

- Department of Neurosurgery, Yokohama Sakae Kyosai Hospital, Sakae-ku, Yokohama 247-8581, Japan
Correspondence Address:
Motohiro Nomura
Department of Neurosurgery, Yokohama Sakae Kyosai Hospital, Sakae-ku, Yokohama 247-8581, Japan
DOI:10.4103/2152-7806.168069
Copyright: © 2015 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Iida Y, Tamase A, Kamide T, Mori K, Seki S, Nomura M. Aneurysm at origin of duplicated middle cerebral artery associated with another aneurysm. Surg Neurol Int 23-Oct-2015;6:
How to cite this URL: Iida Y, Tamase A, Kamide T, Mori K, Seki S, Nomura M. Aneurysm at origin of duplicated middle cerebral artery associated with another aneurysm. Surg Neurol Int 23-Oct-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/aneurysm-at-origin-of-duplicated-middle-cerebral-artery/
Abstract
Background:A duplicated middle cerebral artery (DMCA) is a rare vessel anomaly. Aneurysms at the origin of DMCA have been reported.
Case Description:We report 2 cases of aneurysms at the origin of DMCA accompanied by aneurysms at different sites. Each case of ruptured and unruptured aneurysm at the DMCA origin was associated with an unruptured aneurysm at the ipsilateral internal carotid artery and a ruptured one at the ipsilateral MCA, respectively. The aneurysms were clipped successfully in both patients.
Conclusion:In cases of DMCA aneurysm associated with an aneurysm at another site, either aneurysm has a high risk of rupture. In such a case, radical treatment is necessary.
Keywords: Aneurysm, anomaly, duplicated, middle cerebral artery
INTRODUCTION
Some anomalies of the middle cerebral artery (MCA) have been reported on autopsy and radiological examinations.[
In this report, we describe the patients with DMCA aneurysms and discuss the clinical course, radiological findings, and management of this rare aneurysm.
CASE PRESENTATION
Case 1
A 41-year-old woman without any significant past history experienced sudden-onset headache and vomiting. Computed tomography (CT) on admission showed subarachnoid hemorrhage (SAH) [
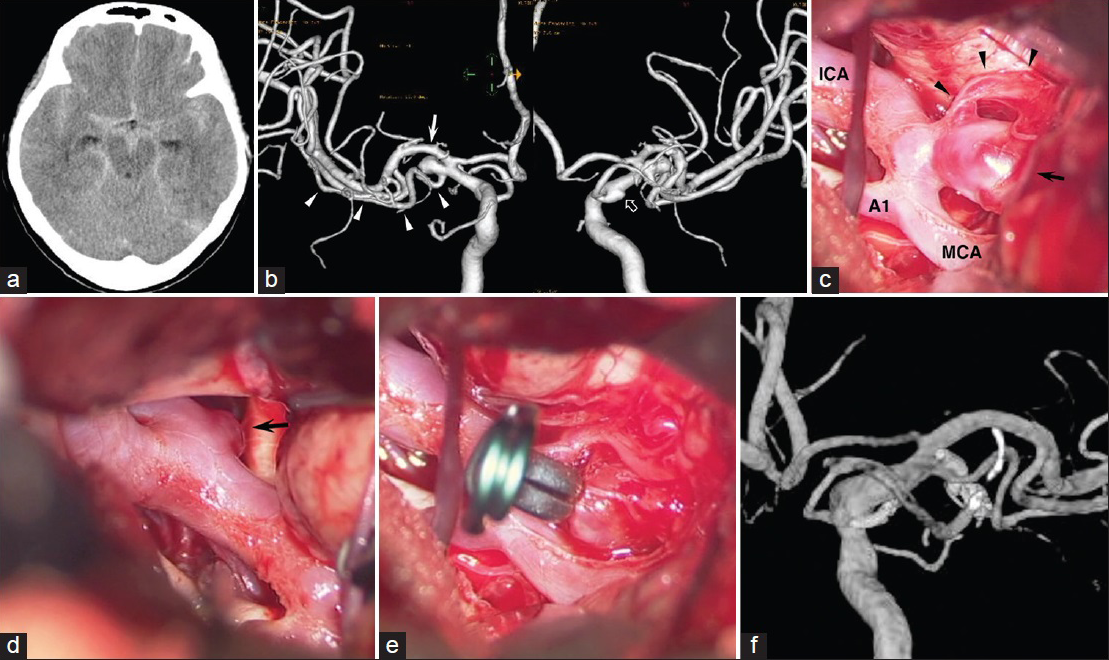
Figure 1
