

- Department of Neurosurgery, University Hospital of Thessaly, University Hospital of Larissa, Biopolis, 41110 Larissa, Thessaly, Greece
- Center for Research and Technology of Thessaly, 38500 Larissa, Greece
Correspondence Address:
George Fotakopoulos
Department of Neurosurgery, University Hospital of Thessaly, University Hospital of Larissa, Biopolis, 41110 Larissa, Thessaly, Greece
Center for Research and Technology of Thessaly, 38500 Larissa, Greece
DOI:10.4103/2152-7806.176671
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Fotakopoulos G, Tsianaka E, Vagkopoulos K, Fountas KN. According to which factors in severe traumatic brain injury craniectomy could be beneficial. Surg Neurol Int 17-Feb-2016;7:19
How to cite this URL: Fotakopoulos G, Tsianaka E, Vagkopoulos K, Fountas KN. According to which factors in severe traumatic brain injury craniectomy could be beneficial. Surg Neurol Int 17-Feb-2016;7:19. Available from: http://surgicalneurologyint.com/surgicalint_articles/according-to-which-factors-in-severe-traumatic-brain-injury-craniectomy-could-be-beneficial/
Abstract
Background:To investigate the clinical outcome at 101 patients undergoing decompressive craniectomy (DC) after severe traumatic brain injury (TBI).
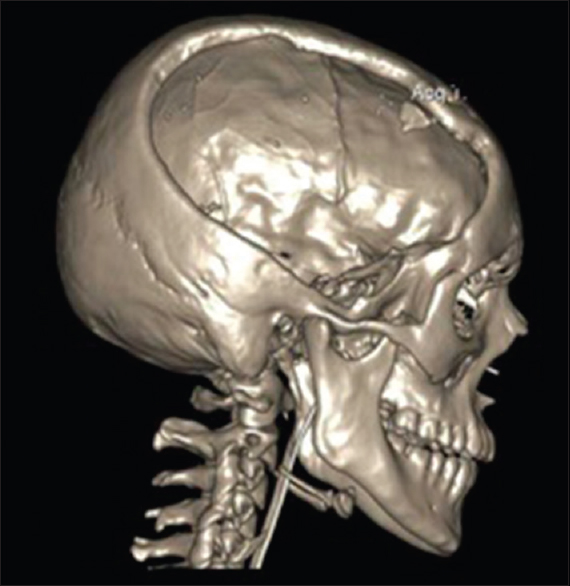
Methods:Age, Glasgow Coma Scale (GCS) at the time of intubation, and the intraoperative intracranial pressure (ICP) were recorded. Formal DC was performed in all cases and the square surface of bone flap was calculated in cm2 based on the length and the width from computed tomography scan.
Results:The difference of good neurological recovery (Glasgow outcome score 4–5), between patients with ICP ≤20 mmHg, GCS ≥5, age ≤60 years, and bone flap ≥130 cm2 and those with ICP >20 mmHg, GCS 60 years, and bone flap 2, was statistically significant.
Conclusion:Although the application of DC in severe TBI is controversial and the population in this study is small, our study demonstrates the threshold of the specific factors (patient age, ICP and GCS on the day of the surgery and the size of the bone flap) which may help in the decision of performing DC. Furthermore, this study proves that the different combinations and mainly at the same time involvement of all prognostic parameters (age 2, and ICP ≤20 at time of DC surgery) allow a better outcome.
Keywords: Brain trauma, decompressive craniectomy, severe brain injury
INTRODUCTION
Decompressive craniectomy (DC) is an old surgical technique, with varied usefulness for a wide range of pathologies.[
The main question in this procedure is whether the results justify the treatment as well as the associated complications and of course the functional outcome in surviving patients. The relationship between high ICP and poor outcome is very well documented.[
The purpose of this study was to analyze all those factors that play a key role in the outcome of patients who had undergone DC and lead to conclusions on whether and when this procedure can be beneficial.
MATERIALS AND METHODS
This is a retrospective study, with 101 patients undergoing DC after severe TBI and who had been submitted in our hospital during the last 5 years to reduce the ICP, were included. The study was approved by the Institutional Review Board of all the participating institutions. A signed written consent form was obtained from the participants or their legal representatives. The analysis of our data was performed according to the regulations of the current Health Insurance Portability and Accountability Act.
