

- Department of Neurosurgery, Hospital Central Sur de Alta Especialidad,
- Department of Anatomy, Faculty of Medicine, Universidad Nacional Autónoma de México,
- Department of Neurosurgery, Hospital Central Norte, Mexico City, Mexico.
Correspondence Address:
Daniel Alejandro Vega-Moreno, Department of Neurosurgery, Hospital Central Sur de Alta Especialidad, Mexico City, Mexico.
DOI:10.25259/SNI_697_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Daniel Alejandro Vega-Moreno1, Martha Elena González-Jiménez2, Víctor Andrés Reyes-Rodríguez3, Abraham Ibarra-de la Torre1, José Omar Santellán-Hernández1, Carlos Betancourt-Quiroz1, Julio César López-Valdés1, Andrés Alberto Moral-Naranjo1, Ulises García-González1. Case of anterolateral migration of herniated cervical disc fragment mimicking a spinal meningioma. 16-Aug-2021;12:415
How to cite this URL: Daniel Alejandro Vega-Moreno1, Martha Elena González-Jiménez2, Víctor Andrés Reyes-Rodríguez3, Abraham Ibarra-de la Torre1, José Omar Santellán-Hernández1, Carlos Betancourt-Quiroz1, Julio César López-Valdés1, Andrés Alberto Moral-Naranjo1, Ulises García-González1. Case of anterolateral migration of herniated cervical disc fragment mimicking a spinal meningioma. 16-Aug-2021;12:415. Available from: https://surgicalneurologyint.com/surgicalint-articles/11040/
Date of Submission
15-Jul-2021
Date of Acceptance
27-Jul-2021
Date of Web Publication
16-Aug-2021
Abstract
Background: Before the introduction of high-resolution MR, few disc fragments were misdiagnosed as meningiomas.
