medially. (d) An intra-operative photograph showing that the aneurysm is clipped. (e) Follow-up angiography obtained 27 months after the operation, showing a small residual neck of the aneurysm
DISCUSSION
An aneurysm with an Acc-MCA origin was first reported by Waga et al. in 1977.[
As for the direction of the aneurysm, most Acc-MCA aneurysms project medially.[
In our case, the aneurysm was directed medially. This direction was opposite to the operator. In the operation, the neck of the aneurysm was relatively difficult to observe. The Acc-MCA aneurysm is deeply located in front of the optic nerve. Therefore, careful intraoperative observation and dissection of the aneurysm neck are necessary for direct clipping. The subfrontal approach might be useful to observe the aneurysm. As for treatment, 12 cases including ours were clipped. Recently, a case which was embolized with platinum coils was reported.[
CONCLUSIONS
Although an Acc-MCA aneurysm is very rare, it has a risk of rupture due to hemodynamic factors. Therefore, radical treatment for an unruptured Acc-MCA aneurysm is necessary.
References
1. Fujiwara K, Saito K, Ebina T. Saccular aneurysm of the accessory middle cerebral artery – Case report. Neurol Med Chir (Tokyo). 2003. 43: 31-4
2. Han DH, Gwak HS, Chung CK. Aneurysm at the origin of accessory middle cerebral artery associated with middle cerebral artery aplasia: Case report. Surg Neurol. 1994. 42: 388-91
3. Lame A, Kaloshi G, Petrela M. Anatomic variants of accessory medial cerebral artery. Neurosurgery. 2010. 66: E1217-
4. Lee IH, Jeon P, Kim KH, Byun HS, Kim HJ, Kim ST. Endovascular treatment of a ruptured accessory middle cerebral artery aneurysm. J Clin Neurosci. 2010. 17: 383-4
5. Nakamura T, Houkin K, Saitoh H, Abe H. Aneurysm of the anterior communicating artery associated with accessory middle cerebral artery – Case report. Neurol Med Chir (Tokyo). 1997. 37: 747-51
6. Nomura M, Yamashima T, Kita D, Kida S, Kajinami K, Yamashita J. Duplication of the middle cerebral artery associated with an unruptured aneurysm. Acta Neurochir (Wien). 2000. 142: 221-2
7. Reis CV, Zabramski JM, Safavi-Abbasi S, Hanel RA, Deshmukh P, Preul MC. The accessory middle cerebral artery: Anatomic report. Neurosurgery. 2008. 63: 10-3
8. Umansky F, Dujovny M, Ausman JI, Diaz FG, Mirchandani HG. Anomalies and variations of the middle cerebral artery: A microanatomical study. Neurosurgery. 1988. 22: 1023-7
9. Waga S, Kojima T, Morooka Y, Sakakura M. Aneurysm of the accessory middle cerebral artery. Surg Neurol. 1977. 8: 359-60
10. Wakabayashi Y, Hori Y, Kondoh Y, Asano T, Yamada A, Kenai H. Ruptured anterior cerebral artery aneurysm at the origin of the accessory middle cerebral artery. Neurol Med Chir (Tokyo). 2011. 51: 645-8