During 5-year period (2009–2013) in our department, 119 patients with severe TBI were admitted and from those 101 patients (84.9%), DC was performed. In 18 cases (15.2%) with severe TBI, ICP values were maintained under 12 mmHg with conservative methods (barbiturate coma, hyperventilation, hypertonic saline, and osmotic diuretics).
The mean age was 42.8 years (range 6–83 years). There were 81 (80.2%) men and 20 (19.8%) women. In all patients, brain computed tomography (CT) scan was performed before surgery. The initial brain CT scan included contusions (8 cases – 8%), fractures (12 cases – 12%), acute subdural hematoma (37 cases – 37%), epidural hematoma (7 cases – 7%), intraparenchymal (21 cases – 21%), intraventricular (7 cases – 7%) or subarachnoid (5 cases – 5%), hemorrhage, and/or brain edema (30 cases – 30%). The most common mechanism of injury was a motor vehicle crash followed by falls. Glasgow Coma Scale (GCS) at the time of intubation and intraoperative ICP were recorded. In the majority of cases in 99 patients (98.9%), GCS was <8. In 2 cases (1.9%), GCS of admission was 12 and after a decrease in level of consciousness and emergent intubation, DC was performed due to values of ICP >18 mmHg.
The basic criterion for performing DC were the values of ICP >18 mmHg. Early (approximately 1 h after admission) DC was performed in 86 patients (85.9%), and in the rest 25 patients (14.1%) after failure of all the conservative methods, DC was performed between the 4th and 6th day.
Formal DC [

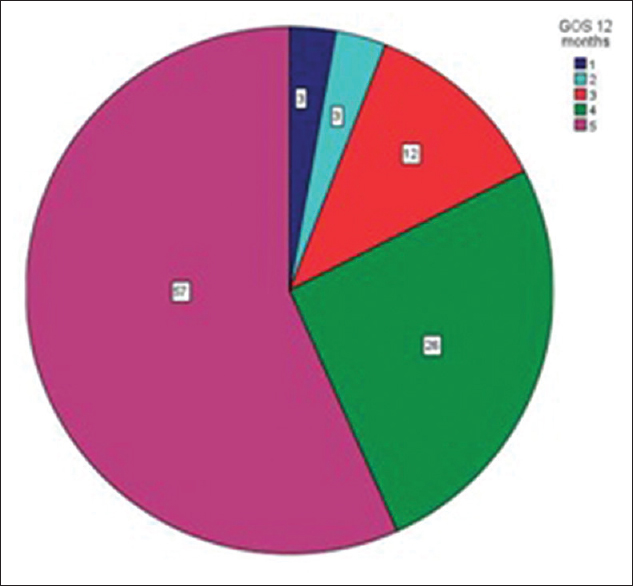
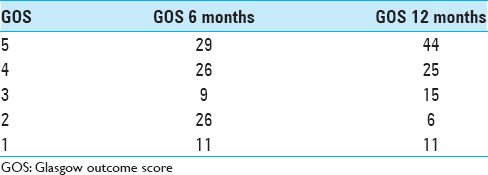
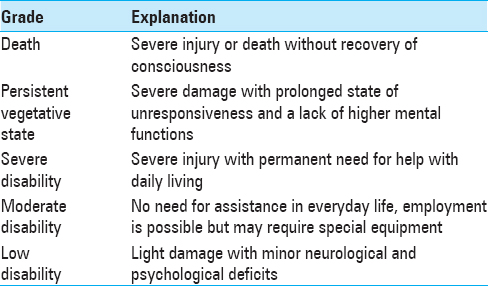
The clinical outcome was assessed with the Glasgow Outcome Score (GOS) score at 6 and 12 months follow-up, respectively [
RESULTS
In this study, following types of DC were performed: Right (48.2%), left (43.6%), and bilateral (8.2%). The most common complications during surgery were hemodynamic instability (15 cases – 15%) and hemorrhagic diathesis (10 cases – 10%). In two cases (1.9%), massive bleeding had occurred and in one of them, patient underwent hypovolemic shock and died. Other complications occurred postoperatively were bradycardia (2%), hypertension (1%), hypotension (1%), seizures (1%), hyperpyrexia (1.2%), difficulty in ventilation (1.2%), and rebleeding (1.2%). All these complications occurred either individually or in various combinations. The mortality, during surgery, was 1.9% (2 cases) and morbidity was 31.9% (32 cases) [
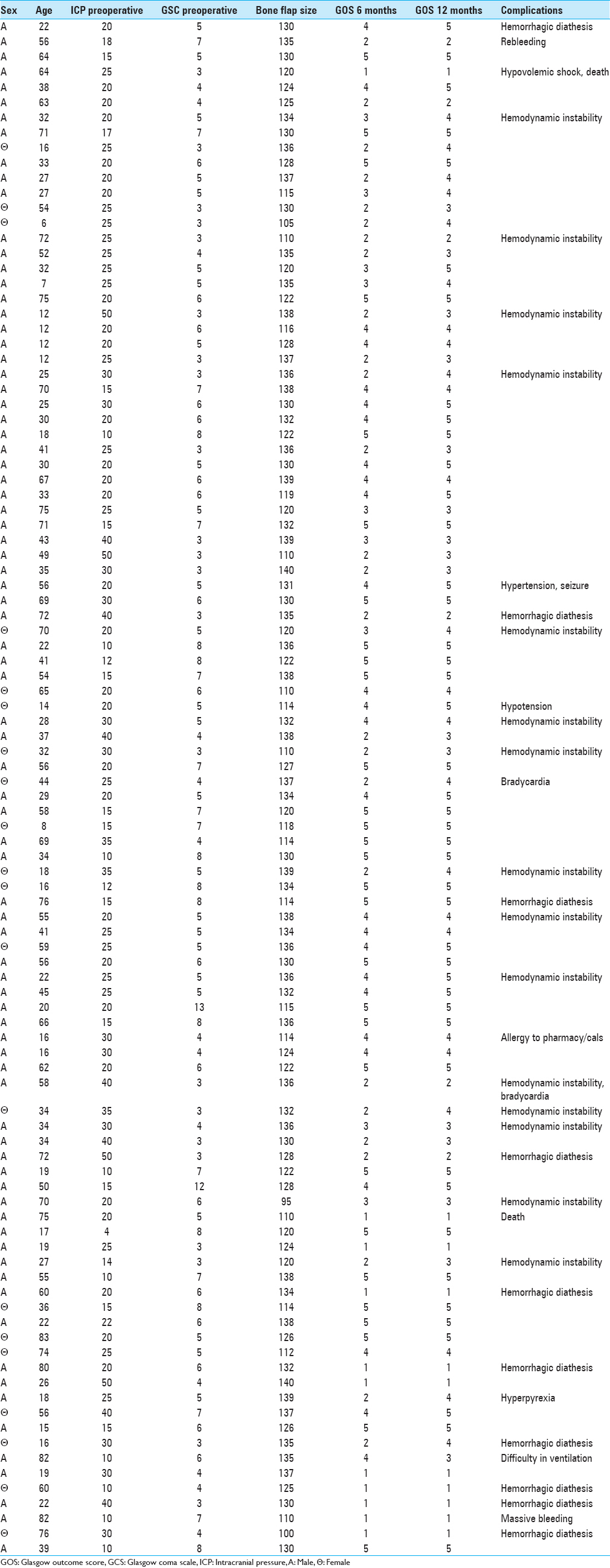