Case Description: A 63-year-old female presented with a 6-month history of mild to moderate pain in the left arm, weakness 4/5 in the left arm C5-C6 distribution, and a loss of the left biceps reflex response. Although the MR study was read as showing a C5-C6 level probable spinal meningioma, this proved to be a sequestrated disc fragment at surgery.
Conclusion: Rarely, cervical disc herniations may be misdiagnosed on MR studies as spinal meningiomas.
Keywords: Cervical spine, Discal herniation, Discal migration, Extradural tumor, Spinal meningioma
INTRODUCTION
Spinal meningiomas represent 7.8% of all meningiomas, and 35% are found in the cervical spine.[
CASE REPORT
A 63-year-old female presented with mild/moderate pain left arm pain, 4/5 weakness in the left C5-C6 distributions, and a decreased biceps reflex. The original MR was interpreted as a C5-C6 cervical meningioma (i.e. including the classical “dural tail” sign) [
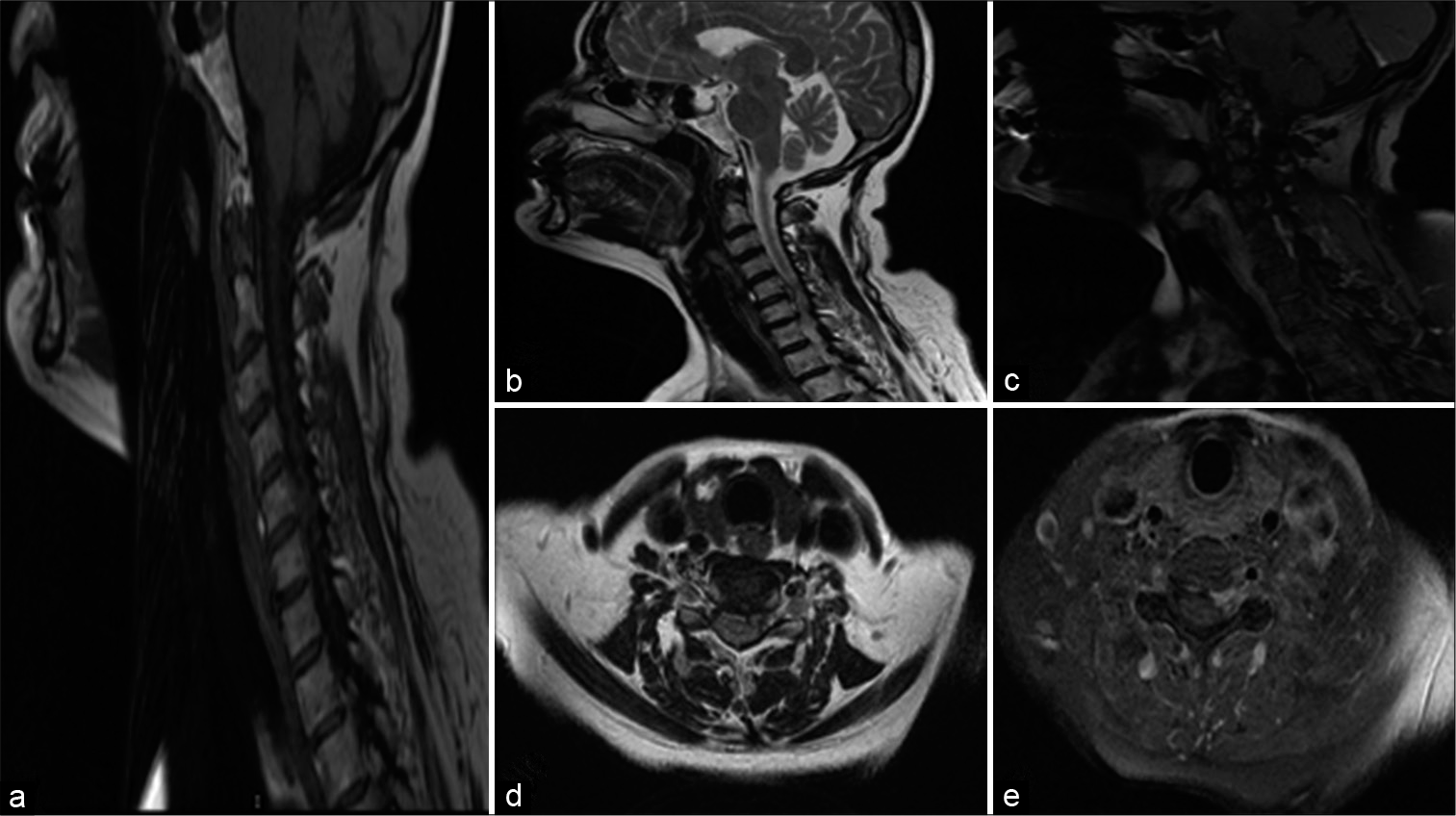
Figure 1:
(a) Sagittal T1 MR; hypo-isointense C5-C6 lesion (b) Sagittal T2 sequence hyperintense lesion intraspinal, extramedullary, extradural lesion. (c) Heterogeneous enhancement with “dural tail” sign. D. axial T2 hyperintense lesion projects toward left neuroforamen, compressing left C5 root. E. Contrast axial section, a poorly defined lesion is seen. Suspicion of spinal meningioma.
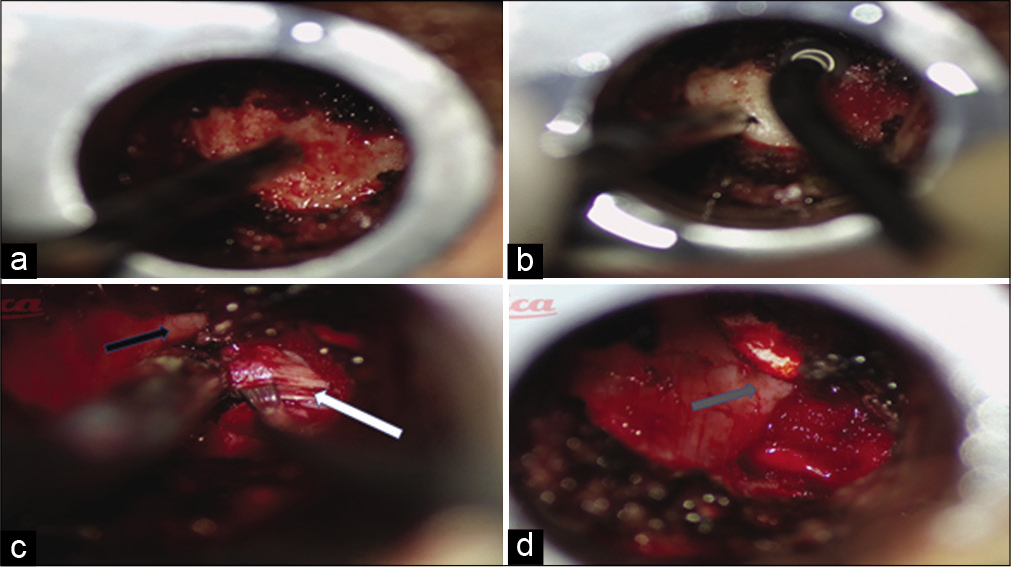
Figure 2:
(a) Left C5 lamina identified with minimally invasive tubular approach. (b) Left C5 hemilaminectomy performed. With diamond burr. (c) Black arrow, Spinal root of C5 separated with a hook. White arrow, showed axilla of C5 root compressed by soft, vascularized, gray/whitish lesion. (d) Spinal root C5 released (Gray arrow).
