

- Department of Neurosurgery, Fukui Prefectural Hospital, Fukui, Japan.
Correspondence Address:
Katsuyoshi Miyashita, Department of Neurosurgery, Fukui Prefectural Hospital, Fukui, Japan.
DOI:10.25259/SNI_923_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Katsuyoshi Miyashita, Kosuke Nambu, Yu Shimizu, Yasuo Tohma. Blister-like aneurysm of the anterior communicating artery treated with only Low-profile Visualized Intraluminal Support Junior stent. 16-Nov-2021;12:564
How to cite this URL: Katsuyoshi Miyashita, Kosuke Nambu, Yu Shimizu, Yasuo Tohma. Blister-like aneurysm of the anterior communicating artery treated with only Low-profile Visualized Intraluminal Support Junior stent. 16-Nov-2021;12:564. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=11225
Date of Submission
12-Sep-2021
Date of Acceptance
21-Oct-2021
Date of Web Publication
16-Nov-2021
Abstract
Background: Endovascular treatment is becoming a mainstream treatment for blister-like aneurysms in recent years. Blister-like aneurysms are usually located in the internal carotid artery, whereas that of the anterior communicating artery (AcomA) are very rare. We report the first case of blister-like aneurysm of AcomA that was treated solely with a neck bridging stent that resulted in complete occlusion without complication.
Case Description: A 50- year- old woman was admitted to our hospital due to a subarachnoid hemorrhage. Digital subtraction angiography showed a very small aneurysm in the dorsal side of the AcomA. We considered it a blister-like aneurysm based on its size and shape. She underwent endovascular treatment under general anesthesia on day 15 after vasospasm period. Dual antiplatelet therapy was administrated 1 week prior. A Low-profile Visualized Intraluminal Support Junior stent was implanted from the left A2 to the right A1, covering the AcomA. The postoperative course was uneventful, and she was discharged with no neurological deficit. The aneurysm remained unchanged on postoperative day 14; however, complete occlusion was achieved 3 months after the treatment.
Conclusion: Monotherapy with a neck bridging stent is an effective treatment option for blister-like aneurysms. Treatment with a single stent could achieve complete occlusion especially if the aneurysms occur elsewhere than the internal carotid artery. We should consider immediate additional treatment if the aneurysm grows within 1 month after initial treatment.
Keywords: Anterior communicating artery, Blister- like aneurysm, Neck bridging stent
INTRODUCTION
Blister-like aneurysms are rare subtype that has the characteristics of a wide neck and dissecting appearance. They have a high tendency for perioperative rebleeding due to fragile walls. Most of the blister-like aneurysms are located in non-branching sites of the internal carotid artery.[
Blister-like aneurysms are treated with both microsurgery and endovascular surgery, while there is no optimal therapeutic strategy. In recent years, endovascular treatment is becoming the main approach of treatment for blister-like aneurysms due to the development of techniques and devices for endovascular treatment.[
Blister-like aneurysms of the AcomA are very rare with only ten previously reported cases [

CASE REPORT
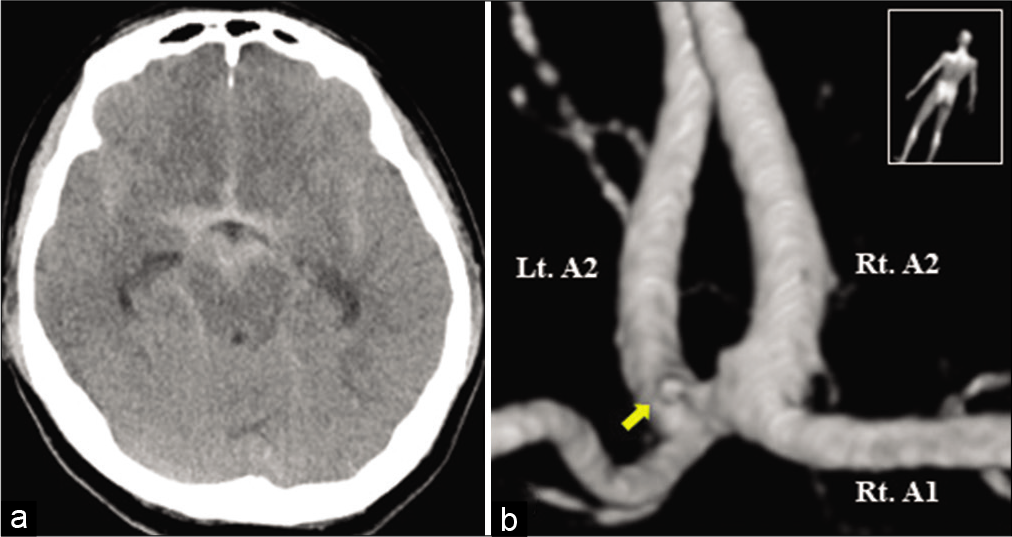