Case 1. (a) Computed tomography on admission showing subarachnoid hemorrhage. (b) Angiography showing the right duplicated middle cerebral artery (arrowheads) and an aneurysm (arrow) at its origin. Angiography also showing a small internal carotid artery-posterior communicating artery aneurysm (open arrow). (c) An intra-operative photograph showing duplicated middle cerebral artery (arrowheads) and the aneurysm (arrow). (d) An intra-operative photograph also demonstrating the internal carotid artery-posterior communicating artery aneurysm (arrow). (e) The duplicated middle cerebral artery aneurysm is clipped. (f) Angiography obtained 8 years after onset, showing no recurrence of the aneurysms
Case 2
A 76-year-old woman was revealed to have a right MCA aneurysm at the M1/M2 junction and a right DMCA aneurysm on magnetic resonance imaging 6 years ago [
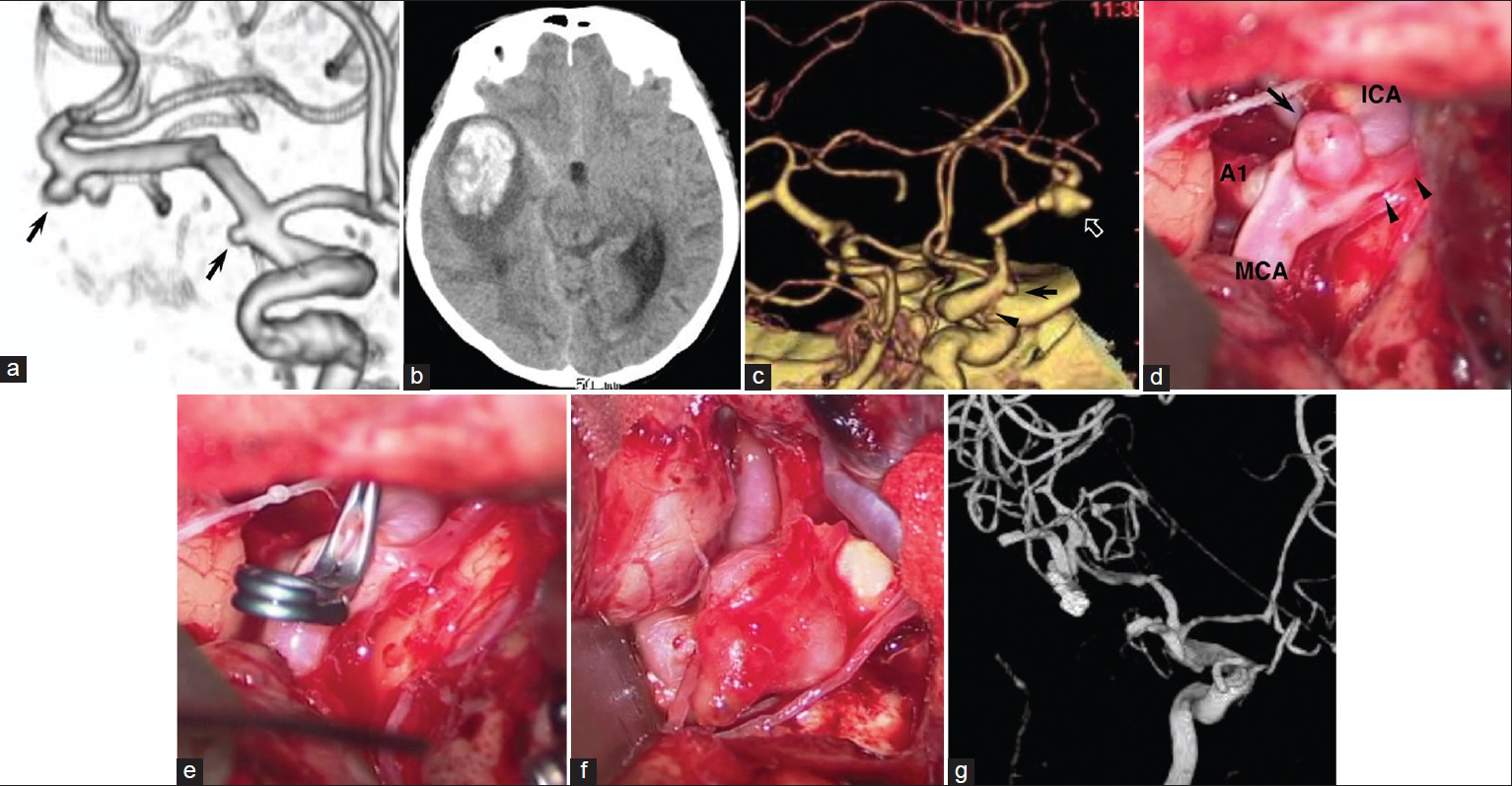
Figure 2
Case 2. (a) Magnetic resonance imaging obtained 6 years previously showing two aneurysms on the right middle cerebral artery and the origin of duplicated middle cerebral artery. (b) Computed tomography on admission showing subarachnoid hemorrhage and intracerebral hemorrhage in the right temporal lobe. (c) Three-dimensional computed tomography angiography showing the right duplicated middle cerebral artery (arrowhead) and an aneurysm (arrow) at its origin. Three-dimensional computed tomography angiography also showing the right middle cerebral artery aneurysm (open arrow). (d) An intra-operative photograph showing duplicated middle cerebral artery (arrowheads), and the aneurysm (arrow) at its origin. (e) The unruptured duplicated middle cerebral artery aneurysm is successfully clipped. (f) An intra-operative photograph showing the ruptured middle cerebral artery aneurysm. (g) Postoperative angiography showing the disappearance of the aneurysms
DISCUSSION
An aneurysm at the DMCA origin was initially reported by Crompton and Lond in 1962.[
Kai et al.[
CONCLUSIONS