DISCUSSION
Migration of epidural herniated cervical disc fragments is rare and must be differentiated in some instances from spinal meningiomas.[
Further, on occasion, contrast-enhanced MR studies of sequestrated disc fragments may demonstrate peripheral/diffuse enhancement that mimics the “dural tail sign” seen with extradural meningiomas classical for meningiomas.[
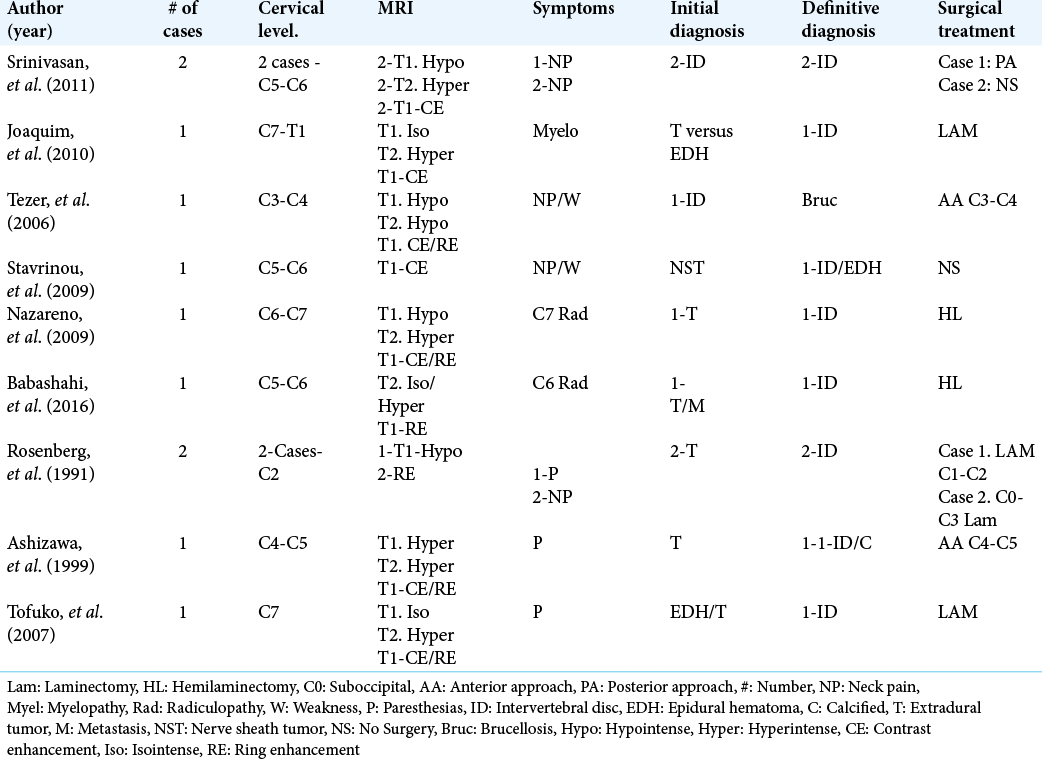
Literature on sequestrated cervical discs
In multiple studies, sequestrated extradural/ extramedullary cervical disc fragments may closely resemble spinal meningiomas.[
CONCLUSION
On occasion, sequestrated epidural cervical disc herniations may migrate and imitate intra-spinal meningiomas or other tumors on MR studies performed with/without contrast. Here, surgical intervention readily differentiated between a cervical disc herniation versus meningioma/other neoplasm.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Babashahi A, Taheri M. The cervical sequestrated disc fragment presenting as mass lesion: Case report and review of the literature. Iran J Neurosurg. 2016. 2: 24-9
2. Ciftdemir M, Kaya M, Selcuk E, Yalniz E. Tumors of the spine. World J Orthop. 2016. 7: 109-16
3. Elsharkawy AE, Hagemann A, Klassen PD. Posterior epidural migration of herniated lumbar disc fragment: A literature review. Neurosurg Rev. 2019. 42: 811-23
4. Lai CY, Salkade PR, Chuah KL, Sitoh YY. Extradural cervical spinal meningioma mimicking malignancy. Radiol Case Rep. 2018. 12: 1-10
5. Lombardi V. Lumbar spinal block by posterior rotation of anulus fibrosus: Case report. J Neurosurg. 1973. 39: 642-4
6. Srinivasan US, Kumar GS, Mahesha KB. Posterior epidural migration of sequestrated cervical disc fragment: Case series. Asian Spine J. 2011. 5: 220-7
7. Vega-Moreno DA, Santellán-Hernández JO, VelázquezDomínguez HE, Martínez-Nava AO, Vicuña-González RM, Mendoza-Trillo PR. Histopathological correlation (World Health Organization classification) of meningiomas and their anatomical localization: A multicenter epidemiological study in Mexico. World Neurosurg. 2021. 151: e888-98