A 50-year-old woman was admitted to our hospital due to a sudden headache. Computed tomography demonstrated diffuse subarachnoid hemorrhage with no laterality [
Endovascular treatment was performed under general anesthesia at day 15. Dual antiplatelet therapy was administrated a week prior. A 6Fr Roadmaster (Goodman, Aichi, Japan) was placed in the right internal carotid artery with the administration of the systemic heparin. Headway 17 (Terumo, Tokyo, Japan) was delivered to the left A2, and 2.5 × 17 mm LVIS Jr. stent was implanted from the left A2 to the right A1 covering AcomA. The LVIS Jr. stent was deployed with wire pushing in order to avoid insufficient expansion. Sufficient expansion and patency of the stent were confirmed [
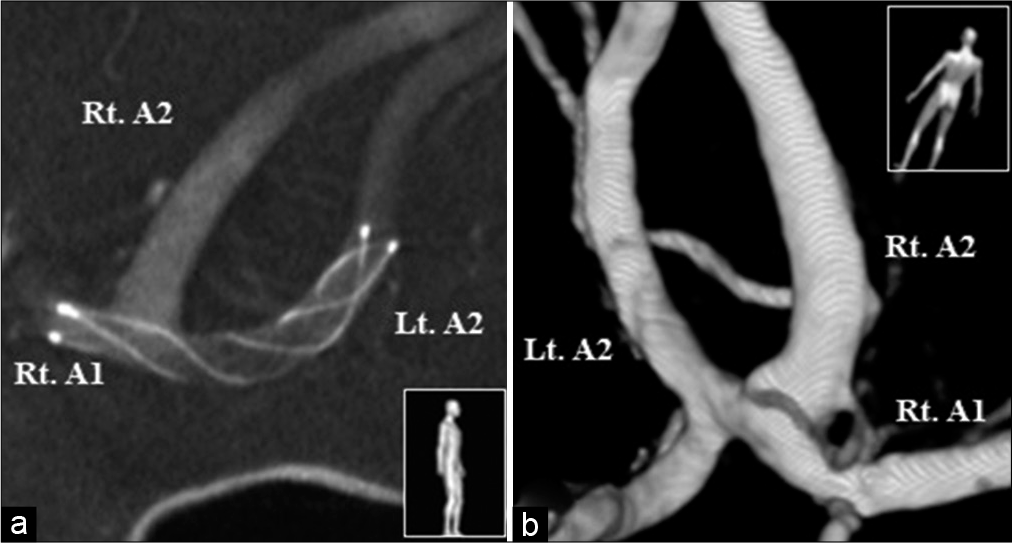
Figure 2:
Postoperative cone beam computed tomography showing the implanted Low-prolife Visualized Intraluminal Support Junior stent from the left A2 to the right A1 covering the anterior communicating artery (a). 3D- RA at 3 months after the treatment demonstrating complete occlusion of the aneurysm (b).
The postoperative course was uneventful and she was discharged with no neurological deficit at day 39 (postoperative day 24). DSA at postoperative day 14 showed that the aneurysm remained unchanged; however, complete occlusion was achieved 3 months after the treatment [
DISCUSSION
Endovascular treatments for blister-like aneurysms include stent-assisted coiling, stenting alone, and flow diversion.[
Metal coverage ratio of the stent is the most important factor in terms of the flow diversion effect. The approximate metal coverage ratio of the FD is 30%, while that of LVIS, LVIS Jr., Enterprise (Johnson and Johnson Codman, Miami, FL, USA), and Neuroform Atlas (Stryker, Fremont, CA, USA) is 23%, 18%, 11%, 12%, respectively.[
Another treatment option for blister-like aneurysms is direct surgery such as clipping and trapping. In AcomA aneurysms, the most critical concern is the preservation of the hypothalamic artery. Seven cases of AcomA blister-like aneurysm were treated by clipping and intraoperative rupture occurred in two cases among them [
CONCLUSION
This is the first report of a ruptured blister-like aneurysm of the AcomA treated solely with a stent. Monotherapy with stent for blister-like aneurysms might be an effective treatment with lower rate of complications than direct surgery. Complete occlusion could be expected for blister-like aneurysms with single stent occurring elsewhere than the internal carotid artery. We should consider immediate additional treatment if the aneurysms grow within 1 month after initial treatment.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Abiko T, Saito K, Murase M, Tomita H. Blister-like aneurysm originating from the anterior communicating artery: A case report. No Shinkei Geka. 2018. 46: 207-12
2. Andaluz N, Zuccarello M. Blister-like aneurysms of the anterior communicating artery: A retrospective review of diagnosis and treatment in five patients. Neurosurgery. 2008. 62: 807-11
3. Bulsara KR, Kuzmik GA, Hebert R, Cheung V, Matouk CC, Jabbour P. Stenting as monotherapy for uncoilable intracranial aneurysms. Neurosurgery. 2013. 73: ons80-85
4. Fiorella D, Albuquerque FC, Deshmukh VR, Woo HH, Rasmussen PA, Masaryk TJ. Endovascular reconstruction with the Neuroform stent as monotherapy for the treatment of uncoilable intradural pseudoaneurysms. Neurosurgery. 2006. 59: 291-300