At 69 patients (68.9%) who had an ICP ≤20 at the time of surgery, GOS was ≥4 after 12 months. In 26 (25.9%) elderly (age >60) patients, 11 patients (10.9%) had GCS ≤5, and their outcome was poor (GOS <4). From 55 patients where the bone flap was ≥130 cm2, 36 of them (65.4%) had significantly better outcome according to GOS (≥4 after 12 months). However, in 10 patients who undergone a DC with bone flap ≤110 cm2, only in 2 cases (20%) had a clinical improvement (GOS ≥4 after 12 months). The difference of good neurological recovery ([GOS 4–5] – threshold ≥4), between patients with ICP ≤ 20 mmHg, GCS ≥5, age ≤60 years, and bone flap ≥130 cm2 and those with ICP >20 mmHg, GCS <5, age >60 years, and bone flap <130 cm2, was statistically significant. For 6 and 12 months follow-up, the two-tailed P < 0.0001, respectively, and is considered to be extremely statistically significant. According to GOS [
DISCUSSION
Diffuse brain swelling is the most common cause of morbidity and death after severe head injury in pediatric and adult patients.[
Despite these various studies, the effect of DC on clinical outcome after TBI is not yet clear. Although DC proved by DECRA study still remains questioning, there are suggesting an improvement in those patients.[
There are many prognostic factors affecting the outcome in severe TBI after DC such as age, lowest recorded GCS, presence of cranial fracture, absence of pupillary response/brainstem reflexes, respiratory insufficiency, refractory rise in ICP and the status of the basal cisterns or third ventricle on CT scan, the volume and location of the lesion, and the timing of surgery.[
The increased ICP is related with poor outcome after head injury, and ICP-guided therapy is commonly used.[
The lowest recorded GCS and the worse outcome were also reported in other studies.[
In our study, 55 patients had undergone DC with bone flap ≥130 cm2 and 36 of them (65.4%) had significantly better outcome according to GOS (≥4 after 12 months). On the other hand, in 10 patients with bone flap ≤110 cm2, only 2 (≈20%) had a clinical improvement (GOS ≥ 4 after 12 months). This shows a strong correlation between the outcome and size of bone flap. In addition, this study proves that the different combinations and mainly at the same time involvement of all prognostic parameters (age <60, GCS <5, bone flap ≥130 cm2 and ICP ≤20 at time of DC surgery) allow a better outcome (P = 0.0001 extremely statistically significant).
According to specific factors and their thresholds, our data can contribute to the decision of when to perform DC after severe TBI to be life-saving procedure and to minimize complications.
CONCLUSION