More than half of the cases of DMCA aneurysms have multiple aneurysms. It is suggested that hemodynamic stress might contribute to formation and enlargement of multiple aneurysms. Therefore, the presence of a DMCA aneurysm along with another aneurysm is associated with a high risk of rupture. In such a case, radical treatment is necessary.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chang HY, Kim MS. Middle cerebral artery duplication: classification and clinical implications. J Korean Neurosurg Soc. 2011. 49: 102-6
2. Crompton MR, Lond MB. The pathology of ruptured middle-cerebral aneurysms with special reference to the differences between the sexes. Lancet. 1962. 2: 421-5
3. Elsharkawy A, Ishii K, Niemelä M, Kivisaari R, Lehto H, Hernesniemi J. Management of aneurysms at the origin of duplicated middle cerebral artery: Series of four patients with review of the literature. World Neurosurg. 2013. 80: e313-8
4. Hori E, Kurosaki K, Matsumura N, Yamatani K, Kusunose M, Kuwayama N. Multiple aneurysms arising from the origin of a duplication of the middle cerebral artery. J Clin Neurosci. 2005. 12: 812-5
5. Kai Y, Hamada J, Morioka M, Yano S, Kudo M, Kuratsu J. Treatment of unruptured duplicated middle cerebral artery aneurysm: Case report. Surg Neurol. 2006. 65: 190-3
6. Kaliaperumal C, Jain N, McKinstry CS, Choudhari KA. Carotid “trifurcation” aneurysm: Surgical anatomy and management. Clin Neurol Neurosurg. 2007. 109: 538-40
7. Miyahara K, Fujitsu K, Ichikawa T, Mukaihara S, Okada T, Kaku S. Unruptured saccular aneurysm at the origin of the duplicated middle cerebral artery: Reports of two cases and review of the literature. No Shinkei Geka. 2009. 37: 1241-5
8. Nomura M, Yamashima T, Kita D, Kida S, Kajinami K, Yamashita J. Duplication of the middle cerebral artery associated with an unruptured aneurysm. Acta Neurochir (Wien). 2000. 142: 221-2
9. Toyota S, Kumagai T, Sugano H, Yamamoto S, Mori K, Taki T. Unruptured aneurysm at the origin of the duplicated middle cerebral artery treated by coil embolization: A case report. Open J Mod Neurosurg. 2015. 5: 27-33
10. Umansky F, Dujovny M, Ausman JI, Diaz FG, Mirchandani HG. Anomalies and variations of the middle cerebral artery: A microanatomical study. Neurosurgery. 1988. 22: 1023-7