5. Gaughen JR, Hasan D, Dumont AS, Jensen ME, McKenzie J, Evans AJ. The efficacy of endovascular stenting in the treatment of supraclinoid internal carotid artery blister aneurysms using a stent-in-stent technique. AJNR Am J Neuroradiol. 2010. 31: 1132-8
6. Grant RA, Quon JL, Bulsara KR. Oversized self-expanding stents as an alternative to flow-diverters for blister-like aneurysms. Neurol Res. 2014. 36: 351-5
7. Lim YC, Shin YS, Chung J. Flow Diversion via LVIS blue stent within enterprise stent in patients with vertebral artery dissecting aneurysm. World Neurosurg. 2018. 117: 203-7
8. Liu Q, Qi C, Zhang Y, Deng L, Li G, Su W. Low-profile visualized intraluminal support stent-only technique for intracranial aneurysms-a report of 12 cases with midterm follow-up. World Neurosurg. 2019. 129: e40-7
9. Monteiro A, Cortez GM, Aghaebrahim A, Sauvageau E, Hanel RA. Low-profile visualized intraluminal support Jr braided stent versus atlas self-expandable stent for treatment of intracranial aneurysms: A single center experience. Neurosurgery. 2021. 88: E170-8
10. Morris TC, Brophy BP. Blister-like aneurysm of the anterior communicating artery. J Clin Neurosci. 2009. 16: 1098-100
11. Peitz GW, Christopher AS, Grandhi R. Endovascular treatment of blister aneurysms. Neurosurg Focus. 2017. 42: E12
12. Peschillo S, Cannizzaro D, Caporlingua A, Missori P. A systematic review and meta-analysis of treatment and outcome of blister-like aneurysms. AJNR Am J Neuroradiol. 2016. 37: 856-61
13. Peschillo S, Cannizzaro D, Missori P, Colonnese C, Santodirocco A, Santoro A. Reconstructive endovascular treatment of a ruptured blood blister-like aneurysm of anterior communicating artery. J Neurosurg Sci. 2017. 61: 438-41
14. Peschillo S, Miscusi M, Caporlingua A, Cannizzaro D, Santoro A, Delfini R. Blister-like aneurysms in atypical locations: A single-center experience and comprehensive literature review. World Neurosurg. 2015. 84: 1070-9
15. Rouchaud A, Saleme S, Gory B, Ayoub D, Mounayer C. Endovascular exclusion of the anterior communicating artery with flow-diverter stents as an emergency treatment for blister-like intracranial aneurysms. A case report. Interv Neuroradiol. 2013. 19: 471-8
16. Seo DH, Lee WC, Choe IS, Park SC, Ha YS. Ruptured and unruptured aneurysms of the accessory anterior cerebral artery combined with a blood blister-like aneurysm of the anterior communicating artery. Neurol India. 2009. 57: 85-7
17. Shah SS, Gersey ZC, Nuh M, Ghonim HT, Elhammady MS, Peterson EC. Microsurgical versus endovascular interventions for blood-blister aneurysms of the internal carotid artery: Systematic review of literature and meta-analysis on safety and efficacy. J Neurosurg. 2017. 127: 1361-73
18. Walsh KM, Moskowitz SI, Hui FK, Spiotta AM. Multiple overlapping stents as monotherapy in the treatment of ‘blister’ pseudoaneurysms arising from the supraclinoid internal carotid artery: A single institution series and review of the literature. J Neurointerv Surg. 2014. 6: 184-94
19. Wang C, Tian Z, Liu J, Jing L, Paliwal N, Wang S. Flow diverter effect of LVIS stent on cerebral aneurysm hemodynamics: A comparison with Enterprise stents and the Pipeline device. J Transl Med. 2016. 14: 199