DC as a treatment option in patients with TBI has been a lot criticized and still remains controversial. Although studies such as DECRA have come up with results that consider DC as not a favorable option according to patients’ outcome, other ongoing studies such as RESCUE-ICP are main to add some more light in the dark field of the best optional treatment. This study and its results tries to emphasize on specific factors under which DC could be beneficial and helps us decide not only if DC should be performed or not but also when and under which specific circumstances it should be performed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Commentary
- Editor-in-Chief, University of California, Los Angeles, CA, USA E-mail:
jia@surgicalneurologyint.com
This paper continues a concept that is common in medicine that chronological age is a marker to be used in treatment. Chronological age is a biased view of aging across all modern cultures except those in which aging is a mark of respect and wisdom. Physiological age would be a better parameter to use. I challenge someone to develop this metric. Physiological age is a measure of the patients total body health. Chronological age does not measure this total body health but only a number in which are mixed many people in various stages of health. This physiological age would apply to all. It would apply to the very young with multisystem disease, who have little hope for recovery. It applies to all ages and avoids the bias that because someone is over 60 or 70, they have lived a full life and there is no use in prolonging it. Studies have reported that life expectancy will be 100 years for those born in the 21st century. Some cite 140 years as the expected life expectancy in the 21st century. Only a review of history will reveal that Hunter Gatherers lived until the age of 20 while during more civilized societies the ages extended to 40 years by the 1900s. In the past 100 years, life expectancy has doubled to 80 years and with some extension of that recently to 90 years. So, how does an arbitrary number of 60 of 70 apply to what will represent 30% of the population of many cultures but 2050. This concept makes no sense. Those now who are young and overweight (2/3 of the world population) will suffer earlier deaths from diabetes and hypertension and other diseases. Hence, I would expect that their physiological age will be higher than those who do not have these diseases or obesity. So, I predict that in the 21st century, we will see a subset of the young dying early and others living longer. Only a physiological age evaluation will make sense and add to the medical decisions governing treatment, no chronological age.
Most papers written using age do not consider this factor. Certainly people as they age have a higher chance of more diseases, but many are living well and contributing to society. Older people are more sensitive to drugs and must be treated as newborns with great care for their sensitivities to many treatments. So, to me papers that use an age as a cutoff without defining the health of the over 60/70 population are not valuable in guiding management decisions. That criticism applies to virtually all the studies written in the past decades.
It is time to start thinking differently about age and move into the 21st century on this subject of aging and medicine. This aging concept is a bias of societies worldwide. It will be rejected by the Boomers all over the world who are looking for a long productive life.
References
1. Aarabi B, Hesdorffer DC, Ahn ES, Aresco C, Scalea TM, Eisenberg HM. Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J Neurosurg. 2006. 104: 469-79
2. Albanèse J, Leone M, Alliez JR, Kaya JM, Antonini F, Alliez B. Decompressive craniectomy for severe traumatic brain injury: Evaluation of the effects at one year. Crit Care Med. 2003. 31: 2535-8
3. Andrews BT, Pitts LH. Functional recovery after traumatic transtentorial herniation. Neurosurgery. 1991. 29: 227-31
4. Arac A, Blanchard V, Lee M, Steinberg GK. Assessment of outcome following decompressive craniectomy for malignant middle cerebral artery infarction in patients older than 60 years of age. Neurosurg Focus. 2009. 26: E3-
5. Balan C, Alliez B. Decompressive craniectomy – From option to standard – Part I. Rom Neurosurg. 2009. 2: 20-6
6. Bohman LE, Schuster JM. Decompressive craniectomy for management of traumatic brain injury: An update. Curr Neurol Neurosci Rep. 2013. 13: 392-
7. Bullock MR, Chesnut R, Ghajar J, Gordon D, Hartl R, Newell DW. Surgical management of acute subdural hematomas. Neurosurgery. 2006. 58: S16-24
8. Bullock MR, Chesnut R, Ghajar J, Gordon D, Hartl R, Newell DW. Surgical management of traumatic parenchymal lesions. Neurosurgery. 2006. 58: S25-46
9. Clark K, Nash TM, Hutchison GC. The failure of circumferential craniotomy in acute traumatic cerebral swelling. J Neurosurg. 1968. 29: 367-71
10. Cooper PR, Hagler H, Clark WK, Barnett P. Enhancement of experimental cerebral edema after decompressive craniectomy: Implications for the management of severe head injuries. Neurosurgery. 1979. 4: 296-300
11. Coplin WM, Cullen NK, Policherla PN, Vinas FC, Wilseck JM, Zafonte RD. Safety and feasibility of craniectomy with duraplasty as the initial surgical intervention for severe traumatic brain injury. J Trauma. 2001. 50: 1050-9
12. Eghwrudjakpor PO, Allison AB. Decompressive craniectomy following brain injury: Factors important to patient outcome. Libyan J Med. 2010. p. 5-
13. Eisenberg HM, Frankowski RF, Contant CF, Marshall LF, Walker MD. High-dose barbiturate control of elevated intracranial pressure in patients with severe head injury. J Neurosurg. 1988. 69: 15-23
14. Elwatidy S. Bifrontal decompressive craniotomy for malignant brain edema. Saudi Med J. 2006. 27: 1547-53
15. Engberg M, Oberg B, Christensen KS, Pedersen MB, Cold GE. The cerebral arterio-venous oxygen content differences (AVDO2) during halothane and neurolept anaesthesia in patients subjected to craniotomy. Acta Anaesthesiol Scand. 1989. 33: 642-6
16. Engelhard K, Müller-Forell W, Werner C. Therapy of head trauma. Anaesthesist. 2008. 57: 1219-31
17. Formicola V, Cammellini S, Caramella D, Del Lucchese A, Goude G, Saccone M. An unusual surgical treatment of the skull following trauma during the copper age (IV millennium B.C.) in Italy. J Anthropol Sci. 2012. 90: 199-200
18. Goldstein MS. Human paleopathology. J Natl Med Assoc. 1963. 55: 100-6
19. Guerra WK, Gaab MR, Dietz H, Mueller JU, Piek J, Fritsch MJ. Surgical decompression for traumatic brain swelling: Indications and results. J Neurosurg. 1999. 90: 187-96
20. Hacke W, Schwab S, Horn M, Spranger M, De Georgia M, von Kummer R. ‘Malignant’ middle cerebral artery territory infarction: Clinical course and prognostic signs. Arch Neurol. 1996. 53: 309-15
21. Heinsius T, Bogousslavsky J, Van Melle G. Large infarcts in the middle cerebral artery territory. Etiology and outcome patterns. Neurology. 1998. 50: 341-50
22. Honeybul S, Ho KM, Lind CR. What can be learned from the DECRA study. World Neurosurg. 2013. 79: 159-61
23. Honeybul S, Ho KM. Decompressive craniectomy for severe traumatic brain injury: The relationship between surgical complications and the prediction of an unfavourable outcome. Injury. 2014. 45: 1332-9
24. Honeybul S. Complications of decompressive craniectomy for head injury. J Clin Neurosci. 2010. 17: 430-5
25. Hutchinson PJCorteen ECzosnyka MMendelow ADMenon DKMitchell P. www.RESCUEicp.com.
26. Kapadia FN, Masurkar VA, Sankhe MS, Gursahani RD. An audit of decompressive craniectomies. Indian J Crit Care Med. 2006. 10: 21-4
27. Kjellberg RN, Prieto A. Bifrontal decompressive craniotomy for massive cerebral edema. J Neurosurg. 1971. 34: 488-93
28. Kshettry VR, Mindea SA, Batjer HH. The management of cranial injuries in antiquity and beyond. Neurosurg Focus. 2007. 23: E8-
29. Kunze E, Meixensberger J, Janka M, Sörensen N, Roosen K. Decompressive craniectomy in patients with uncontrollable intracranial hypertension. Acta Neurochir Suppl. 1998. 71: 16-8
30. Marshall LF, SMith RW, Rauscher LA, Shapiro HM. Mannitol dose requirements in brain-injured patients. J Neurosurg. 1978. 48: 169-72
31. Marshall LF, Smith RW, Shapiro HM. The outcome with aggressive treatment in severe head injuries.Part II: Acute and chronic barbiturate administration in the management of head injury. J Neurosurg. 1979. 50: 26-30
32. Marshall LF, Toole BM, Bowers SA. The national traumatic coma data bank. Part 2: Patients who talk and deteriorate: Implications for treatment. J Neurosurg. 1983. 59: 285-8
33. Miller JD, Becker DP, Ward JD, Sullivan HG, Adams WE, Rosner MJ. Significance of intracranial hypertension in severe head injury. J Neurosurg. 1977. 47: 503-16
34. Missios S. Hippocrates, Galen, and the uses of trepanation in the ancient classical world. Neurosurg Focus. 2007. 23: E11-
35. Mori K, Aoki A, Yamamoto T, Horinaka N, Maeda M. Aggressive decompressive surgery in patients with massive hemispheric embolic cerebral infarction associated with severe brain swelling. Acta Neurochir (Wien). 2001. 143: 483-91
36. Moulin DE, Lo R, Chiang J, Barnett HJ. Prognosis in middle cerebral artery occlusion. Stroke. 1985. 16: 282-4
37. Münch E, Horn P, Schürer L, Piepgras A, Paul T, Schmiedek P. Management of severe traumatic brain injury by decompressive craniectomy. Neurosurgery. 2000. 47: 315-22
38. Narayan RK, Kishore PR, Becker DP, Ward JD, Enas GG, Greenberg RP. Intracranial pressure: To monitor or not to monitor?. A review of our experience with severe head injury. J Neurosurg. 1982. 56: 650-9
39. Olivecrona M, Rodling-Wahlström M, Naredi S, Koskinen LO. Effective ICP reduction by decompressive craniectomy in patients with severe traumatic brain injury treated by an ICP-targeted therapy. J Neurotrauma. 2007. 24: 927-35
40. Ong YK, Goh KY, Chan C. Bifrontal decompressive craniectomy for acute subdural empyema. Childs Nerv Syst. 2002. 18: 340-3
41. Oppenheim C, Samson Y, Manaï R, Lalam T, Vandamme X, Crozier S. Prediction of malignant middle cerebral artery infarction by diffusion-weighted imaging. Stroke. 2000. 31: 2175-81
42. Piek J. Decompressive surgery in the treatment of traumatic brain injury. Curr Opin Crit Care. 2002. 8: 134-8
43. Polin RS, Shaffrey ME, Bogaev CA, Tisdale N, Germanson T, Bocchicchio B. Decompressive bifrontal craniectomy in the treatment of severe refractory posttraumatic cerebral edema. Neurosurgery. 1997. 41: 84-92
44. Reddy AK, Saradhi V, Panigrahi M, Rao TN, Tripathi P, Meena AK. Decompressive craniectomy for stroke: Indications and results. Neurol India. 2002. 50: 66-9
45. Rengachary SS, Batnitzky S, Morantz RA, Arjunan K, Jeffries B. Hemicraniectomy for acute massive cerebral infarction. Neurosurgery. 1981. 8: 321-8
46. Rifkinson-Mann S. Cranial surgery in ancient Peru. Neurosurgery. 1988. 23: 411-6
47. Ruf B, Heckmann M, Schroth I, Hügens-Penzel M, Reiss I, Borkhardt A. Early decompressive craniectomy and duraplasty for refractory intracranial hypertension in children: Results of a pilot study. Crit Care. 2003. 7: R133-8
48. Sahuquillo J, Martínez-Ricarte F, Poca MA. Decompressive craniectomy in traumatic brain injury after the DECRA trial. Where do we stand?. Curr Opin Crit Care. 2013. 19: 101-6
49. Schwab S, Steiner T, Aschoff A, Schwarz S, Steiner HH, Jansen O. Early hemicraniectomy in patients with complete middle cerebral artery infarction. Stroke. 1998. 29: 1888-93
50. Seppelt I. Intracranial hypertension after traumatic brain injury. Indian J Crit Care Med. 2004. 8: 120-6
51. Stiver SI. Complications of decompressive craniectomy for traumatic brain injury. Neurosurg Focus. 2009. 26: E7-
52. Stocchetti N, Penny KI, Dearden M, Braakman R, Cohadon F, Iannotti F. Intensive care management of head-injured patients in Europe: A survey from the European brain injury consortium. Intensive Care Med. 2001. 27: 400-6
53. Timofeev I, Czosnyka M, Nortje J, Smielewski P, Kirkpatrick P, Gupta A. Effect of decompressive craniectomy on intracranial pressure and cerebrospinal compensation following traumatic brain injury. J Neurosurg. 2008. 108: 66-73
54. Vahedi K, Hofmeijer J, Juettler E, Vicaut E, George B, Algra A. Early decompressive surgery in malignant infarction of the middle cerebral artery: A pooled analysis of three randomised controlled trials. Lancet Neurol. 2007. 6: 215-22
55. Wani AA, Dar TI, Ramzan AU, Malik NK, Kirmani AR, Bhatt AR. Decompressive craniectomy in head injury. Indian J Neurotrauma. 2009. 6: 103-10
56. Waziri A, Fusco D, Mayer SA, McKhann GM, Connolly ES. Postoperative hydrocephalus in patients undergoing decompressive hemicraniectomy for ischemic or hemorrhagic stroke. Neurosurgery. 2007. 61: 489-93
57. Weiner GM, Lacey MR, Mackenzie L, Shah DP, Frangos SG, Grady MS. Decompressive craniectomy for elevated intracranial pressure and its effect on the cumulative ischemic burden and therapeutic intensity levels after severe traumatic brain injury. Neurosurgery. 2010. 66: 1111-8
58. Williams RF, Magnotti LJ, Croce MA, Hargraves BB, Fischer PE, Schroeppel TJ. Impact of decompressive craniectomy on functional outcome after severe traumatic brain injury. J Trauma Inj Infect Crit Care. 2009. 66: 1570-6
59. Ziai WC, Port JD, Cowan JA, Garonzik IM, Bhardwaj A, Rigamonti D. Decompressive craniectomy for intractable cerebral edema: Experience of a single center. J Neurosurg Anesthesiol. 2003. 15: 25-32

